Download presentation
Presentation is loading. Please wait.

1
Scrotal disorders Dr.Saad Dakhil

2
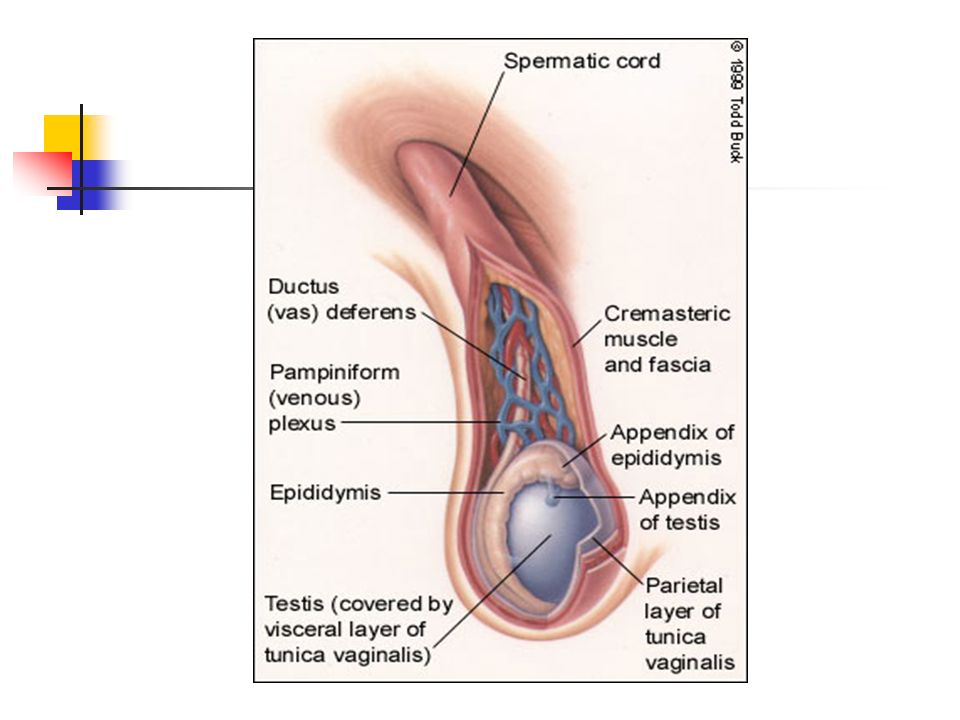
Anatomy; Scrotum;can be considered as an outpouching of the lower part of the anterior abdominal wall.it contains the Testis,Epididymides,lower end of spermatic cord

4
Spermatic cord Structure of spermatic cord ; 1-vas deferens
2-testicular artery 3- testicular veins (pampiniform plexus) 4-testicular lymph vessels 5-autonomic nerves 6-processus vaginalis 7-cremasteric artery 8-artery of the vas deferens 9-genital branch of the genitofemoral nerve
 4-testicular lymph vessels. 5-autonomic nerves. 6-processus vaginalis. 7-cremasteric artery. 8-artery of the vas deferens. 9-genital branch of the genitofemoral nerve.")
5
Scrotal Swellings Cystic Solid Neither varicocele Hernia Epididymal
Tumor (benign/ Malignant) varicocele Hernia Hydrocele Epididymal cyst/ spermatocele Hematocele
 varicocele. Hernia. Hydrocele. Epididymal. cyst/ spermatocele. Hematocele.")
6
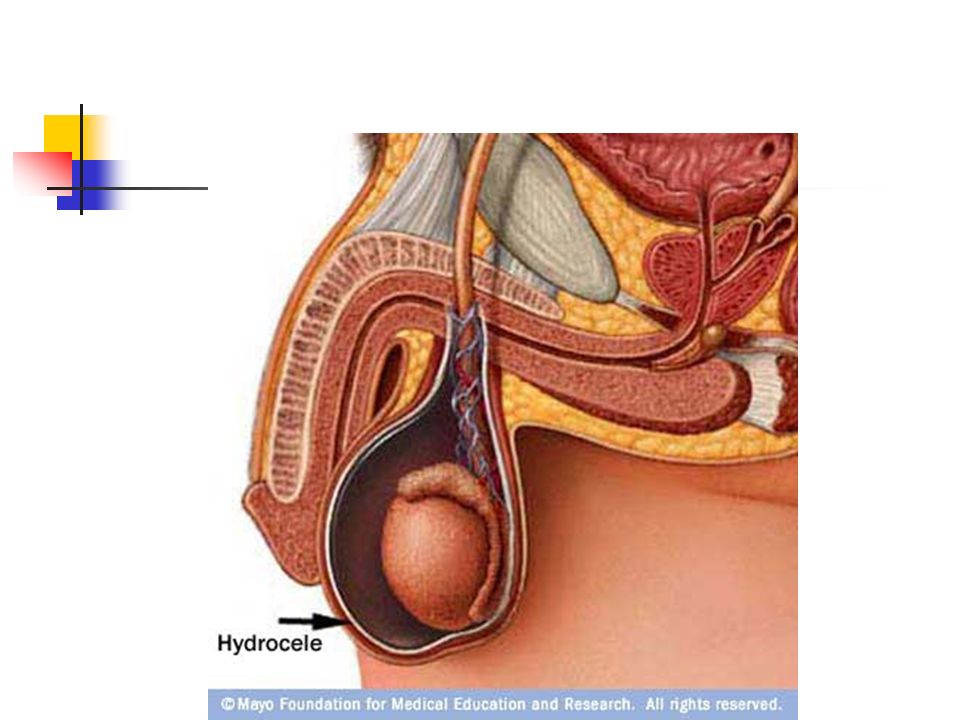
Hydrocele; Collection of abnormal quantity of serous fluid in the tunica vaginalis. If it contains pus or blood it is called pyocele or haematocele respectively. Hydrocele is more common than the two other varieties.

8
Hernia / Hydrocele Hydrocele: incomplete obliteration of the processus vaginalis Hernia: large opening of the processus vaginalis which may allow abdominal contents to enter scrotal sac.

9
Scrotal Ultrasound Large left hydrocele

10
Cont; Causes; 1-primary;cause unknown associate with patency of proccessus vaginalis. It classified as follows; 1-communicating;it connect with the peritoneal cavity. 2-noncommunicating;it dose not connect with peritoneal cavity.

11
Cont; 2- Secondary; where the fluid accumulate secondary to pathology inside the testis like epididymo-orchitis,testicular tumor and trauma.

12
Clinical presentation;
Symptoms; 1-painless swelling 2-embarrassment 3-frequent and painful micturation may occur if hydrocele is secondary to epididymo-orchitis Hydrocele not affect fertility

13
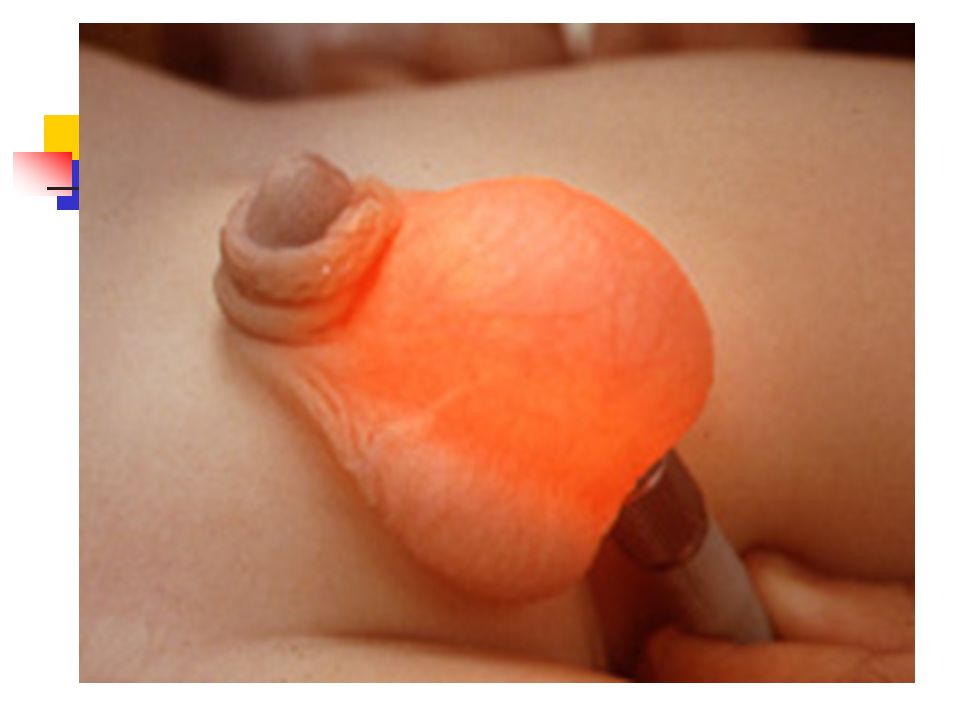
Cont; Examination; Position; the swelling usually unilateral but can be bilateral .if communicating can not feel the cord above the lump. Colour and temperature; normal Tenderness; primary are not tender but secondary may be tender Composition; fluctuant and have fluid thrill if large enough Reducibility; can not reduced Testis impalpable and transillumenate

15
Mangement; Primary; in children:
most neonatal hydrocel resolve in first 2 year of life if persists repair as herniotomy.(communicating). The scrotal approach (Lord or Jaboulay technique) is used in the treatment of a secondary non-communicating hydrocele.
. The scrotal approach (Lord or Jaboulay technique) is used in the treatment of a secondary non-communicating hydrocele.")
16
Cont; In adult; surgical excision. Secondary :
treatment the underlying condition.

17
ACUTE SCROTUM IN CHILDREN
A child or adolescent with acute scrotal pain, tenderness, or swelling should be looked on as an emergency situation requiring prompt evaluation, differential diagnosis, and potentially immediate surgical exploration.

18
Painful scrotal swellings

19
Causes Testicular Torsion Epididmyo-orchitis

20
Is it torsion or not Adolescent Children Gradual Sudden present absent
By History Epidimyo-orchitis Testicular torsion Adolescent Children Gradual Sudden present absent Age Onset Fever

21
Epidimyo-orchitis Testicular torsion
moderate Sever present absent Severity Irritative symptoms

22
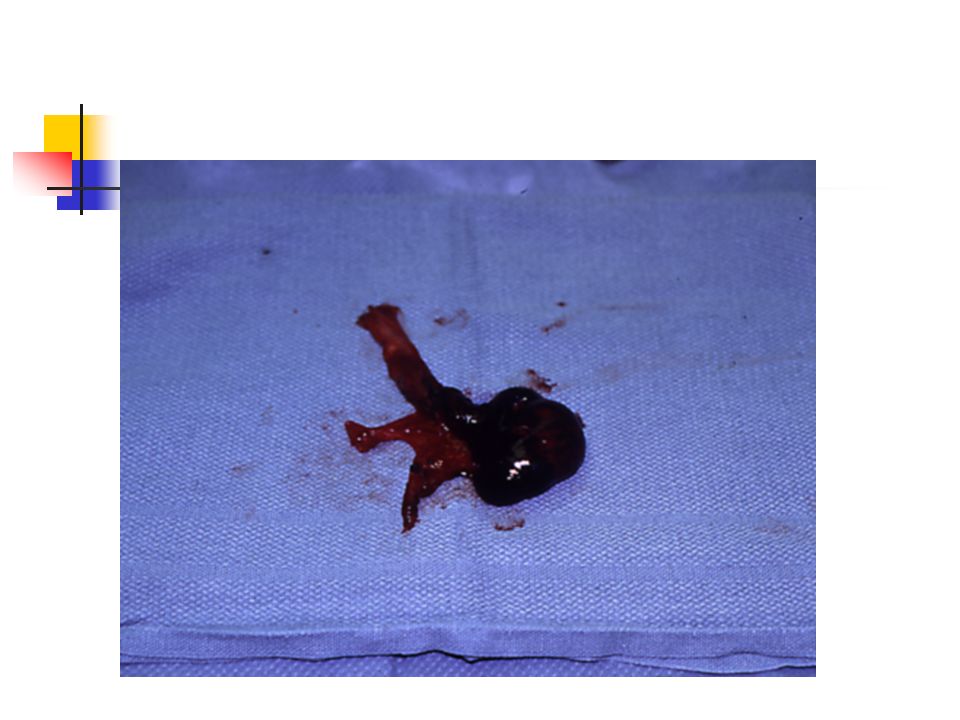
Testicular Torsion The most urgent problem.
High risk of loss due to infarction (90%) May have torsion of cord or appendages Neonatal and adolescence more common in undescended testes due to absence of fixation Extravaginal: exclusive to perinatal Intravaginal: 90% of adolescent age group
 May have torsion of cord or appendages. Neonatal and adolescence. more common in undescended testes due to absence of fixation. Extravaginal: exclusive to perinatal. Intravaginal: 90% of adolescent age group.")
23
Extravaginal Torsion

24
Intravaginal Torsion

25
Testicular Torsion History Physical Sudden onset of pain
Past history of similar pain in 50% Physical Cremasteric reflex may be absent Prehn’s sign: elevation of testes does not relieve pain lateral testicular lie.

26
Testicular Torsion Diagnosis if certain : emergent surgery
if uncertain: Nuclear scan: not done often depending on facility Ultrasonography: documents blood flow PROVIDES ANATOMY

27
Testicular Torsion Refer Emergently! Attempt manual detorsion- outward
< 6 hours, 90% salvage > 24 hours, 100% loss and atrophy Attempt manual detorsion- outward “ open the book “ Some may be twisted 360, 720 degrees

30
Testicular Appendages
Appendix testis Appendix epididymis

31
Testicular Appendages
Torsion of appendages rarely seen after puberty Presents with pain Physical may develop scrotal swelling & erythema “blue dot sign” seen early Ultrasound required to rule out testis torsion Treat symptomatically Be sure of early exam before swelling makes any further exam suspect!

32
Torsion of Appendix Testis
Blue dot of gangrenous appendix testis

34
Epididymitis Most common acute scrotum post-pubertal
Gradual onset of pain Fever in 40% of patients Dysuria in 50% of patients Urinalysis may show pyuria in 50%

35
Doppler Epididymitis Left Epididymitis Increased blood flow

36
Epididymitis Confirm that torsion of testis does not exist Treatment
scrotal elevation Antibiotics considered: keflex, septra Refer for persistence of pain/swelling.

37
CRYPTORCHIDISM Background
Almost 1% of all full-term male infants are affected at the age of one year. Categorisation into palpable and non-palpable testis seems to be most the appropriate method.

38
Iliac fossa 3rd-5th month Deep inguinal ring 7th month
Empty Scrotum Iliac fossa rd-5th month Deep inguinal ring 7th month Superficial ring th month Scrotum th month

39
Higher incidence of: Complications (THIN)
Empty Scrotum Complications (THIN) Higher incidence of: Cancer times increased risk. not affected by orchiopexy. Infertility. 50% abnormal semen in unilat. UDT 70% in bilateral. Testicular torsion. Trauma. Hernia
 Higher incidence of: Cancer times increased risk. not affected by orchiopexy. Infertility. 50% abnormal semen in unilat. UDT. 70% in bilateral. Testicular torsion. Trauma. Hernia.")
40
Assessment A physical examination is the only method of differentiating between palpable or non-palpable testes. Radiological imaging: 44% There is no reliable examination to confirm or rule out an intra-abdominal, inguinal and absent/vanishing testis (nonpalpable testis), except for diagnostic laparoscopy.
, except for diagnostic laparoscopy.")
41
Assessment In cases of bilateral non-palpable testes and any suggestion of sexual differentiation problems, urgent endocrinological and genetic evaluation is mandatory.

42
Treatment To prevent histological deterioration, treatment should be undertaken and completed before the age of months. Medical therapy Medical therapy using human chorionic gonadotrophin (hCG) or gonadotrophin-releasing hormone (GnRH) is based on the hormonal dependence of testicular descent, with success rates of a maximum of 20%.
 or gonadotrophin-releasing hormone (GnRH) is based on the hormonal dependence of testicular descent, with success rates of a maximum of 20%.")
43
Surgery Palpable testis:
Surgery for the palpable testis includes orchidofuniculolysis and orchidopexy, with success rates of up to 92%. Non-palpable testis: Inguinal surgical exploration with the possibility of performing laparoscopy should be attempted. Laparoscopy is the most appropriate way of examining the abdomen for a testis. Microvascular autotransplantation is also an option.

44
Laparoscopy

45
perineal prepenile. femoral. inguinal pouch. Ectopic Testes
Empty Scrotum Ectopic Testes perineal prepenile. femoral. inguinal pouch. Vs undescended?

46
normal size & consistency scrotum well developed.
Empty Scrotum Retractile Testes functions normally. normal size & consistency scrotum well developed. ? Hyperactive cremasteric reflex. most are normal by 12 yrs.

47
Atrophied Testes ? - Trauma. - Torsion. - Infection.
Empty Scrotum Atrophied Testes ? - Trauma. - Torsion. - Infection. - Previous inguinal surgery.

48
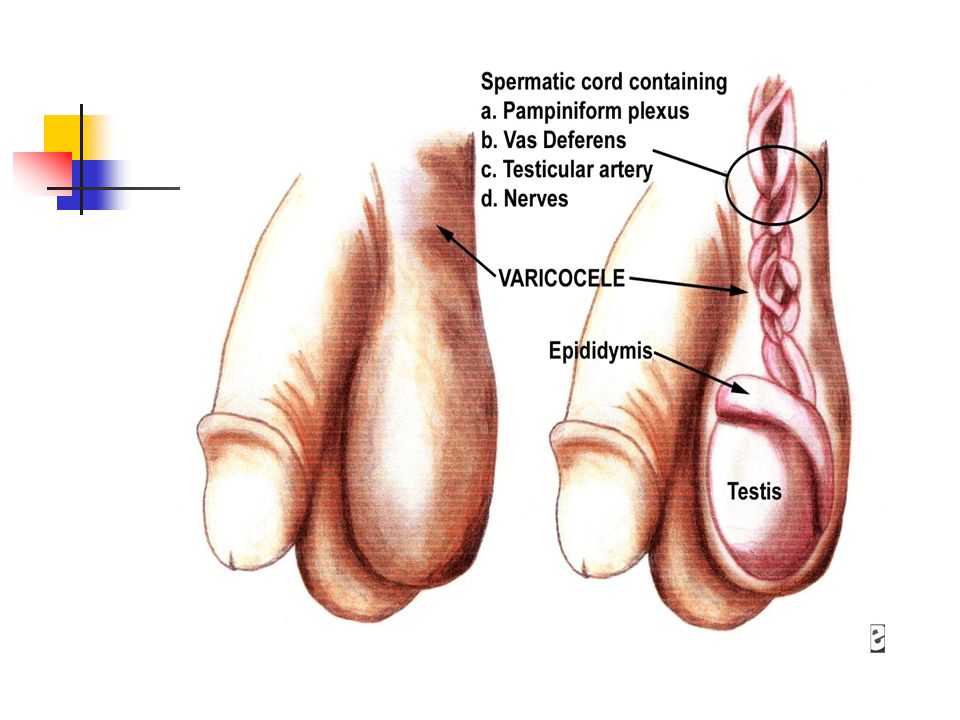
VARICOCELE Background
Ectatic and tortuous veins of the pampiniform plexus of the spermatic cord are found in approximately 15% of male adolescents, with a marked left-sided predominance . This is unusual in boys under 10 years of age, but becomes more frequent at the beginning of puberty. Fertility problems will arise in about 20% of adolescents with varicocele. The adverse influence of varicocele increases with time.

50
Assessment

51
Treatment Surgery Surgical intervention is based on ligation or occlusion of the internal spermatic veins. Microsurgical lymphatic-sparing repair (microscopic or laparoscopic) are associated with the lowest recurrence and complication rate. Follow-up During adolescence, testicular size should be checked annually. After adolescence, repeated sperm analysis is to be recommended.
 are associated with the lowest recurrence and complication rate. Follow-up. During adolescence, testicular size should be checked annually. After adolescence, repeated sperm analysis is to be recommended.")
52
The potential complications of varicocelectomy
hydrocele formation, varicocele recurrence and testicular infarction (atrophy). Hydrocele formation is related to failure to preserve the lymphatic vessels associated with the spermatic cord.
. Hydrocele formation is related to failure to preserve the lymphatic vessels associated with the spermatic cord.")
53
Testicular tumors Commonest malignancy in men < 35 years.
Rare in african men and before puberty. Peaks in the early twenties. One in 10 testicular tumors occurs in association with maldescent of the testis. Prognosis is good particularly if there was no lymph node involvement.

54
Classification According to the cells of origin, they’re classified into: Primary cell tumors (90-95%), which include: Germ cell tumors: Seminoma, teratoma,Embryonal CA, Yolk Sac Tumor. Non-germ cells tumors: like sertoli cells tumors, Lyedig cell tumor. 2. Secondary tumors: lymphoma, leukemic infiltration of the testes.

55
Germ cell tumors 1. Seminomas - 40% (a) Classic Typical Seminoma
(b) Anaplastic Seminoma (c) Spermatocytic Seminoma 2. Embryonal Carcinoma % 3. Teratoma % (a) Mature (b) Immature 4. Choriocarcinoma - 1% 5. Yolk Sac Tumour
 Anaplastic Seminoma. (c) Spermatocytic Seminoma. 2. Embryonal Carcinoma % 3. Teratoma % (a) Mature. (b) Immature. 4. Choriocarcinoma - 1% 5. Yolk Sac Tumour.")
56
Clinical features Painless Swelling of One testis
Dull Ache or Heaviness in Lower Abdomen 10% - Acute Scrotal Pain 10% - Present with Metatstasis - Neck Mass / Cough / Anorexia / Vomiting / Back Ache/ Lower limb swelling 5% - Gynecomastia Rarely - Infertility

57
Physical Examination Examine contralateral normal testis.
Firm to hard fixed area within tunica albugenia is suspicious. Seminoma expand within the testis as a painless, rubbery enlargement. Embryonal carcinoma or teratocarcinoma may produce an irregular, rather than discrete mass.

58
Differential Diagnosis
Testicular torsion Epididymitis, or epididymo-orchitis Hydrocele, Hernia, Hematoma, Spermatocele, Syphilitic gumma .

59
DICTUM FOR ANY SOLID SCROTAL SWELLINGS
All patients with a solid, Firm Intratesticular Mass that cannot be Transilluminated should be regarded as Malignant unless otherwise proved.

60
Tumor markers TWO MAIN CLASSES Onco-fetal Substances : AFP & HCG
Cellular Enzymes : LDH & PLAP AFP - Trophoblastic Cells HCG - Syncytiotrophoblastic Cells ( PLAP- placental alkaline phosphatase, & LDH lactic acid dehydrogenase)
")
61
ROLE OF TUMOUR MARKERS Degree of Marker Elevation Appears to be Directly Proportional to Tumor Burden Markers indicate Histology of Tumor: If AFP elevated in Seminoma - Means Tumor has Non-Seminomatous elements Negative Tumor Markers becoming positive on follow up usually indicates - Recurrence of Tumor Markers become Positive earlier than X-Ray studies

62
Investigation: US testis CXR metastasis CT scan abdomen and chest to identify lymph nodes and pulmonary mets Tumor markers :AFP (yolk-sac cell), βHCG (trophoblastic cells).
, βHCG (trophoblastic cells).")
63
Tumor staging Primary Tumor (T)pTX - Primary tumor cannot be assessed . pT0 - No evidence of primary tumor. pTis - Intratubular germ cell neoplasia. pT1 - Tumor limited to the testis and epididymis. pT2 - Tumor limited to the testis and epididymis with vascular/lymphatic invasion or tumor extending through the tunica albuginea with involvement of tunica vaginalis pT3 - Tumor invades the spermatic pT4 - Tumor invades the scrotum

64
Regional Lymph Nodes Clinical NX - Regional lymph nodes cannot be assessed N0 - No regional lymph node metastasis N1 - Lymph node mass 2 cm or less in greatest dimension. N2 - Lymph node mass, more than 2 cm but not more than 5 cm in greatest dimension. N3 - Lymph node mass more than 5 cm in greatest dimension

65
Distant metastasis M0 - No evidence of distant metastases
M1 - Nonregional nodal or pulmonary metastases M2 - Nonpulmonary visceral masses

66
Serum tumor markers LDH HCG Miu/ml AFP Ng/ml S0 < N <N S1
<1.5 x N < 5000 < 1000 S2 1.5-10x N 5000 to 1000 to 10000 S3 >10x N > 50000 >10000

67
Treatment: Explore testis through an inguinal incision.
Radical Orchidectomy. Further treatments depends on the type and stage ( see Table) . Chemotherapy regimen : BEP :Bleomycine , Etopside ,Cisplatine DXT=deep x-ray therapy, RPLND=retroperitoneal lymph node dissection
 . Chemotherapy regimen : BEP :Bleomycine , Etopside ,Cisplatine. DXT=deep x-ray therapy, RPLND=retroperitoneal lymph node dissection.")
68
Staging Treatment of seminoma Stage I
. Staging Treatment of seminoma Treatment of non-seminomatous germ cell tumor Stage I confined to the testis DXT to the abdominal nodes or single agent carboplatine chemo therapy Observation or RPLND Or primary chemotherapy Stage II Retroperitolneal LN involvement II a : nodes <2cm II b : nodes 2-5cm II c : nodes >5cm DXT to abdominal nodes. or Chemotherapy Chemo & RPLND of residual tumor Stage III nodal dx above the diaphragm DXT to abdominal wall & thoracic nodes or chemo therapy Stage IV visceral metastasis

69
Fournier’s Gangrene Necrotizing fasciitis of the perineum
May ascend of fascial planes Colles > Dartos > Scarpas 20% to 50% Mortality Rate Polymicrobial infection Treat with Gent, Pen G and Flagyl Debridement surgically

71
Thank you

Similar presentations





: Gary Faerber, M.D., 2011>")








; FRCS (Ireland); MMed (Wits); FCS (SA) Urology 38 th BMA CONGRESS.>")





