Download presentation
Presentation is loading. Please wait.

1
INFANTS OF DIABETIC MOTHERS MUHAMMAD ALI Cardiology Division Department of Child Health University of Sumatera Utara

2
Prevalence At least 1.3% of pregnancies are complicated by diabetes mellitus. Pathology The teratogenic action of DM is generalized, affecting multiple organ systems. The prevalence of major congenital malformations in infants of diabetic mothers is as high as 6% to 9% (i.e., three to four times that found in the general population). Congenital malformations of all types are increased in infants of diabetic mothers, but neural tube defects (anencephaly, myelomeningocele), CHDs, and sacral dysgenesis or agenesis are common. Infants born to insulin-dependent diabetic mothers are at highest risk for developing congenital malformations; infants born to mothers with non-insulin-dependent, well-controlled diabetes do not appear to have an increased risk of congenital malformations
. Congenital malformations of all types are increased in infants of diabetic mothers, but neural tube defects (anencephaly, myelomeningocele), CHDs, and sacral dysgenesis or agenesis are common. Infants born to insulin-dependent diabetic mothers are at highest risk for developing congenital malformations; infants born to mothers with non-insulin-dependent, well-controlled diabetes do not appear to have an increased risk of congenital malformations.")
3
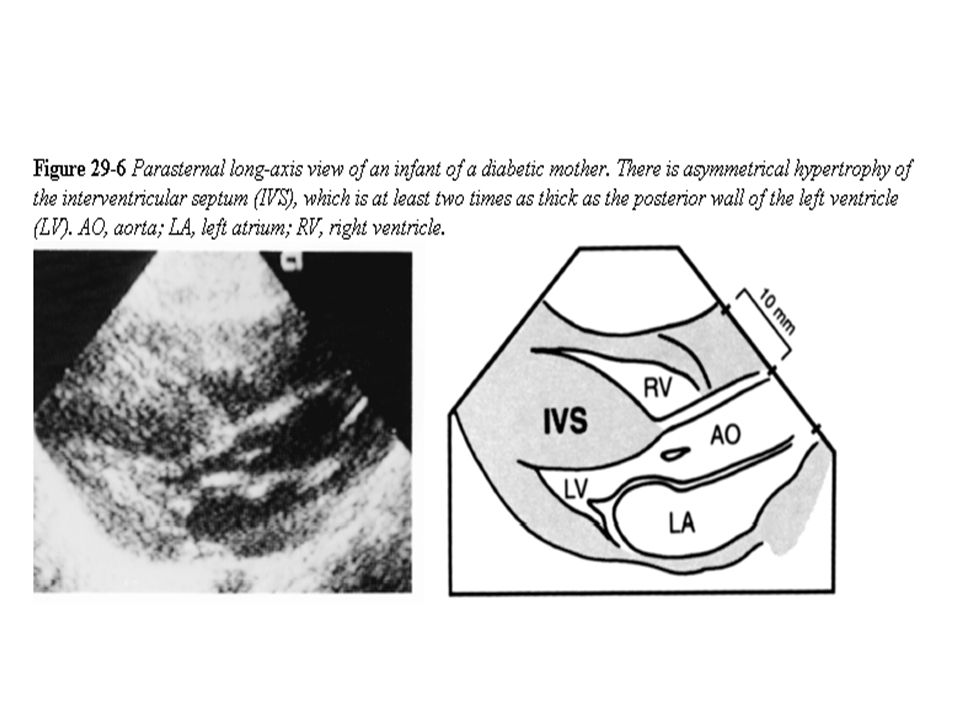
Infants of diabetic mothers have a high prevalence of CHDs, cardiomyopathy, and PPHN. The risk of CHD is three to four times greater than that in the general population, with VSD, TGA, and COA among the more common defects. Hypertrophic cardiomyopathy with or without obstruction is seen in 10% to 20% of these infants. The weight of the heart is increased by the increased myocardial fiber size and number (rather than by excess glycogen, as once thought); the hypertrophy is thought to be caused by hyperinsulinemia. Although free walls of both ventricles and the ventricular septum are hypertrophied, the ventricular septum characteristically is more hypertrophied than the LV posterior wall (asymmetrical septal hypertrophy) Infants of diabetic mothers also have an increased risk of PPHN. They often are affected by conditions that promote the persistence of pulmonary hypertension, such as hypoglycemia, perinatal asphyxia, respiratory distress, and polycythemia
; the hypertrophy is thought to be caused by hyperinsulinemia. Although free walls of both ventricles and the ventricular septum are hypertrophied, the ventricular septum characteristically is more hypertrophied than the LV posterior wall (asymmetrical septal hypertrophy) Infants of diabetic mothers also have an increased risk of PPHN. They often are affected by conditions that promote the persistence of pulmonary hypertension, such as hypoglycemia, perinatal asphyxia, respiratory distress, and polycythemia.")
5
Clinical Manifestations The history usually reveals gestational or insulin-dependent DM in the mother. The patient often has a history of progressive respiratory distress with tachypnea (80 to 100 breaths/minute) from birth. These large for gestational age babies often are plethoric and mildly cyanotic and may have tachypnea and tachycardia (>160 beats/minute). Signs of CHF with gallop rhythm may be found in 5% to 10% of these babies. The patient may have a systolic murmur along the left sternal border, which may be caused by an outflow tract obstruction or an associated defect. Chest x-ray films may reveal a varying degree of cardiomegaly. Pulmonary vascular markings are normal or mildly increased due to pulmonary venous congestion.
 from birth. These large for gestational age babies often are plethoric and mildly cyanotic and may have tachypnea and tachycardia (>160 beats/minute). Signs of CHF with gallop rhythm may be found in 5% to 10% of these babies. The patient may have a systolic murmur along the left sternal border, which may be caused by an outflow tract obstruction or an associated defect. Chest x-ray films may reveal a varying degree of cardiomegaly. Pulmonary vascular markings are normal or mildly increased due to pulmonary venous congestion..")
6
The ECG usually is nonspecific, but a long QT interval caused by a long ST segment of hypocalcemia may be found. Occasionally, RVH, LVH, or combined ventricular hypertrophy (CVH) may be seen. Echo may show the following: –The ventricular septum often is disproportionately thicker than the LV posterior wall, but even free walls are thicker than normal. The degree of asymmetrical septal hypertrophy has no relationship to the severity of the maternal diabetes. –Supernormal contractility of the LV and evidence of left ventricular outflow tract obstruction (systolic anterior motion of the mitral valve and fluttering of the aortic valve) appear in about 50% of these infants. –Rarely, the LV is dilated, and its contractility is decreased.
 may be seen. Echo may show the following: –The ventricular septum often is disproportionately thicker than the LV posterior wall, but even free walls are thicker than normal. The degree of asymmetrical septal hypertrophy has no relationship to the severity of the maternal diabetes. –Supernormal contractility of the LV and evidence of left ventricular outflow tract obstruction (systolic anterior motion of the mitral valve and fluttering of the aortic valve) appear in about 50% of these infants. –Rarely, the LV is dilated, and its contractility is decreased..")
7
Management General supportive measures are provided, such as intravenous fluids correction of hypoglycemia and hypocalcemia, and ventilatory assistance, if indicated. In most cases, the hypertrophy spontaneously resolves within the first 6 to 12 months of life. β-Adrenergic blockers, such as propranolol, may help the left ventricular outflow tract obstruction, but treatment usually is not necessary. Digitalis and other inotropic agents are contraindicated because they may worsen the obstruction. If the LV is dilated with decreased LV contractility, the usual anticongestive measures (e.g., digoxin, diuretics) are indicated.
 are indicated..")
8
THANK YOU

Similar presentations



, tachycardia (170) and “dusky” in appearance.>")









The following personal financial relationships with commercial interests relevant to this presentation existed during the past.>")





