Download presentation
Presentation is loading. Please wait.

1
abnormal PSYCHOLOGY Fourth Canadian Edition Chapter 6 Anxiety Disorders Prepared by: Tracy Vaillancourt, Ph.D. Modified by: Réjeanne Dupuis, M.A.

2
Types of Anxiety Disorders Phobias Panic Disorder (PD) Generalized Anxiety Disorder (GAD) Obsessive-Compulsive Disorder (OCD) Post-Traumatic Stress Disorder (PTSD) Acute Stress Disorder
 Generalized Anxiety Disorder (GAD) Obsessive-Compulsive Disorder (OCD) Post-Traumatic Stress Disorder (PTSD) Acute Stress Disorder")
3
Anxiety Disorders Anxiety: the unpleasant feeling of fear and apprehension Anxiety disorders tend to be comorbid The most common psychological disorders in Canada (2006)
")
4
Prevalence In Ontario (one year) 16% of women and 9% of men suffered from anxiety disorders highest one-year prevalence rates found in women 15 to 24 years of age In U.S. 12% in university students for 12-month prevalence 80% of them do not seek treatment In Canada (lifetime prevalence) PTSD at 9.2% Social anxiety disorder at 8.1% Anxiety disorders are more common in women than in men across all age groups and decrease with age
 PTSD at 9.2% Social anxiety disorder at 8.1% Anxiety disorders are more common in women than in men across all age groups and decrease with age.")
5
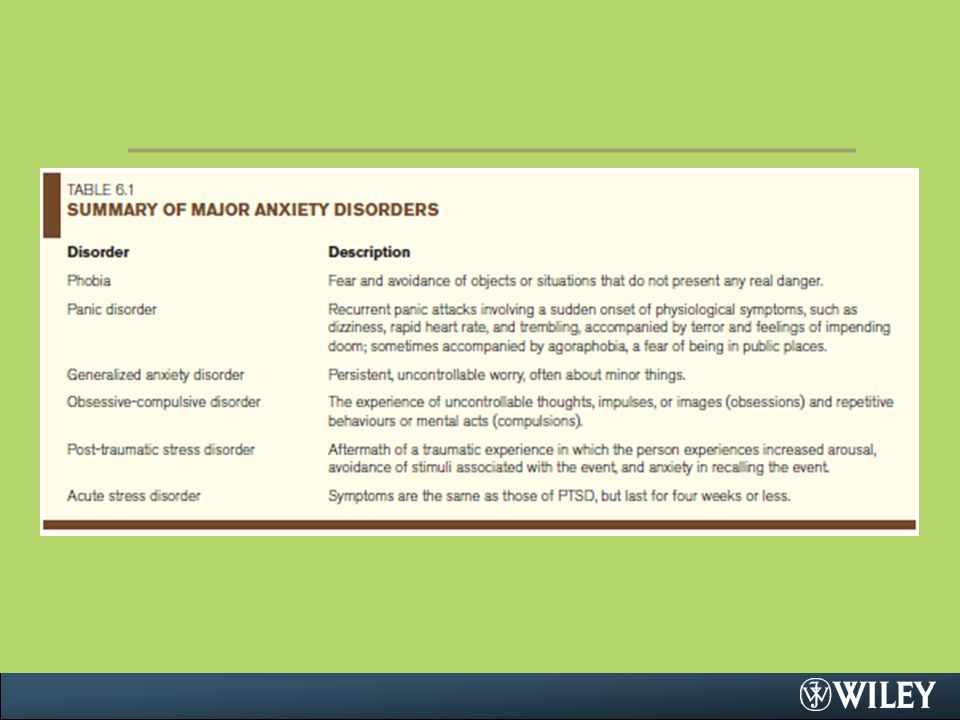
Summary: Table 6.1 DisorderDescription PhobiaFear and avoidance of objects or situations that do not present any real danger. Panic DisorderRecurrent panic attacks involving a sudden onset of physiological symptoms, such as dizziness, rapid heart rate, and trembling, accompanied by terror and feelings of impending doom; sometimes accompanied with agoraphobia, a fear of being in public places. Generalized Anxiety DisorderPersistent, uncontrollable worry, often about minor things. Obsessive-Compulsive DisorderThe experience of uncontrollable thoughts, impulses, or images (obsessions) and repetitive behaviours or mental acts (compulsions). Post-traumatic Stress DisorderAftermath of a traumatic experience in which the person experiences increased arousal, avoidance of stimuli associated with the event, and anxiety in recalling the event. Acute Stress DisorderSymptoms are the same as those of post-traumatic stress disorder, but last for four weeks or less.
 and repetitive behaviours or mental acts (compulsions). Post-traumatic Stress DisorderAftermath of a traumatic experience in which the person experiences increased arousal, avoidance of stimuli associated with the event, and anxiety in recalling the event. Acute Stress DisorderSymptoms are the same as those of post-traumatic stress disorder, but last for four weeks or less..")
7
Phobias Phobia—disrupting, fear-mediated avoidance that is out of proportion to the danger actually posed and is recognized by the sufferer as groundless Examples of common phobias –Claustrophobia: fear of closed spaces –Agoraphobia: fear of public places –Acrophobia: fear of heights. –Ergosiaphobia: fear of working –Mysophobia: fear of contamination and dirt

8
Specific Phobias Specific phobias— unwarranted fears caused by the presence or anticipation of a specific object or situation Phobias sub-divided according to source of fear: –Blood, injuries, and injections –Situations (e.g., planes, elevators, enclosed spaces) –Animals –Natural environment (e.g., heights, water) Evidence to support the grouping of fears into 5 factors: 1. Agoraphobia 2. Fears of heights or water 3. Threat fears (e.g., blood/needles, storms/thunder) 4. Fears of being observed 5. Speaking fears
 4. Fears of being observed 5. Speaking fears.")
9
Social Phobia (SP) Social phobias— persistent, irrational fears linked generally to the presence of other people. –Can be extremely debilitating –People with a SP try to avoid situations in which they might be evaluated because they fear that they will reveal signs of anxiousness or behave in an embarrassing way Examples: –Speaking or performing in public –Eating in public –Using public lavatories

10
Social Phobias (cont.) Social phobias can be either generalized or specific –Generalized SP involve many different interpersonal situations –Specific SP involve intense fear of one particular situation (e.g., public speaking). Generalized SP has an earlier age of onset and is more often comorbid with other disorders than specific SP Lifetime prevalence in Canada –7.5% in men –8.7% in women

11
Etiology of Phobias Behavioural Theories –Focus on learning as the way in which phobias are acquired –Several types of learning may be involved Avoidance Conditioning— reactions are learned avoidance responses –Avoidance-conditioning formulation –Phobias develop from two related sets of learning: 1. Via classical conditioning 2. Person learns to reduce conditioned fear by escaping from or avoiding the CS (operant conditioning)
.")
12
Behavioural Theories (cont.) Modelling—person can also learn fears through imitating the reactions of others. –Learning of fear by observing others is referred to as vicarious learning. Prepared Learning—people tend to fear only certain objects and events –Fear spiders, snakes, and heights but not lambs –Some fears may reflect classical conditioning, but only to stimuli to which an organism is physiologically prepared to be sensitive Is a diathesis needed ? –Cognitive diathesis such as the tendency to believe that similar traumatic experiences will occur in the future or not being able to control the environment may be important in developing a phobia. Social Skills Deficits in Social Phobias –Inappropriate behaviour or a lack of social skills the cause of social anxiety

13
Etiology of Phobia (cont.) Cognitive Theories –Focus on how people’s thought processes can serve as a diathesis and on how thoughts can maintain a phobia –Anxiety is related to being more likely to: 1.Attend to negative stimuli 2.Interpret ambiguous information as threatening 3.Believe that negative events are more likely than positive ones to re-occur Cognitive-behavioural models of social phobia –link social phobia to certain cognitive characteristics: 1.Attentional bias to focus on negative social information 2.Perfectionistic standards for accepted social performances 3.High degree of public self-consciousness
 Cognitive Theories –Focus on how people’s thought processes can serve as a diathesis and on how thoughts can maintain a phobia –Anxiety is related to being more likely to: 1.Attend to negative stimuli 2.Interpret ambiguous information as threatening 3.Believe that negative events are more likely than positive ones to re-occur Cognitive-behavioural models of social phobia –link social phobia to certain cognitive characteristics: 1.Attentional bias to focus on negative social information 2.Perfectionistic standards for accepted social performances 3.High degree of public self-consciousness")
14
Etiology of Phobia (cont.) Predisposing Biological Factors 1. Autonomic Nervous System –Autonomic lability 2. Genetic factors –Blood-and-injection phobia has a strong familial association 64% have at least one first-degree relative with the same disorder 3-4% prevalence in general population –Prevalence of social and specific phobias higher than average in first-degree relatives of patients –Twin studies also provide support

15
Etiology of Phobias (cont.) Psychoanalytic Theory –Phobias are a defence against the anxiety produced by repressed id impulses
 Psychoanalytic Theory –Phobias are a defence against the anxiety produced by repressed id impulses")
16
Therapies for Phobias Behavioural Approaches Systematic desensitization – In vivo exposure – Virtual reality exposure Flooding Cognitive approaches – Viewed with skepticism because of a central defining characteristic of phobias Phobic fear is recognized by the individual as excessive or unreasonable. Cognitive-Behavioural Case Formulation Framework –Contains causal and maintaining factors –Permits the development of case formulation and treatment planning

17
Therapies for Phobias (cont.) Biological Approaches Anxiolytics—Drugs that reduce anxiety (sedatives and tranquilizers) –Barbiturates—first major category of drugs used to treat anxiety disorders and we supplanted in the 1950s by two other classes of drugs: Propanediols (e.g., Miltown) Benzodiazepines (e.g., Valium and Xanax). –Today newer benzodiazepines such as Ativan and Clonapam are prescribed Monoamine oxidase (MAO) inhibitors and SSRIs also used to treat SP
 inhibitors and SSRIs also used to treat SP.")
18
Therapies for Phobias (cont.) Psychoanalytic Approach Attempt to uncover the repressed conflicts believed to underlie the extreme fear and avoidance characteristic of disorder
 Psychoanalytic Approach Attempt to uncover the repressed conflicts believed to underlie the extreme fear and avoidance characteristic of disorder")
19
Panic Disorder Panic Attack—person suffers a sudden and often inexplicable attack of alarming symptoms: –Laboured breathing, heart palpitations, –Nausea and chest pain; –Feelings of Choking and smothering; Dizziness, sweating, and trembling; –Intense apprehension, terror, and feelings of impending doom. May also experience depersonalization and derealization

20
Panic Disorder (cont.) Other features: –Panic attacks may occur frequently –May be linked specific situations if so referred to as cued panic attacks –Panic disorder is diagnosed as with or without agoraphobia Lifetime prevalence –2-3% for men –5-6% for women –Typically begins in adolescence –Onset associated with stressful life experience –> 80% of patients diagnosed as having an anxiety disorder also experience panic attacks
 Other features: –Panic attacks may occur frequently –May be linked specific situations if so referred to as cued panic attacks –Panic disorder is diagnosed as with or without agoraphobia Lifetime prevalence –2-3% for men –5-6% for women –Typically begins in adolescence –Onset associated with stressful life experience –> 80% of patients diagnosed as having an anxiety disorder also experience panic attacks")
21
Panic Disorder in Canadian University Students 34% of first-year and 22.1% of university students reported having experienced at least one panic attack during the previous year Those meeting criteria for panic attack had 4 attacks on average over the previous year

22
Etiology of Panic Disorder Biological Theories Mitral valve prolapse syndrome Inner ear disease causes dizziness May be linked to “Val158Met COMT polymorphism” or other loci within or near the COMT gene (on chromosome 22)
")
23
Etiology of Panic Disorder (cont.) Noradrenergic activity theory –Panic is caused by overactivity in the noradrenergic system Specifically locus ceruleus has been implicated Stimulation of the locus ceruleus causes monkeys to have “panic attack” in humans yohimbine (drug that stimulates activity in the locus ceruleus) can elicit panic attacks Problem in gamma-aminobutyric acid (GABA) –GABA generally inhibit noradrenergic activity –Positron emission tomography study found fewer GABA-receptor binding sites in people with PD Cholecystokinin (CCK) –Peptide that occurs in the cerebral cortex, amygdala, hippocampus, and brain stem, induces anxiety-like symptoms in rats and effect can be blocked with benzodiazepines
 Noradrenergic activity theory –Panic is caused by overactivity in the noradrenergic system Specifically locus ceruleus has been implicated Stimulation of the locus ceruleus causes monkeys to have panic attack in humans yohimbine (drug that stimulates activity in the locus ceruleus) can elicit panic attacks Problem in gamma-aminobutyric acid (GABA) –GABA generally inhibit noradrenergic activity –Positron emission tomography study found fewer GABA-receptor binding sites in people with PD Cholecystokinin (CCK) –Peptide that occurs in the cerebral cortex, amygdala, hippocampus, and brain stem, induces anxiety-like symptoms in rats and effect can be blocked with benzodiazepines")
24
Etiology of Panic Disorder (cont.) Psychological Theories –The fear-of-fear hypothesis Suggests that agoraphobia is not a fear of public places per se, but a fear of having a panic attack in public. –Misinterpretation of physiological arousal symptoms

25
Therapies for Panic Disorder Biological Treatments –Antidepressants Both selective SSRIs and tricyclic antidepressants have been used successfully to treat PD Psychological Treatments –Exposure-based treatments are often useful in reducing PD with agoraphobia –Cognitive-Behavioural Therapy

26
Generalized Anxiety Disorder People with GAD are persistently anxious and often about minor items. –Chronic, uncontrollable worry about everything Most frequent worries concern their health and the hassles of daily life

27
GAD (cont.) Other features include: –Difficulty concentrating, –Tiring easily, restlessness, –Irritability, –A high level of muscle tension Lifetime prevalence is 5% for the general population GAD typically begins in mid-teens Stressful life events play role in onset
 Other features include: –Difficulty concentrating, –Tiring easily, restlessness, –Irritability, –A high level of muscle tension Lifetime prevalence is 5% for the general population GAD typically begins in mid-teens Stressful life events play role in onset")
28
Etiology of GAD Cognitive-Behavioural Perspectives –See learning views of phobias Anxiety regarded as having been classically conditioned to external stimuli, but with a broader range of conditioned stimuli.

29
Etiology of GAD (cont.) Biological Perspectives –GAD may have a genetic component. –Neurobiological model for GAD based on fact that benzodiazepines are often effective in treating anxiety Receptor in the brain for benzodiazepines has been linked to the inhibitory neurotransmitter GABA Benzodiazepines may anxiety by release of GABA –Drugs that block or inhibit the GABA system anxiety

30
Etiology of GAD (cont.) Psychoanalytic Perspective –Unconscious conflict between the ego and id impulses
 Psychoanalytic Perspective –Unconscious conflict between the ego and id impulses")
31
Therapies for GAD Treatment for GAD is very similar to that for phobias

32
Obsessive-Compulsive Disorder Obsessive-compulsive disorder (OCD)— an anxiety disorder in which the mind is flooded with persistent and uncontrollable thoughts (obsessions) and the individual is compelled to repeat certain acts again and again (compulsions)
— an anxiety disorder in which the mind is flooded with persistent and uncontrollable thoughts (obsessions) and the individual is compelled to repeat certain acts again and again (compulsions)")
33
Obsessions vs. Compulsions Obsession— intrusive and recurring thoughts, impulses, and images –Most frequent obsessions: fears of contamination, fears of expressing some sexual or aggressive impulse, and hypochondriacal fears of bodily dysfunction Compulsion— a repetitive behaviour or mental act that the person feels driven to perform to reduce the distress caused by obsessive thoughts or to prevent some calamity from occurring –Examples: checking, cleanliness and orderliness, avoiding particular objects, performing protective practices or a particular act

34
OCD (cont.) Other features of OCD –Lifetime prevalence of 1 to 2% –Affects women > than men –Early onset (before age 10) is more common among men and is associated with checking compulsions –Later onset is more frequent among women and is linked with cleaning compulsions –Depression is often comorbid with OCD
 Other features of OCD –Lifetime prevalence of 1 to 2% –Affects women > than men –Early onset (before age 10) is more common among men and is associated with checking compulsions –Later onset is more frequent among women and is linked with cleaning compulsions –Depression is often comorbid with OCD")
35
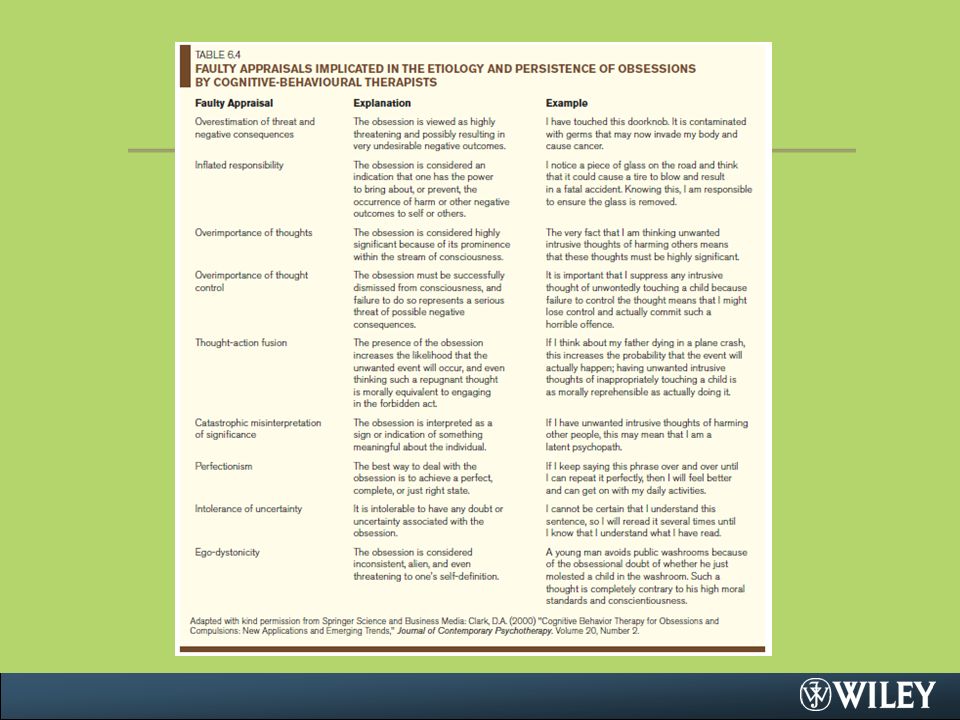
Etiology of OCD Behavioural and Cognitive Theories Learned behaviours reinforced by fear reduction Rachman’s theory of obsessions in OCD –Unwanted intrusive thoughts are the roots of obsessions –Obsessions often involve catastrophic misinterpretations of negative intrusive thoughts See Table 6.4 for list of faulty cognitive appraisals

37
Etiology of OCD (cont.) Biological Factors Genetic evidence High rates of anxiety disorders occur among the first- degree relatives (10.3%) than control relatives (1.9%) Brain structure –Encephalitis, head injuries, and brain tumours associated with the development of OCD –PET scan studies shown activation in the frontal lobes –Basal ganglia dysfunction further linked to OCD due to link with Tourette’s syndrome, which is marked by motor and vocal tics
 Biological Factors Genetic evidence High rates of anxiety disorders occur among the first- degree relatives (10.3%) than control relatives (1.9%) Brain structure –Encephalitis, head injuries, and brain tumours associated with the development of OCD –PET scan studies shown activation in the frontal lobes –Basal ganglia dysfunction further linked to OCD due to link with Tourette’s syndrome, which is marked by motor and vocal tics")
38
Etiology of OCD (cont.) Biological Factors con’t. Hypothesized to be related to serotonin –40-60% of OCD clients treated with SSRIs do not show improvement

39
Etiology of OCD (cont.) Psychoanalytic Theory Classical psychoanalysis: –Obsessions and compulsions are viewed as similar –Result from instinctual forces, sexual or aggressive, that are not under control because of overly harsh toilet training Alfred Adler viewed OCD as a result of feelings of incompetence due to an inferiority complex
 Psychoanalytic Theory Classical psychoanalysis: –Obsessions and compulsions are viewed as similar –Result from instinctual forces, sexual or aggressive, that are not under control because of overly harsh toilet training Alfred Adler viewed OCD as a result of feelings of incompetence due to an inferiority complex")
40
Therapies for OCD Exposure and Response Prevention (ERP) –Most widely used and accepted behavioural approach –Combines exposure with response prevention Cognitive-Behaviour Therapy Biological Treatment –Drugs increasing serotonin, e.g., SSRIs and tricyclics –ERP and fluoxetine treatments show same changes in brain function –Cingulotomy Psychoanalytic Therapy –Resembles that for phobias and generalized anxiety
 –Most widely used and accepted behavioural approach –Combines exposure with response prevention Cognitive-Behaviour Therapy Biological Treatment –Drugs increasing serotonin, e.g., SSRIs and tricyclics –ERP and fluoxetine treatments show same changes in brain function –Cingulotomy Psychoanalytic Therapy –Resembles that for phobias and generalized anxiety")
41
Post-Traumatic Stress Disorder Extreme response to a severe stressor, including increased anxiety, avoidance of stimuli associated with the trauma, and a numbing of emotional responses. –Note. Unlike the definitions of other psychological disorders, the definition of PTSD includes part of its presumed etiology –The stressor can be experienced directly, vicariously, or via indirect, information exposure

42
PTSD (cont.) The symptoms for PTSD are grouped into three major clusters. 1.Re-experiencing the traumatic event 2.Avoidance of stimuli associated with the event or numbing of responsiveness 3.Symptoms of increased arousal Prevalence rate = 1 to 3% PTSD vs. Acute Stress Disorder –If stressor causes significant impairment in social or occupational functioning < than one month then acute stress disorder is diagnosed

43
Risk Factors of PTSD Risk Factors Exposure to trauma and severity of trauma Gender (more females) Perceived threat to life Personality traits of neuroticism and extroversion Early conduct problems Family history of psychiatric disorders Presence of pre-existing psychiatric disorders Early separation from parents Previous exposure to traumas Tendency to take personal responsibility for failures and to cope with stress by focusing on emotions Attachment style Stressful occupations
 Perceived threat to life Personality traits of neuroticism and extroversion Early conduct problems Family history of psychiatric disorders Presence of pre-existing psychiatric disorders Early separation from parents Previous exposure to traumas Tendency to take personal responsibility for failures and to cope with stress by focusing on emotions Attachment style Stressful occupations")
44
Etiology of PTSD Psychological Theories –PTSD arises from a classical conditioning of fear –Anxiety sensitivity Biological theories –Genetics –Specific domains of noradrenergic system Trauma may raise levels of norepinephrine Evidence for increased sensitivity of noradrenergic receptors in patients with PTSD –Associated with smaller hippocampal volume –Associated with anterior cingulate and medial prefrontal function

45
Therapies for PTSD Crisis intervention Exposure-based behaviour therapy –Exposure to thoughts and images of the frightening event Systematic desensitization Eye Movement Desensitization and Reprocessing Relaxation + rational-emotive therapy + training in problem solving Psychoactive drugs –See Table 6.5

47
Canadian Clinic Focus 6.1 Anxiety Treatment and Research Centre, St. Joseph Hospital, Hamilton, Ontario Referral process Assessment Treatment Research Training programs –Comments: such centres are not available to the majority of Canadians

48
Copyright Copyright © 2011 John Wiley & Sons Canada, Ltd. All rights reserved. Reproduction or translation of this work beyond that permitted by Access Copyright (The Canadian Copyright Licensing Agency) is unlawful. Requests for further information should be addressed to the Permissions Department, John Wiley & Sons Canada, Ltd. The purchaser may make back-up copies for his or her own use only and not for distribution or resale. The author and the publisher assume no responsibility for errors, omissions, or damages caused by the use of these programs or from the use of the information contained herein.
 is unlawful. Requests for further information should be addressed to the Permissions Department, John Wiley & Sons Canada, Ltd. The purchaser may make back-up copies for his or her own use only and not for distribution or resale. The author and the publisher assume no responsibility for errors, omissions, or damages caused by the use of these programs or from the use of the information contained herein..")
Similar presentations





 Anxiety Disorders.>")

 David Myers PowerPoint Slides Worth Publishers, © 2007.>")












