Download presentation
Presentation is loading. Please wait.

1
Anatomical modification of Dens Invaginatus treatment
Dr. Fouad Abduljabbar, BDS,MDS Consultant Endodontist, King Abdulziz Medical City Ministry of National Guard, Saudi Arabia

3
Outlines: Anatomical modification of dens invagenatus treatment
Defintion Features Etiology Histology Prevalence Classification Diagnosis Treatment Case Report Abduljabbar F, Aljehani M, Al Sharafi E, Bakhsh A, Abed H, Alghamdi A. Anatomical Modification for Dens Invaginatus Treatment: A Literature Review and a Case Report. Journal of International Oral Health 2015; 7(12):
:")
4
Dens invaginatus (DI) is a developmental anomaly which rarely occurs
Dens invaginatus (DI) is a developmental anomaly which rarely occurs. It is the result of invagination of enamel organ into the dental papilla during the soft tissue stage of tooth development.
 is a developmental anomaly which rarely occurs. It is the result of invagination of enamel organ into the dental papilla during the soft tissue stage of tooth development.")
5
Features As the hard tissues are formed, the invaginated enamel produces a small tooth within the pulp chamber It begins at the crown and sometimes extends into the root

6
Features The malformation shows a morphologic variation and results in pulp necrosis Crown morphology: (peg-shaped, barrel-shaped, incisal notching or increased labiolingual and mesiodistal diameter) Root canal treatment may present a severe problem because of the complex anatomy of teeth
 Root canal treatment may present a severe problem because of the complex anatomy of teeth.")
7
Etiology No exact cause
Several theories have been suggested to clarify the etiology of this anomaly: - Localized failure of growth (unknown, infection, trauma) - Genetic factors
 - Genetic factors.")
8
Histology The dentin below invagination could be intact without irregularities It may also contain strains of vital tissue or even fine canals that communicate to the dental pulp. Enamel lining the invagination was shown to be irregularly structured Studies reported differences in structure between the external and internal enamel .** Piatelli A, Trisi P. Dens invaginatus: A histological study of undemineralized material. Endod Dent Traumatol 1993;9:191-5

9
Prevalence The range of occurrence is between 0.04% and 26%
The most commonly affected teeth are maxillary lateral incisors Data suggest a more male gender predilection Contralateral tooth ** Omnell KA, Swanbeck G, Lindahl B. Dens invaginatus. II. A microradiographical, histological and micro X-ray diff raction study. Acta Odontol Scand 1960;18:303-30 ** Rotstein I, Stabholz A, Heling I, Friedman S. Clinical considerations in the treatment of dens invaginatus. Endod Dent Traumatol 1987;3(5): ** Hülsmann M. Dens invaginatus: Aetiology, classifi cation, prevalence, diagnosis, and treatment considerations. Int Endod J 1997;30(2):79-90. ** Alani A, Bishop K. Dens invaginatus. Part 1: Classifi cation, prevalence and aetiology. Int Endod J 2008;41(12):
: ** Hülsmann M. Dens invaginatus: Aetiology, classifi cation, prevalence, diagnosis, and treatment considerations. Int Endod J 1997;30(2): ** Alani A, Bishop K. Dens invaginatus. Part 1: Classifi cation, prevalence and aetiology. Int Endod J 2008;41(12):")
10
Classification Oehlers Classification:
Type I: A minor enamel lined invagination, which is confined to the crown of the tooth but not extending beyond the cementoenamel junction Type II: Enamel-lined invagination extending beyond the cementoenamel junction; may or may not communicate with the pulp Type III: The invagination extends through the root. Usually, there is no communication with the pulp ** Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957;10(11):
. I. Variations of. the invagination process and associated anterior crown forms. Oral Surg Oral. Med Oral Pathol 1957;10(11):")
11
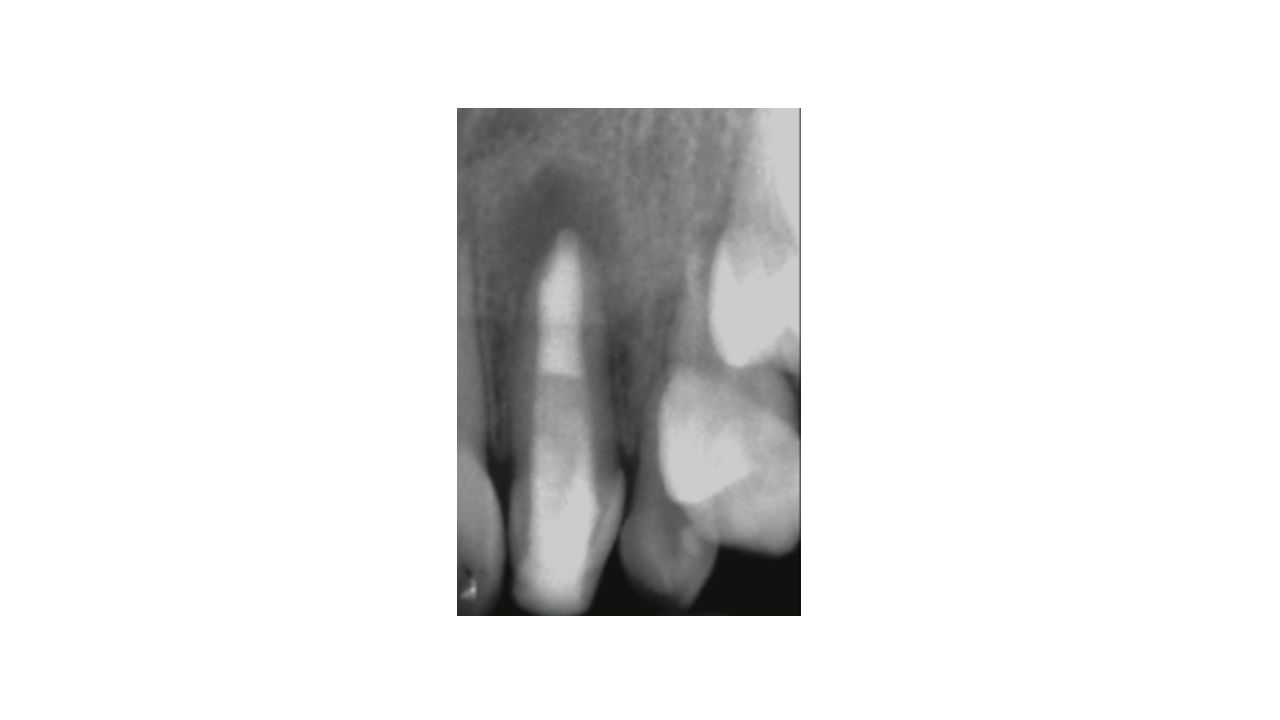
Diagnosis Dental Radiograph - Narrow fissure - Tear-drop shape
- Radiolucent periapical lesion

12
Diagnosis Clinical morphological; incisal notching, labial groove, exaggerated palatal cingulum Magnification

13
Treatment Extraction Root canal treatment (RCT)
Different preventive procedures Open- apex tooth management

15
Case Report - 10-year-old medically free girl - Clinical examination
- Intraoral sinus tract buccal to the tooth - Non-mobile but tender to percussion - Periapical radiograph: periapical radiolucency

19
6 months 2 years

20
Preoperative Postoperative 6 months 2 years

21
Conclusion Modificaton of the internal anatomy of the canal system may be considered by clinicians for the treatment of DI treatment, to gain better access for instrumentation, disinfection, and sealing of the root canal.

22
Thank you

Similar presentations























 3- Pulp space Morphology: a. Root canal.>")