Download presentation
Presentation is loading. Please wait.

1
Inflammatory Bowel Disease Dr.S.Nandakumar Professor of Medicine 2nd Year Gastrointestinal System

2
Learning Objectives Name the 2 major types of idiopathic inflammatory bowel disease (IBD) Describe the epidemiology and aetiology of Crohn’s disease and ulcerative colitis (UC) Describe and contrast the pathological changes in the bowel in Crohn’s and UC Describe the clinical features of Crohn’s disease and UC Outline the clinical approach to a patient with suspected IBD Describe the management of Crohn’s disease and UC List the complications of Crohn’s disease and UC
 Describe the epidemiology and aetiology of Crohn’s disease and ulcerative colitis (UC) Describe and contrast the pathological changes in the bowel in Crohn’s and UC Describe the clinical features of Crohn’s disease and UC Outline the clinical approach to a patient with suspected IBD Describe the management of Crohn’s disease and UC List the complications of Crohn’s disease and UC")
3
Inflammatory Bowel Diseases 1.Specific infections –Viruses –Bacteria –Protozoa and worms 2.Other specific conditions –Coeliac disease and other food allergies –Drug-induced –Radiation enteritis –Ischaemia –Vasculitis (Behcet’s) –Diverticulitis
 –Diverticulitis")
4
Inflammatory Bowel Diseases 3. Idiopathic IBD –Crohn’s disease –Ulcerative Colitis Exclude 1 and 2, then consider 3

5
Idiopathic IBD

6
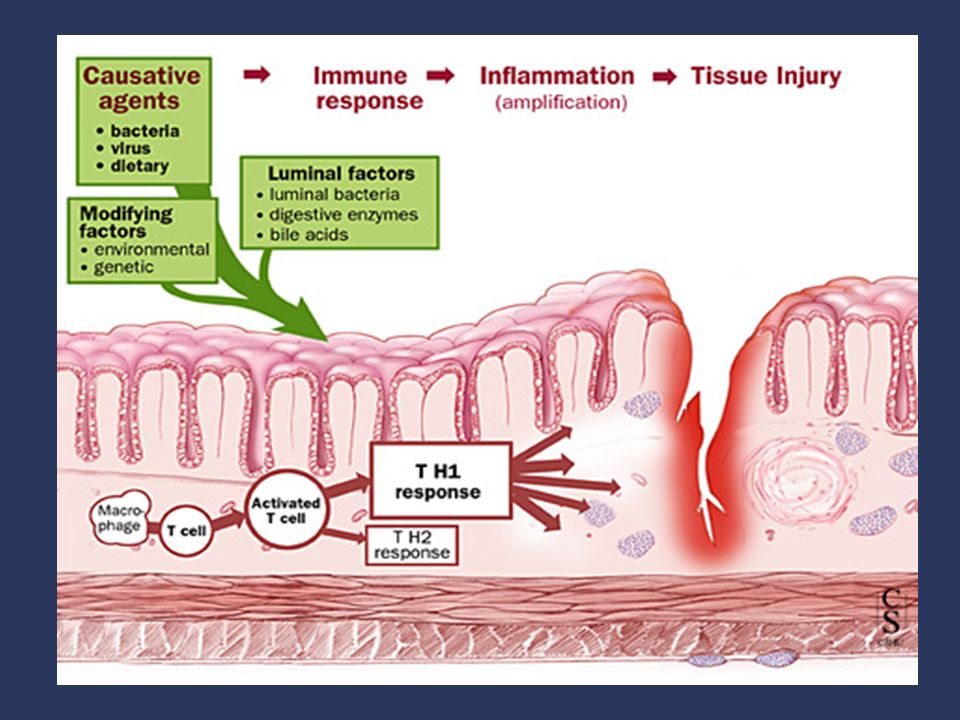
ETIOLOGIC HYPOTHESES

7
Gene-Environment Interaction

9
Impact of Race and Ethnicity Basu, D; Am J Gastroenterology 100:2254-2261, 2005 A Whites had stronger family history of IBD and colorectal cancer. African Americans with CD had higher incidence of arthritis. Disease severity similar across all groups. P-anca served as a sensitive maker for Mexican Americans as 100% with UC were positive compared with 40% in whites

10
Crohn’s diseaseUC Prevalence (Malaysia) 3.6 per 100,0006 per 100,000 Age of onset15-44 SexM=FF>M GeographyCommon in Europeans + Jewish people Identical twin concordance 42.2%16.5%
 3.6 per 100,0006 per 100,000 Age of onset15-44 SexM=FF>M GeographyCommon in Europeans + Jewish people Identical twin concordance 42.2%16.5%")
12
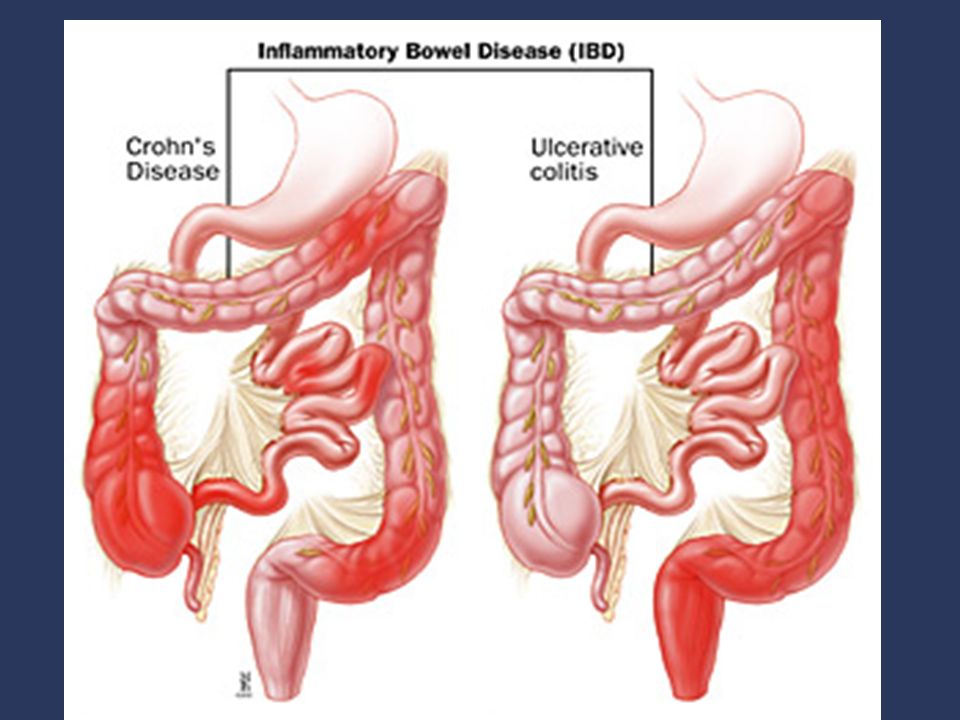
Crohn’s diseaseUC Infective agent ?virus ?measles ?M.paraTB Precipitated by gastroenteritis/ antibiotics OCPillMore incidenceNo effect SmokersMore incidenceLess incidence Part of bowel affected Mouth to anusColon LesionsDiscontinuous (skip) Rectum upwards (to ileocaecal valve) Extent of wall involvement Full-thicknessMucosa only
 Rectum upwards (to ileocaecal valve) Extent of wall involvement Full-thicknessMucosa only")
14
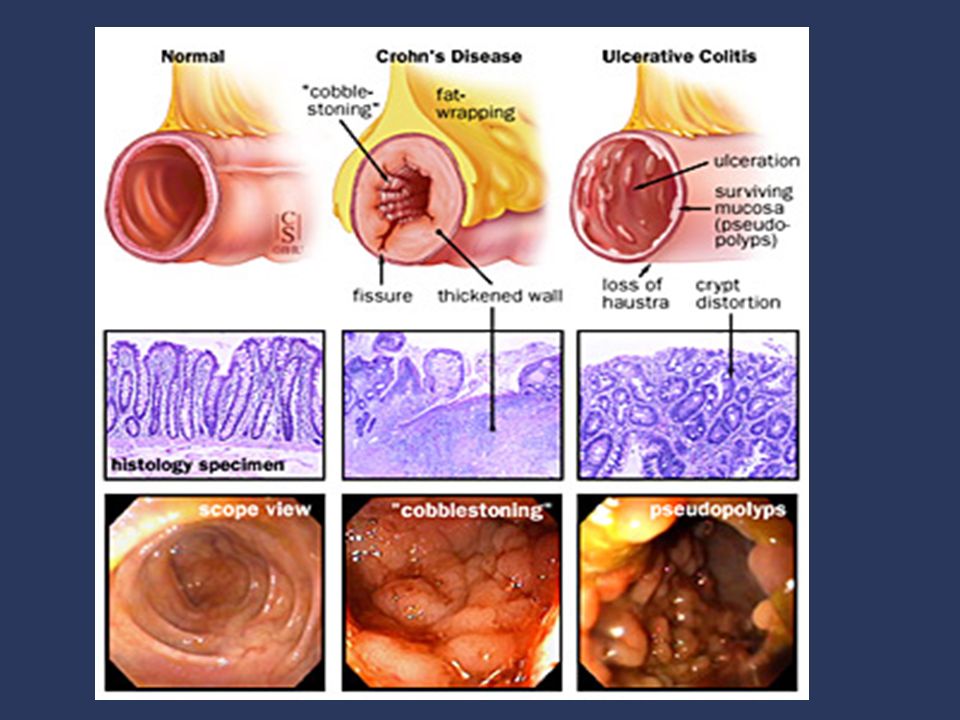
Crohn’s diseaseUC InflammationDeep(transmural) & patchy Superficial & continuous Granulomas++Rare Goblet cellsPresentDepleted Crypt abscesses ++++
 & patchy Superficial & continuous Granulomas++Rare Goblet cellsPresentDepleted Crypt abscesses ++++")
15
Clinical features- Crohn’s Diarrhoea –Present in 80% –Contains blood if colon affected Abdominal pain –May be colicky –May mimic appendicitis Weight loss Constitutional symptoms Recurrent disease (normal life in between)
")
16
Clinical features- Crohn’s Thin, generally unwell Aphthous ulcers in mouth May have abdominal tenderness May have Rt.iliac fossa mass Anal tags/fissures or perianal abscess

17
Management of Crohn’s disease Medical –Steroids –Azathioprine –Sulphasalazine (5-ASA) Surgical –80% of pts need surgery at some point –Recurrence almost inevitable, so surgery avoided as much as possible but there are certain indications such as failure of medical therapy, complications
 Surgical –80% of pts need surgery at some point –Recurrence almost inevitable, so surgery avoided as much as possible but there are certain indications such as failure of medical therapy, complications")
19
Referral Population Cohort: Disease Distribution at Presentation n = 1116 37% 17% 46% Farmer RG, Easley KA, Ranking GB. Dig Dis Sci 1993;38(6):1137-1146
:")
20
UC Pathology Macroscopic Appearance –Limited to mucosa and submucosa of rectum and colon –Presence of numerous ulcers with heaped up regenerating mucosa-> “pseudopolyps” & – superficial fissures –Microscopic Appearance –Polymorphs infiltrate crypts of Lieberkuhn at mucosal base to form crypt abscesses. –superficial desquamation of epithelium leads to ulcer formation-> cryptitis –Adjacent mucosa which becomes edematous-> causing hyperemia and wall thinning

21
Clinical features- UC Majority (80%) - mild, predominantly distal disease Diarrhoea with blood and mucus –Can be up to 20x per day Lower abdominal discomfort Malaise, anorexia Rectal disease: urgency, tenesmus Slight abdominal tenderness + distension PR- blood
 - mild, predominantly distal disease Diarrhoea with blood and mucus –Can be up to 20x per day Lower abdominal discomfort Malaise, anorexia Rectal disease: urgency, tenesmus Slight abdominal tenderness + distension PR- blood")
22
UC Clinical Features Minority (20%) - pancolitis –Anemia, fatigue, anorexia, weight loss –Chronic colitis-> loss of mucosal folds, – haustra: lead pipe appearance on radiograph –Toxic megacolon: fever, abd pain, tachycardia, focal tenderness, leukocytosis, –Radiographic dilatation >6cm t-colon; risk of gangrene, perforation
 - pancolitis –Anemia, fatigue, anorexia, weight loss –Chronic colitis-> loss of mucosal folds, – haustra: lead pipe appearance on radiograph –Toxic megacolon: fever, abd pain, tachycardia, focal tenderness, leukocytosis, –Radiographic dilatation >6cm t-colon; risk of gangrene, perforation")
23
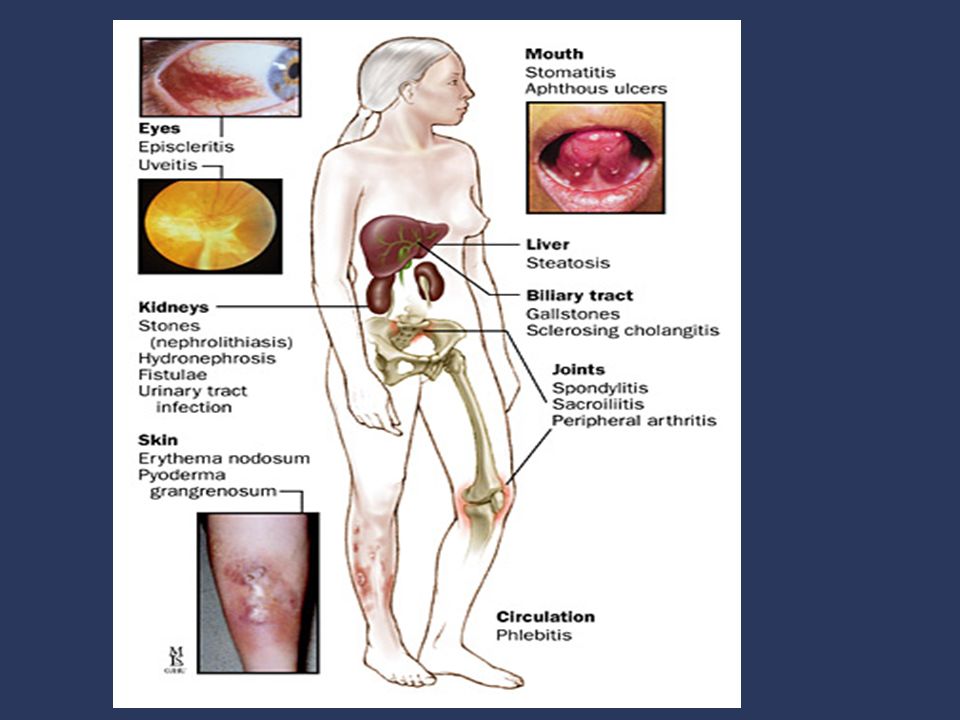
Extra intestinal manifestations Arthritis (20%) knees, ankles, hips, shoulders typically in association with increased activity of intestinal disease Ankylosing spondylitis (3-5%) HLA-B27+ or FamHx of AS Erythema nodosum (10-15%) Often in conjunction with arthropathy Pyoderma gangrenosum (rare) PG is associated with IBD in 50% of cases
 knees, ankles, hips, shoulders typically in association with increased activity of intestinal disease Ankylosing spondylitis (3-5%) HLA-B27+ or FamHx of AS Erythema nodosum (10-15%) Often in conjunction with arthropathy Pyoderma gangrenosum (rare) PG is associated with IBD in 50% of cases")
24
UC Diagnosis Rule out infectious causes –Fecal leukocytes Confirm inflammatory origin to diarrhea, urgency etc –Stool cultures, Ova & Parasites Campylobacter, Salmonella, Shigella, C. Proctosigmoidoscopy Indeterminate Colitis –Treat as UC until/if declares itself Crohn’s

25
Risk for carcinoma in UC A. Disease duration –25% at 25 yrs, 35% at 30 yrs, 45% at 35 yrs, and 65% at 40 yrs B. Severity of Inflammation C. Colonic stricture must be considered to be cancer until proven otherwise

26
UC Medical Therapy Aminosalicylates (e.g. sulfasalazine, mesalamine) –Block cyclooxygenase, lipoxygenase pathways Corticosteroids (e.g. prednisone, budesonide) –Block phospholipase A2, thereby decreasing prostaglandins and leukotrienes –effective in rectal and left-sided disease with fewer adverse systemic effects Immunomodulatory agents –6-MP, Azathioprine - inhibit proliferation of T>B lymphoctyes –Cyclosporine - inhibits IL-2 gene transcription
 –Block cyclooxygenase, lipoxygenase pathways Corticosteroids (e.g. prednisone, budesonide) –Block phospholipase A2, thereby decreasing prostaglandins and leukotrienes –effective in rectal and left-sided disease with fewer adverse systemic effects Immunomodulatory agents –6-MP, Azathioprine - inhibit proliferation of T>B lymphoctyes –Cyclosporine - inhibits IL-2 gene transcription.")
27
Indications for Surgery Intractability (most common indication) –Debilitating symptoms, complications of steroid therapy, extra colonic manifestations Dysplasia-Carcinoma Massive colonic bleeding Toxic mega colon
 –Debilitating symptoms, complications of steroid therapy, extra colonic manifestations Dysplasia-Carcinoma Massive colonic bleeding Toxic mega colon")
28
Extra GI manifestations Both Crohn’s and UC patients sometimes have extra gastrointestinal manifestations of disease

30
Clinical approach (History) PH: Fever, anorexia, weight loss, diet Eye, mouth, skin, joint symptoms PMH: Previous diarrhoea, TB, abdo surgery DH:NSAIDS, antibiotics, OCP, allergies FH:IBD, other abdo problems, TB SH:Race, travel, contacts, food hygiene, food intolerance, smoking, alcohol
 PH: Fever, anorexia, weight loss, diet Eye, mouth, skin, joint symptoms PMH: Previous diarrhoea, TB, abdo surgery DH:NSAIDS, antibiotics, OCP, allergies FH:IBD, other abdo problems, TB SH:Race, travel, contacts, food hygiene, food intolerance, smoking, alcohol")
31
Investigations Haem: Hb, WCC, Plts, ESR Biochem: K, Na, Urea, Cr, Albumin, LFT Micro. stool: WCC, ova, cysts, culture, C. difficile toxin Micro blood: Culture, Yersinia Ab Immunology: Endomysial Ab (for Coeliac)
.")
32
Investigations Radiology –CXR for TB –Abdo XR for toxic dilatation/obstruction –Small bowel barium swallow –Barium enema –Isotope labelled white cell scan Endoscopy and biopsy: –OGDS (+ small bowel) –Sigmoidoscopy/colonoscopy
 –Sigmoidoscopy/colonoscopy")
33
Moderately severe ulcerative colitis with irregular, inflamed, ulcerated mucosa & patchy exudate

34
Management of ulcerative colitis Medical –Steroids –Sulphasalazine –Steroid/ 5-ASA enema Surgical –20-30% require surgery –Colectomy is curative –Main indication is severe attack unresponsive to medical therapy

35
Therapeutic Pyramid for Active UC Severe Moderate Mild Systemic Corticosteroids Aminosalicylates Surgery Oral Steroids AZA/6-MP Cyclosporine Cyclosporine Infliximab

36
Complications Fistulas, fissures, abscess (esp Crohn’s) Toxic dilatation (megacolon) Perforation Massive haemorrhage (rare) Carcinoma of colon
 Toxic dilatation (megacolon) Perforation Massive haemorrhage (rare) Carcinoma of colon")
37
Toxic megacolon

38
Conclusion Crohn’s disease and ulcerative colitis are the 2 major idiopathic inflammatory bowel diseases Aetiology remains unclear Patient usually present with diarrhoea +/- blood and mucus, abdo pain and weight loss Patients sometimes have extra GI manifestations Treatment is initially medical, with surgery for patients who don’t improve or develop complications

39
Thank you

Similar presentations










, FRCS (Glasg), FAMS, DNB, FACS, FICS Professor of Surgery.>")
 Kristina Blaslov Mentor: A. Žmegač Horvat.>")








 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")