Download presentation
Presentation is loading. Please wait.

1
BLOOD TRANSFUSION

2
Objectives: This lecture provides an understanding of: Blood groups Routine pre-transfusion compatibility testing Transfusion reactions Overview of bone marrow transplantation

3
Learning outcome Review blood groups Recall the routine pre-transfusion compatibility testing Discuss transfusion reactions Overview of bone marrow transplantation

4
Blood groups: red cell groups Antigens (blood group antigens) A series of glycoproteins and glycolipids on the surface of red blood cells The development of these antigens is genetically controlled
 A series of glycoproteins and glycolipids on the surface of red blood cells The development of these antigens is genetically controlled")
5
Blood groups: red cell groups 15 well-defined red cell blood group systems ABO, MNSs, P, Rh,Lutheran, Kell, Lewis, Duffy, Kidd, Diego, Yt, Xg, Ii, Dombrock, and Colton systems only two are of major importance in clinical practice ABO and Rh systems

6
Inheritance of all these blood group systems is determined 'by autosomal genes with the exception of the Xg system which is determined by genes on the X chromosome Blood groups: red cell groups

7
Antibodies Naturally occurring antibodies occur without any obvious antigenic stimulus in the serum of individuals lacking the corresponding red cell antigen

8
Blood groups: red cell groups Immune or acquired antibodies are produced in individuals as a result of stimulation by a red cell antigen which is not present on their own red cells or in their body fluids

9
Blood groups: red cell groups Complement-binding antibodies All the main blood group antibodies bind complement, with the exception of Rh and MN antibodies

10
Blood groups: red cell groups Naturally occurring red cell antibodies are partly or wholely IgM and generally react with their corresponding antigens at temperatures below 37°C

11
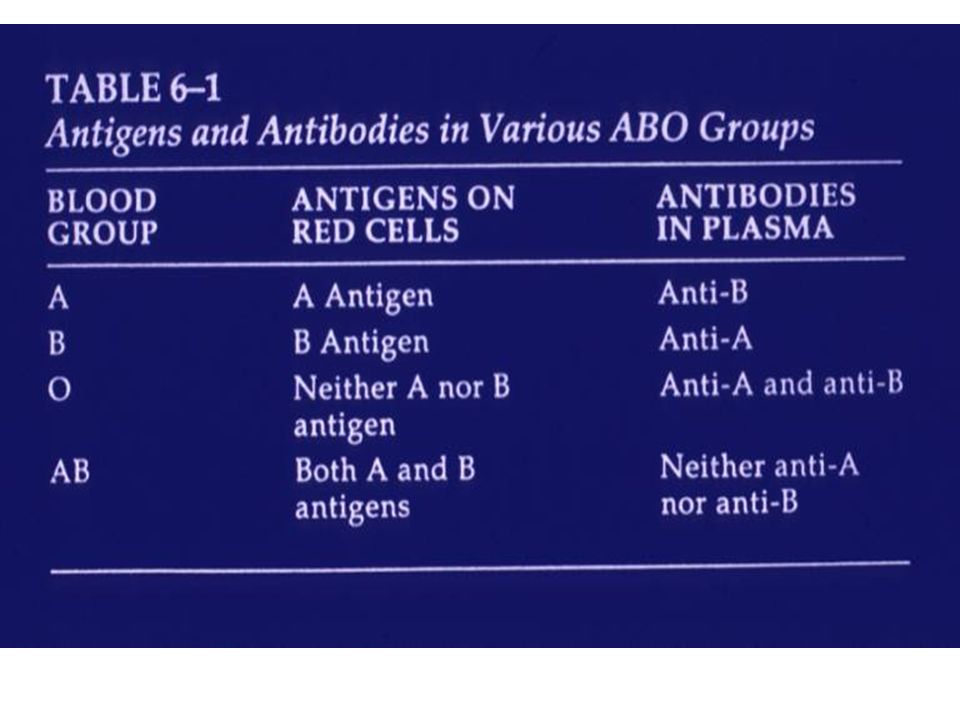
A B 0 Blood groups There are four different ABO groups, determined by whether or not an individual’s red cells carry the A antigen, the B antigen, both A and B, or neither Normal healthy individuals, from early in childhood, make antibodies against A or B antigens that are not present on their own cells

13
People who are group A have anti-B antibody in their plasma People who are group B have anti-A antibody in their plasma People who are group O have anti-A and anti-B antibodies in their plasma People who are group AB have neither of these antibodies in their plasma

14
A B 0 Blood groups 4 main groups - A B, A, B & O BLOOD GROUP AB A, BNil AAAnti B BBAnti A ONil AntiA, AntiB Blood groupAntigenAntibody

15
A,B, O Anti-A, Anti-B

16
Rhesus( Rh ) Blood groups Demonstrated in human RBCs by use of an antiserum prepared by immunizing rabbits with red cells from Rhesus monkey Rh (+)ve Rh (-)ve
 Blood groups Demonstrated in human RBCs by use of an antiserum prepared by immunizing rabbits with red cells from Rhesus monkey Rh (+)ve Rh (-)ve")
17
Rhesus( Rh ) Blood groups Rh Ag - C, c, D, d, E, e Rh Ab - results from immunization transfusion of Rh (+)ve blood into Rh (-)ve person or from passage of Rh (+)ve red cells from fetus into circulation of Rh (-)ve mother during pregnancy
 Blood groups Rh Ag - C, c, D, d, E, e Rh Ab - results from immunization transfusion of Rh (+)ve blood into Rh (-)ve person or from passage of Rh (+)ve red cells from fetus into circulation of Rh (-)ve mother during pregnancy")
18
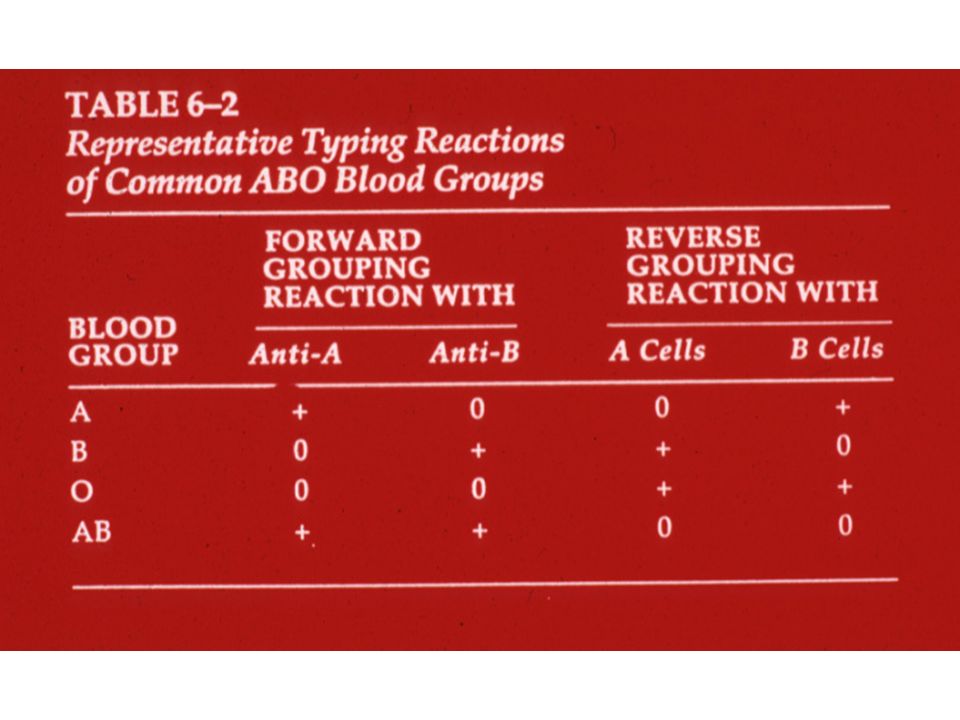
Blood Grouping Test ABO blood grouping in two ways 1. Cell grouping and 2. Serum grouping

21
Blood Grouping Test Cell grouping Antigenic character of the red cells is determined by reacting with the corresponding antibody This leads to hemeagglutination

22
Blood Grouping Test Serum grouping The character of the antibody present in the blood group established by cell grouping

23
CELL GROUPING A suspension of red cells is made to react with a known reagent antisera-anti–A and anti–B Positive agglutination indicates the presence of the corresponding antigen on the red cells

24
SERUM GROUPING Serum from the blood sample submitted for grouping is reacted with known A cells and B cells Agglutination indicates the presence of corresponding antibody in serum

27
Blood group Cell GroupingSerum Grouping Anti- A Anti- B Anti- AB A-cellB-cellO-cell A+-+-+- B-+++-- AB + ++--- O---++- ABO-CELL GROUPING AND SERUM GROUPING

28
Compatibility Testing A crossmatch consists of testing the patient’s plasma against a sample of red cells from the actual unit that has been selected for transfusion

29
Compatibility Testing Immediate spin: patient’s plasma is mixed with donor red cells and observed for immediate agglutination and/or haemolysis (A,B,O check) at room temperature ( 5 minutes)
 at room temperature ( 5 minutes)")
30
Compatibility Testing Full crossmatch:(or Coombs Crossmatch): patient’s plasma is mixed with donor red cells and incubated at 37 o C Anti IgG is added and a check is made for the presence of agglutination ( 40 minutes)
: patient’s plasma is mixed with donor red cells and incubated at 37 o C Anti IgG is added and a check is made for the presence of agglutination ( 40 minutes)")
38
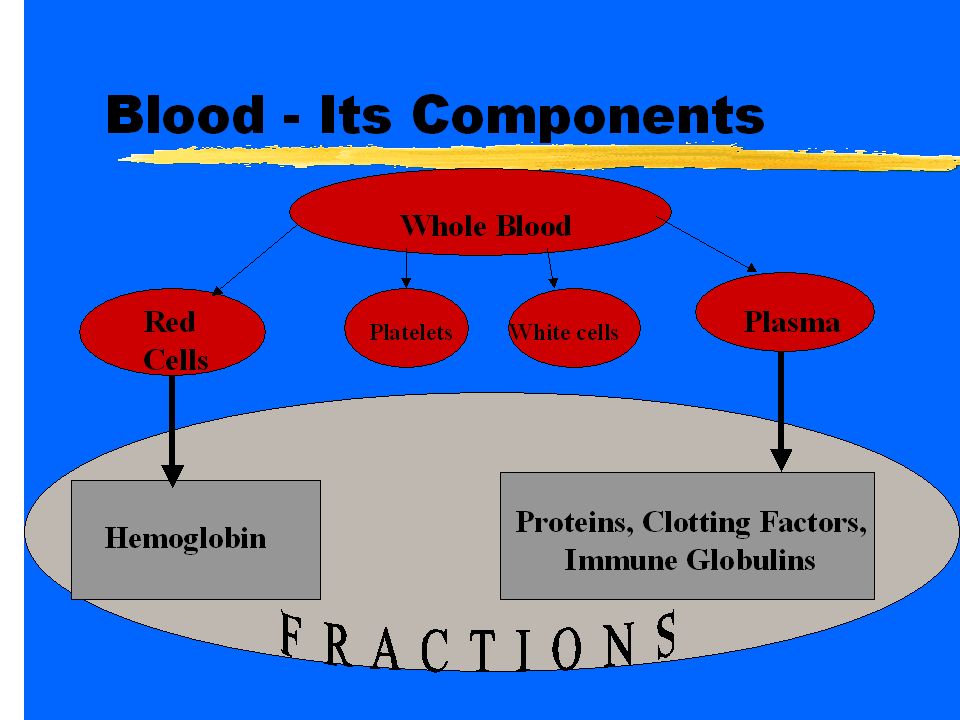
DEFINITIONS Blood product Any therapeutic substance prepared from human blood Whole blood Unseparated blood collected into an approved container containing an anticoagulant-preservative solution

39
DEFINITIONS Blood component 1. A constituent of blood, separated from whole blood, such as: Red cell concentrate Red cell suspension Plasma Platelet concentrates

40
Blood component 2. Plasma or platelets collected by apheresis 3. Cryoprecipitate, prepared from fresh frozen plasma: rich in Factor VIII and fibrinogen

41
DEFINITIONS Plasma derivative Human plasma proteins prepared under pharmaceutical manufacturing conditions, such as: Albumin Coagulation factor concentrates Immunoglobulins

42
Principles of clinical transfusion practice Transfusion is only one part of the patient’s management Transfusion should be prescribed only when the benefits to the patient are likely to outweigh the risks

43
Appropriate Indications for the Transfusion of Blood Components Indications for transfusing blood and blood components must balance the potential benefits and known risks Most important risks Incompatibility non infectious complications and potential bacterial contamination

44
Hazards of transfusion A.Hemolytic Transfusion reaction B.Febrile Transfusion reaction C.Allergic Transfusion reaction D.Reaction due to infected blood E.Circulatory overload

45
Hazards of transfusion F.Transmission of diseases G.Transfusion Haemosiderosis H.complications of massive transfusion; I. Post-transfusion purpura J. Air Embolism K.Transfusion Related Acute Lung Injury

46
Hemolytic Transfusion Reaction DEFINITION ( by Mollison ) Occurance of signs of red cell destruction following transfusion the most obvious is Haemoglobinuria & jaundice
 Occurance of signs of red cell destruction following transfusion the most obvious is Haemoglobinuria & jaundice")
47
Hemolytic Transfusion Reaction (1). (1).Immune Haemolytic transfusion reaction Due to incompatible blood transfusion (a). Destruction of donor cells Due to specific alloAbs in patient’s ( recipient ‘s ) plasma ABO incompatibility cases more severe than Rh incompatibility
.Immune Haemolytic transfusion reaction Due to incompatible blood transfusion (a). Destruction of donor cells Due to specific alloAbs in patient’s ( recipient ‘s ) plasma ABO incompatibility cases more severe than Rh incompatibility.")
48
Hemolytic Transfusion Reaction Mechanism 1.Complement activitation - lysis 2. Coating of red cells by Ab - destruction by MPS Causes 1.Error in blood grouping & cross matching 2.Error in identification of blood or patient ( labeling )
.")
49
Pathophysiology Hypotension Vasoconstriction, renal ischemia Platelet activation intravascular haemolysis

50
Hemolytic Transfusion Reaction CLINICAL FEATURES Course of a severe immediate haemolytic reaction is typically characterized by four phases Phase of haemolytic shock Post shock phase in which the clinical features of increased blood destruction become obvious Oliguric phase Diuretic phase

51
CLINICAL FEATURES 1. Phase of haemolytic shock onset of symptoms varies with the rapidity of destruction Severe reactions occur particularly when the causative antibody is of high titre and activates complement, causing marked intravascular red cell destruction Hemolytic Transfusion Reaction

52
CLINICAL FEATURES 1.Phase of haemolytic shock Typical symptoms an aching pain in the lumbar region, sometimes in the thighs and down the legs flushing of the face, throbbing in the head, anxiety, precordial pain or constriction, breathlessness, nausea, vomiting, chills Hemolytic Transfusion Reaction

53
1.Phase of haemolytic shock rise in temperature tachycardia, and a fall in blood pressure haemorrhagic diathesis (DIC) – uncontrolled bleeding during surgery
 – uncontrolled bleeding during surgery")
54
Hemolytic Transfusion Reaction (2).Post shock phase : 1.Haemoglobinuria-transient &(+) in 1st specimen of urine 2.Jaundice 3.decreased Hb 4.Moderate leucocytosis
.Post shock phase : 1.Haemoglobinuria-transient &(+) in 1st specimen of urine 2.Jaundice 3.decreased Hb 4.Moderate leucocytosis")
55
Hemolytic Transfusion Reaction (3).Oliguric phase : Due to acute tubular necrosis A R F (4). Diuretic phase : Due to spontaneous diuresis loss of Na+, K+, water electrolyte imbalance

56
What to do? If an AHTR occurs STOP TRANSFUSION ABC’s Maintain IV access and run IVF (NS or RL) Monitor and maintain BP/pulse Give diuretic Obtain blood and urine for transfusion reaction Lab tests Send remaining blood back to Blood Bank
 Monitor and maintain BP/pulse Give diuretic Obtain blood and urine for transfusion reaction Lab tests Send remaining blood back to Blood Bank.")
57
Blood Bank Work-up of AHTR Check paperwork to assure no errors Check plasma for hemoglobin DAT Repeat crossmatch Repeat Blood group typing Blood culture

58
Labs found with AHTR Hemoglobinemia Hemoglobinuria Positive DAT Hyperbilirubinemia

59
Monitoring in AHTR Monitor patient clinical status and vital signs Monitor renal status (BUN, creatinine) Monitor coagulation status (DIC panel– PT/PTT, fibrinogen, D-dimer/FDP, Plt, Antithrombin-III) Monitor for signs of hemolysis (LDH, bili, haptoglobin)
 Monitor coagulation status (DIC panel– PT/PTT, fibrinogen, D-dimer/FDP, Plt, Antithrombin-III) Monitor for signs of hemolysis (LDH, bili, haptoglobin)")
60
Delayed haemolytic transfusion reaction 3 - 21 Days after transfusion S° immune response with increased Ab, extravascular destruction of red cells C/F; mild symptoms, fever, arthralgia, myalgia

61
Febrile Transfusion Reactions Definition- Rise in patient temperature >1°C (associated with transfusion without other fever precipitating factors) caused by alloantibodies directed against HLA antigens in multiparous females, in previously transfused patients
 caused by alloantibodies directed against HLA antigens in multiparous females, in previously transfused patients")
62
Allergic Transfusion Reactions C/F; Wheals, erythema, edema of face & mucous membrane, headache, Fever, nausea & vomiting rarely laryngeal oedema, & anaphylactic shock Causes : Causes : due to Anti Ig A Ab in patient’s circulation which react with Ig A in transfused plasma

63
CIRCULATORY OVERLOAD Acute pulmonary edema, sometime heart failure, cyanosis, dyspnoea Occur in chronic anaemia,elderly, very young, or cardiopulmonary d/s Prevention : Use packed cells Treatment : Diagoxin, Lasix, Morphine, O2

64
Reaction due to infected blood Bacterial infection of stored blood is a potential hazard in blood transfusions C/F: Septicemia (high fever, rigors, prostration, peripheral circulatory failure with persistent hypotension and tachycardia,vomiting, diarrhoea, and melaena)
")
65
Massive Transfusions Transfusion of 5 L or more over 24 Hours ( a) Citrate toxicity (b) K+ toxicity (c) Acid load - low pH (d) decreased calcium tremors, cardiac arrhythmias, abnormal ECG cardiac arrest
 Citrate toxicity (b) K+ toxicity (c) Acid load - low pH (d) decreased calcium tremors, cardiac arrhythmias, abnormal ECG cardiac arrest")
66
Transfusion Related Acute Lung Injury Clinical syndrome similar to ARDS Occurs 1-6 hours after receiving plasma- containing blood products Caused by WBC antibodies present in donor blood that result in pulmonary leukostasis Treatment is supportive High mortality

67
Transmission of infection A.Hepatitis B B.Hepatitis C C.HIV D.Bacterial Contamination/Sepsis E.HTLV 1/2 F.Malaria

68
TRANSFUSION HEMOSIDEROSIS Occur in repeated transfusion for anaemia without blood loss e.g.thalassaemia, aplastic anaemia, etc. Site: liver,spleen, B.M, Pancreas, Ht, Kidney, adrenal gland functional disturbance

69
Bone Marrow Transplantation Hematopoietic stem cell transplantation

70
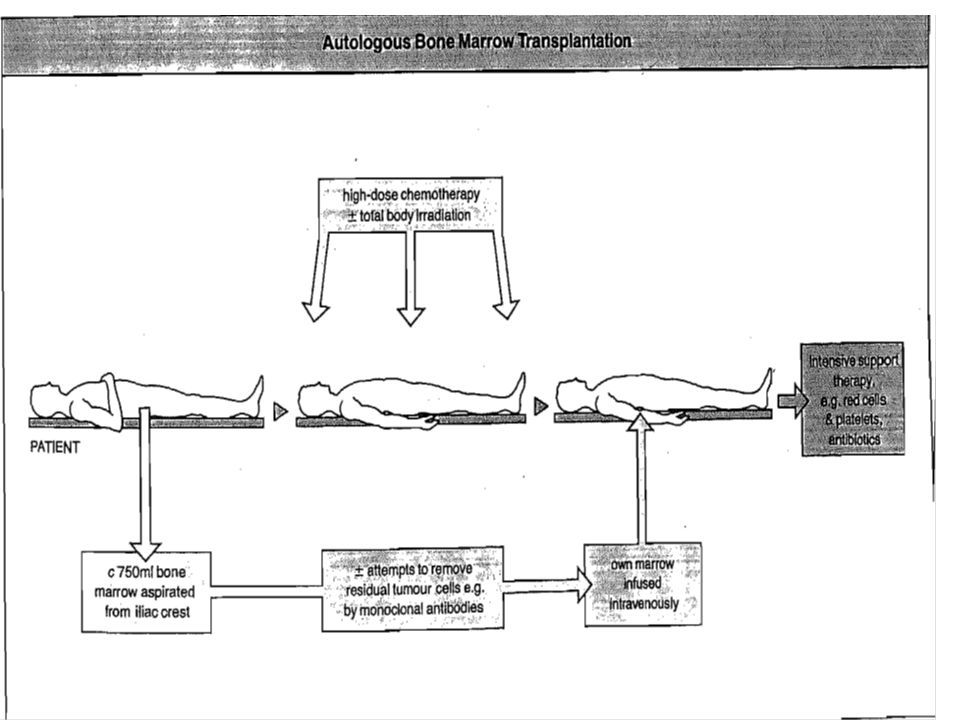
Types of Transplantation Allogeneic: from another person Syngeneic: from an identical twin Autologous: from the patient

71
Hematopoietic stem cell transplantation Intravenous infusion of autologous or allogeneic stem cells collected from bone marrow, peripheral blood or umbilical cord blood

72
Re-establish hematopoietic function in patients with damaged/defective bone marrow or immune systems Potentially curative for a wide variety of disorders Hematopoietic stem cell transplantation

73
Bone marrow transplantation used as therapy for Hematopoietic malignancies aplastic anemias Congenital immune deficiency states

74
HLA Typing HLA typing became feasible in 1960s Linked on chromosome 6 Inherited as haplotypes 1 in 4 chance a sibling will be identical

75
HLA Matching HLA loci on chromosome 6 HLA-A, HLA-B, HLA-C, HLA-DR, HLA- DQ, HLA-DP

76
Preparative Regimens Myeloablative High doses of chemotherapy +/- radiation 3 goals Eliminate malignancy Immunosuppression to allow engraftment Decrease graft versus host effects

77
Preparative Regimens Myeloablative Regimens Most common regimens Cyclophosphamide/TBI Busulfan/Cyclophosphamide

78
Preparative Regimens Nonmyeloablative Sufficient immunosuppression to allow donor cell engraftment Injury to organs less, fewer infections, fewer transfusions Higher relapse rates Graft versus tumor effects

79
Collection of Stem Cells Bone Marrow Harvest General anesthesia Equivalent of 50-100 bone marrow biopsies

80
Figure 2. The posterior iliac crests (arrows) are common sites for bone marrow aspiration and biopsy
 are common sites for bone marrow aspiration and biopsy.")
81
Collection of Stem Cells Stem Cell Collection (mobilization) Stem cells circulate in the blood Identified by CD34+ by flow cytometry Stem cells are collected through an apheresis catheter
 Stem cells circulate in the blood Identified by CD34+ by flow cytometry Stem cells are collected through an apheresis catheter")
84
Infusion of Stem Cells Stem cells may be infused fresh within a few hours of collection May be frozen Umbilical cord blood is obtained from one of the umbilical cord veins and frozen with an anticoagulant and nutrient media

85
Complications Graft Rejection by the host Acute graft-vs,-host disease (GVHD) Infections Chronic GVHD Prolonged immunodeficiency Disease recurrence
 Infections Chronic GVHD Prolonged immunodeficiency Disease recurrence")
Similar presentations












 – Leukocytes (WBCs) – Thrombocytes (platelets) Plasma – 90% water – 10% solutes – Proteins,>")
 for cell recognition (identification tags) The immune system has cells and chemicals.>")











.>")

 1958: Plastic bag of transfusion 1656: Initial theory and.>")
 CLS 245. What is Immunohematology? It is the study of Antigen-Antibody reaction as they relate to blood disorder.>")
