Download presentation
Presentation is loading. Please wait.

1
Upper Respiratory Tract Infections (URIs) Dr Simin Dashti-Khavidaki, Department of Pharmacotherapy, Tehran University of Medical Sciences
 Dr Simin Dashti-Khavidaki, Department of Pharmacotherapy, Tehran University of Medical Sciences")
2
Acute Otitis Media

3
Otitis Media (OM) n Most common reason for visit to pediatrician n Occurs in >75% of all children 2y/o n Peaks between 6mo-3yr
 n Most common reason for visit to pediatrician n Occurs in >75% of all children 2y/o n Peaks between 6mo-3yr")
5
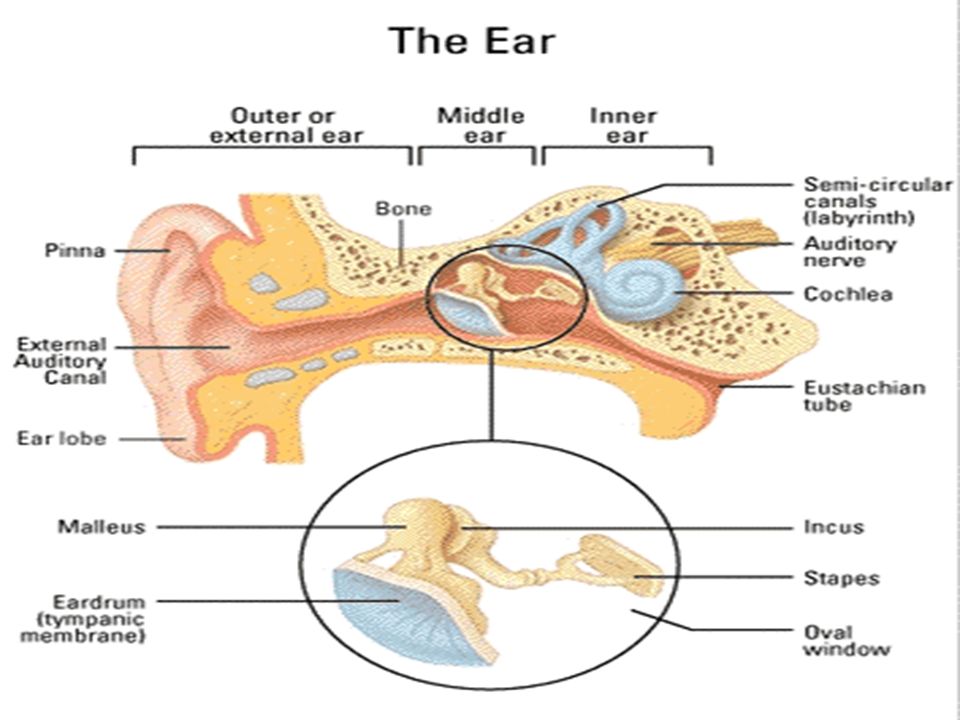
Otitis Media - Definition Inflammation of the middle ear

6
Acute Otitis Media: Sign & Symptoms n Otalgia (discomfort referable to the ears) n Irritability n With or without fever n Pts may experience nasal congestion, coughing, loss of appetite, vomiting, discharge from the ear
 n Irritability n With or without fever n Pts may experience nasal congestion, coughing, loss of appetite, vomiting, discharge from the ear")
7
Acute Otitis Media: Diagnosis 1) Recent, usually abrupt onset of S&S 2) Presence of MEE including: bulging, limited or absence motility of TM, otorrhea 3) S&S of middle ear inflammation including: erythema of TM, otalgia (discomfort referable to the ears and interference with normal activity or sleep)
 Recent, usually abrupt onset of S&S 2) Presence of MEE including: bulging, limited or absence motility of TM, otorrhea 3) S&S of middle ear inflammation including: erythema of TM, otalgia (discomfort referable to the ears and interference with normal activity or sleep)")
8
Recurrent otitis media n 3 episodes of AOM within 6mo period or 4 episodes within 1yr at least one of them within past 6 months

10
AAP 2013 n Clinicians should diagnose AOM in children who present with moderate to severe bulging of the TM or new onset of otorrhea not due to acute otitis externa.

11
AAP 2013 n Clinicians should diagnose AOM in children who present with mild bulging of the TM and recent (<48h) onset of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM.
 onset of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM.")
12
AAP 2013 n Clinicians should not diagnose AOM in children who do not have MEE (based on pneumatic otoscopy and/or tympanometry

13
Microbiology n S. pneumoniae - 30-35% n H. influenzae - 20-25% n M. catarrhalis - 10-15% n Group A strep - 2-4% n Infants with higher incidence of gram negative bacilli (esp E. coli)
.")
14
Virology n Up to 50% of AOM due to viruses n RSV - 74% of middle ear isolates n Rhinovirus n Parainfluenza virus n Influenza virus

15
Pain Management n The management of AOM should include an assessment of pain. If pain is present, the clinician should recommend treatment to reduce pain.

16
Pain Management n Analgesics and antipyretics –Acetaminophen: 10-15mg/kg/dose Q4-6h –Ibuprofen: 5-10mg/kg/dose Q6-8h, esp at night

17
AOM-Treatment Severe AOM n The clinician should prescribe antibiotic therapy for AOM (bilateral or unilateral) in children 6 months and older with severe signs or symptoms (ie, moderate or severe otalgia or otalgia for at least 48 hours, or T 39°C).
 in children 6 months and older with severe signs or symptoms (ie, moderate or severe otalgia or otalgia for at least 48 hours, or T 39°C).")
18
AOM-Treatment Nonsevere Bilateral AOM in Young Children n The clinician should prescribe antibiotic therapy for bilateral AOM in children <24 months without severe signs or symptoms (i.e., mild otalgia for less than 48 hours, T< 39°C.)
")
19
AOM Tx Nonsevere Unilateral AOM in Young Children n The clinician should either prescribe antibiotic therapy or offer observation with close follow-up based on joint decision-making with the parent(s)/caregiver for unilateral AOM in children 6-23 months of age without severe signs or symptoms (i.e., mild otalgia for less than 48 hours, T<39°C) n If wait and see, begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms.
/caregiver for unilateral AOM in children 6-23 months of age without severe signs or symptoms (i.e., mild otalgia for less than 48 hours, T<39°C) n If wait and see, begin antibiotic therapy if the child worsens or fails to improve within 48 to 72 hours of onset of symptoms.")
20
Nonsevere AOM in Older Children n The clinician should either prescribe antibiotic therapy or offer observation with close follow- up based on joint decision-making with the parent(s)/caregiver for AOM (bilateral or unilateral) in children 24 months without severe signs or symptoms (i.e., mild otalgia for <48 hours, T<39°C ).
/caregiver for AOM (bilateral or unilateral) in children 24 months without severe signs or symptoms (i.e., mild otalgia for <48 hours, T<39°C ).")
21
n Clinicians should prescribe amoxicillin for AOM when a decision to treat with antibiotics has been made and the child has not received amoxicillin in the past 30 days or the child does not have concurrent purulent conjunctivitis or the child is not allergic to penicillin

22
n Clinicians should prescribe an antibiotic with additional β-lactamase coverage for AOM when a decision to treat with antibiotics has been made, and the child has received amoxicillin in the last 30 days or has concurrent purulent conjunctivitis, or has a history of recurrent AOM unresponsive to amoxicillin.

23
n Clinicians should reassess the patient if the caregiver reports that the child’s symptoms have worsened or failed to respond to the initial antibiotic treatment within 48 to 72 hours and determine whether a change in therapy is needed.

24
AOM-Treatment in low-risk children ConditionRecommendedAlternative First line Standard-dose amoxicillin TMP-SMXAzithromycinClarithromycin Clinical failure after 48-72h High-dose amoxicillin or Co-amoxiclaveCefuroximecefixime

25
High-risk group n Day-care center attendance n Recent antibiotic use (within 30-60 d) n Resistance suspected n Recurrent AOM n Past/present Amoxicillin failure n Infant<6Mo n Immunosuppression n TM perforation/ tympanostomy tube n Chronic OM
 n Resistance suspected n Recurrent AOM n Past/present Amoxicillin failure n Infant<6Mo n Immunosuppression n TM perforation/ tympanostomy tube n Chronic OM")
26
AOM: Treatment in high-risk children ConditionRecommendedAlternative First line high-dose amoxicillin Cefuroxime (30-40mg/kg/d) Cefixime(8mg/kg/d) Ceftriaxone (50mg/kg/d) Clinical failure after 48-72h High-doseCo-amoxiclave Cefuroxime (40mg/kg/d) Cefixime (8mg/kg/d) IM Ceftriaxone(50mg/kg/d)
 Cefixime(8mg/kg/d) Ceftriaxone (50mg/kg/d) Clinical failure after 48-72h High-doseCo-amoxiclave Cefuroxime (40mg/kg/d) Cefixime (8mg/kg/d) IM Ceftriaxone(50mg/kg/d)")
27
AOM: Treatment duration n 10-14 days n Ceftriaxone 3 days

28
Notes n Cefexime: good activity against H.influenza and M. catarrhalis but less against S.pneumoniae n Cotrimoxazole: Resistance? n Azithromycin?

29
Recurrent AOM n Clinicians should not prescribe prophylactic antibiotics to reduce the frequency of episodes of AOM in children with recurrent AOM.

30
Recurrent AOM n Clinicians may offer tympanostomy tubes for recurrent AOM

31
Other Recommendations n Clinicians should recommend pneumococcal conjugate vaccine to all children and n annual influenza vaccine

32
Other Recommendations n Clinicians should encourage exclusive breastfeeding for at least 6 months

33
Other Recommendations n Clinicians should encourage avoidance of tobacco smoke exposure

34
Other Recommendations n Xylitol n Sweetening substitute n Inhibits growth of pneumococcus and inhibits adhesion of pneumococcus and H. flu in nasopharynx n Gum and syrup reduced incidence of AOM 40% and 30%

35
Sinusitis

36
Sinusitis: predisposing factors n Viral URI (80%) n Allergic inflammation (20%) n Immune deficiency n Asthma n GERD
 n Allergic inflammation (20%) n Immune deficiency n Asthma n GERD")
37
Sinusitis: Sign & Symptoms

38
n H/A n Fever n Sneezing n Coughing n Runny nose n halitosis n Purulent nasal discharge n Erythematous throat

39
Sinusitis: paraclinics n CBC/diff n CT-scan: for >6yo, persistent or recurrent infection, not responsive to medical management

40
Sinusitis: microbiology n Middle ear cavity is also a paranasal sinus; the pathogenesis and microbiology of AOM and acute bacterial sinusitis are similar

41
Sinusitis: definition n Acute bacterial sinusitis: bacterial infection of the paranasal sinuses lasting less than 30 days in which symptoms resolve completely n Subacute bacterial sinusitis: lasting 30-90 days n Recurrent acute bacterial sinusitis n Chronic sinusitis: >90 days persistent symptoms e.g. cough, rhinirrhea or nasal obstruction

42
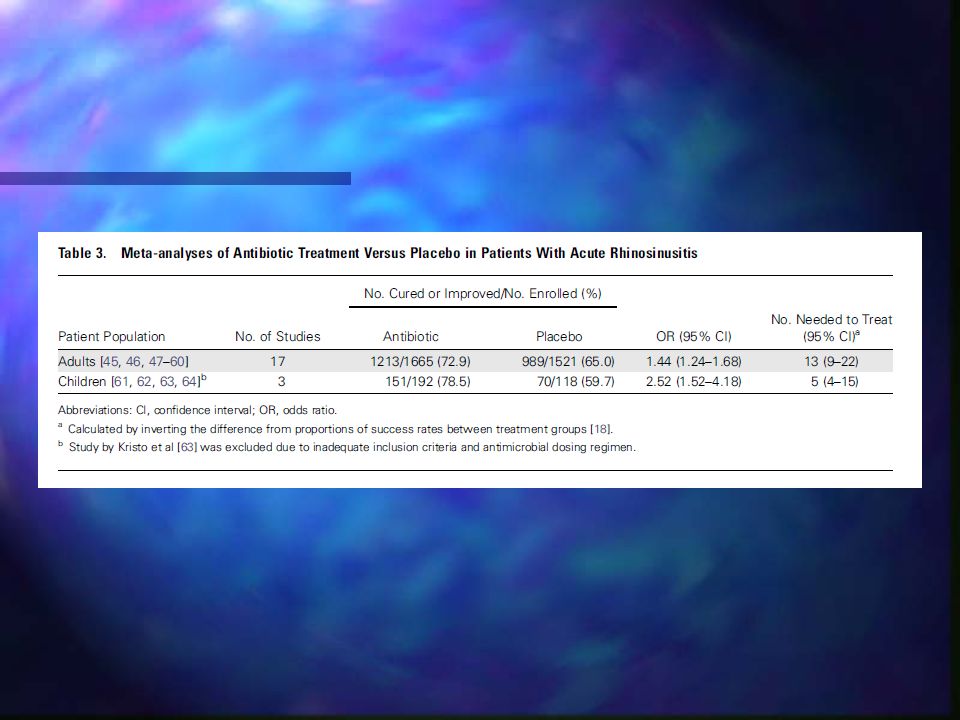
Acute bacterial sinusitis n Acute bacterial sinusitis follows upper (usually viral) respiratory tract infection in 0.5% to 5% of cases. n It is usually caused by: n Streptococcus pneumoniae n Haemophilus influenzae n Moraxella catarrhalis

59
Pharyngitis

60
Pharyngitis: Signs & Symptoms n Fever, fatigue n Nausea n Sore throat usually beginning after woke up one morning n Swollen lymph glands in the back of neck

61
Pharyngitis: Signs & Symptoms n Throat, palate (roof of mouth) and tonsils are red n Tonsil may have white exudate patches (covering) n Rash (scarlet fever) which looks like a sunburn with fine red dots n Tongue may become “strawberry’ looking appearance
 and tonsils are red n Tonsil may have white exudate patches (covering) n Rash (scarlet fever) which looks like a sunburn with fine red dots n Tongue may become strawberry’ looking appearance")
65
Pharyngitis: microbiology n Viral (adenovirus, enterovirus, parainfluenza, influenza, EBV); n in <2yo pts most pharyngitis are viral n Bacterial (30% of cases): Group A Hemolytic Streptococci (GABHS) (S.pyogenes) the most common bacteria in 5-15 y/o
; n in <2yo pts most pharyngitis are viral n Bacterial (30% of cases): Group A Hemolytic Streptococci (GABHS) (S.pyogenes) the most common bacteria in 5-15 y/o")
68
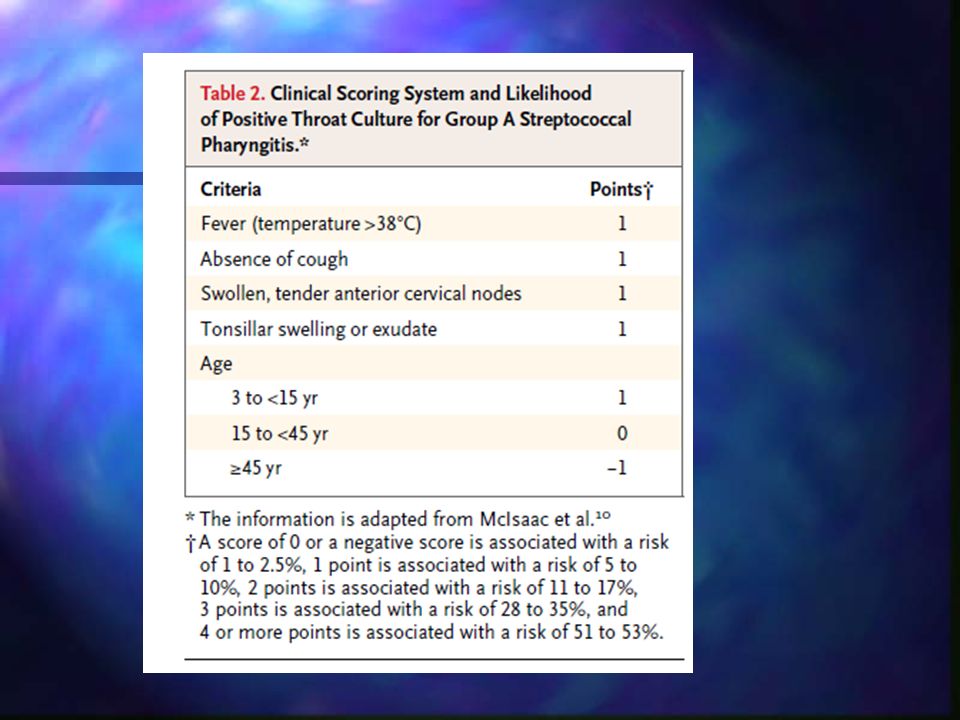
Management of Pharyngitis Predictor Score n Fever>36.1 C +3/degree n Recent exposure to strep inf. +17 n Recent cough - 7 n Pharyngeal exudate + 6 n Tender cervical adenopathy +11

69
Management of Pharyngitis Total Score Strep P.(%) Decision n -10 to 0 1.8 No Rx n +1 to 10 4.6 No Rx n +11 to 20 18 Culture n +21 to 30 19 Culture n +31 to 40 44 Rx n > + 41 100 Rx
 Decision n -10 to No Rx n +1 to No Rx n +11 to Culture n +21 to Culture n +31 to Rx n > Rx")
71
SYMPTOMATIC THERAPY n Warm saline gargles n Rest n Analgesics : Ibuprofen ; Acetaminophen n Liquids

Similar presentations





























>")






. >")
 is inflammation.>")