Download presentation
Presentation is loading. Please wait.

1
Chad J. Muxlow, D.O. ORV Journal Club January 2013

2
Overview Histology of bone Biology Bone Matrix Blood Supply Repair/Remodeling

3
Types of Bone Lamellar mature Woven Immature Pathologic

4
Organized Stress oriented (Wolff’s Law) Less Cellular Increased Strength
 Less Cellular Increased Strength")
5
Cortical bone Cancellous bone (trabecular or spongy bone) Bony struts (trabeculae) that are oriented in direction of the greatest stress
 Bony struts (trabeculae) that are oriented in direction of the greatest stress")
6
Immature Pathologic Weak Random More cellular Not stress oriented

7
Coarse with random orientation Weaker than lamellar bone Normally remodeled to lamellar bone Figure from Rockwood and Green’s: Fractures in Adults, 4 th ed

8
Less Dense More Elastic Smaller Young’s Modulus Higher turnover Found in metaphysis and epiphysis of long bones and in cuboid bones (vertebrae)
")
9
80% of skeleton High Young’s Modulus Slow turnover rate Increased torsional and bending resistance - Found in diaphysis of long bones and envelopes cuboid bones

10
Composed of vascular channels circumferentially surrounded by lamellar bone (aka osteon complex arrangement of bone around the vascular channel) Osteon are usually oriented in the long axis of the bone Cortical bone = a complex of many adjacent osteons and their interstitial and circumferential lamellae
 Osteon are usually oriented in the long axis of the bone Cortical bone = a complex of many adjacent osteons and their interstitial and circumferential lamellae")
11
Haversian canal: central canal of an osteon, containing cells, vessels and nerves Volkmann’s canal: connects osteons Cement line: boundaries of an osteon Lacuna: where osteocytes live and connect to each other via cannaliculi

12
Osteon with central haversian canal containing Cells Vessels Nerves Volkmann’s canal Connects osteons osteon Haversian canal osteocyte Volkmann’s canal

13
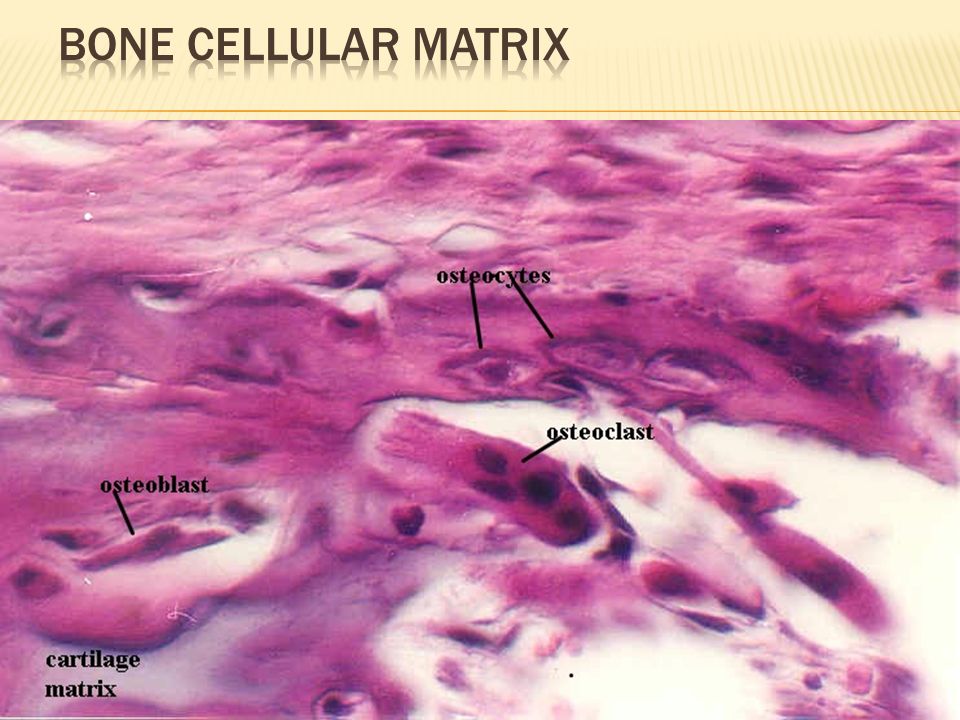
Cells Osteoblasts Ostocytes Osteoclasts Osteoprogenitor cells Extracellular Matrix Organic (4o%) Collagen (type I) 90% Osteocalcin, osteonectin, proteoglycans, glycosaminoglycans, lipids (ground substance) Inorganic (60%) Primarily hydroxyapatite Ca 10 (PO 4 ) 6 (OH) 2
 Collagen (type I) 90% Osteocalcin, osteonectin, proteoglycans, glycosaminoglycans, lipids (ground substance) Inorganic (60%) Primarily hydroxyapatite Ca 10 (PO 4 ) 6 (OH) 2")
14
Derived from mesenchymal stem cells Responsive to PTH Produce bone matrix type 1 collagen Osteocalcin, bone sialoprotein extracellular matrix proteins specific to bone Line the surface of bone and follow osteoclasts in cutting cones

15
PTH Estrogen Glucocorticoids Vitamin D

16
Derived from osteoblasts (osteoblasts that are encased in mineralized matrix) 90% of cells in mature skeleton Maintain bone
 90% of cells in mature skeleton Maintain bone")
17
Derived from hematopoietic stem cells (monocyte precursor cells) Multinucleated cells whose function is bone resorption Reside in bone resorption pits (Howship’s lacunae) Parathyroid hormone stimulates receptors on osteoblasts that activate osteoclastic bone resorption
 Multinucleated cells whose function is bone resorption Reside in bone resorption pits (Howship’s lacunae) Parathyroid hormone stimulates receptors on osteoblasts that activate osteoclastic bone resorption")
18
Ruffled border Attach to bone via integrins Specific calcitonin receptors inhibits bone resorption Metastatic bone disease Interacts with osteoblasts via RANKL pathway

19
IL-1 stimulator Calcitonin inhibitor Bisphosphonates Disrupt the ruffled border PTH (indirect osteoclast stimulator)
")
22
Tensile strength of bone Type I collagen 90% organic matrix 5% Type III and IV

23
Osteocalcin – most abundant noncollagenous matrix protein Osteonectin – role in Ca regulation Osteopontin – similar to integrins

24
Calcium Hydroxyapatite Compressive strength Osteocalcium Phosphate

25
Bone receives 5-10% of cardiac output 3 sources nutrient artery metaphyseal/epiphyseal periosteal Nutrient artery Metaphyseal vessels Periosteal vessels

26
Nutrient artery enters diaphyseal cortex through nutrient foramen branches into ascending and descending arteries inner 2/3 of cortex high pressure Blood Supply to Bone

27
Metaphyseal/epiphyseal arises from periarticular vascular plexus Periosteal system outer 1/3 of cortex low pressure

28
Response to mechanical stress Wolff’s Law Piezoelectric Charges Compression side – electronegative Stimulates osteoblasts Tension side – electropositive Stimulates osteoclasts

29
Hueter-Volkmann Law Compression – inhibits growth Tension – stimulates growth

30
Cutting Cones Intramembranous Bone Formation Endochondral Bone Formation

31
Primarily a mechanism to remodel bone Osteoclasts at the front of the cutting cone remove bone Trailing osteoblasts lay down new bone

32
Mechanism by which a long bone grows in width Osteoblasts differentiate directly from preosteoblasts and lay down seams of osteoid Does NOT involve cartilage precursor Examples Embryonic flat bones (pelvis, clavicle, vault of skull) Distraction osteogenesis
 Distraction osteogenesis")
34
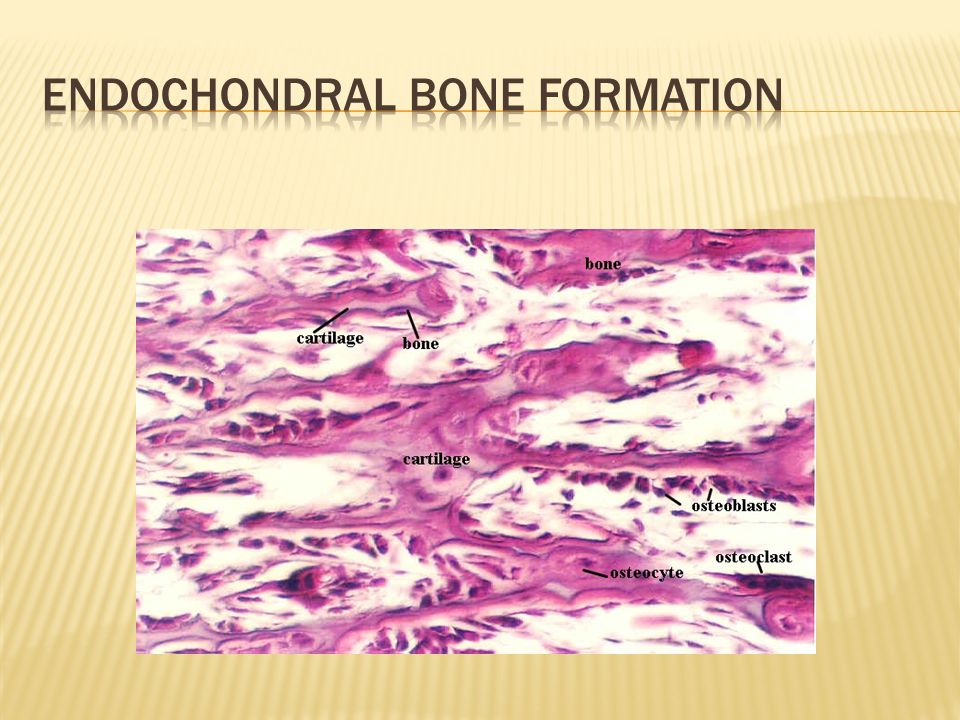
Mechanism by which a long bone grows in length Bone replaces cartilage The chondrocytes hypertrophy, degenerate and calcify (area of low oxygen tension) Vascular invasion of the cartilage occurs followed by ossification (increasing oxygen tension) Examples Embryonic long bone formation Physis Fracture callus DMB matrix
 Vascular invasion of the cartilage occurs followed by ossification (increasing oxygen tension) Examples Embryonic long bone formation Physis Fracture callus DMB matrix")
36
Adequate blood supply Adequate mechanical stability

37
Fracture stimulates the release of growth factors that promote angiogenesis and vasodilation Blood flow is increased substantially to the fracture site Peaks at two weeks after fracture

38
Early stability promotes revascularization After first month, loading and interfragmentary motion promotes greater callus formation

39
Mechanical load and small displacements at the fracture site stimulate healing Inadequate stabilization may result in excessive deformation at the fracture site interrupting tissue differentiation to bone (soft callus) Over-stabilization, however, reduces periosteal bone formation (hard callus)
 Over-stabilization, however, reduces periosteal bone formation (hard callus)")
40
Inflammation Repair Remodeling

41
Tissue disruption results in hematoma at the fracture site Local vessels thrombose causing bony necrosis at the edges of the fracture Increased capillary permeability results in a local inflammatory milieu Osteoinductive growth factors stimulate the proliferation and differentiation of mesenchymal stem cells

42
Periosteal callus forms along the periphery of the fracture site Intramembranous ossification initiated by preosteoblasts Intramedullary callus forms in the center of the fracture site Endochondral ossification at the site of the fracture hematoma Chemical and mechanical factors stimulate callus formation and mineralization

43
Figure from Brighton, et al, JBJS-A, 1991.

44
Woven bone is gradually converted to lamellar bone Medullary cavity is reconstituted Bone is restructured in response to stress and strain (Wolff’s Law)
")
45
Direct (primary) bone healing Indirect (secondary) bone healing
 bone healing Indirect (secondary) bone healing")
46
Mechanism of bone healing seen when there is no motion at the fracture site (i.e. rigid internal fixation) Does not involve formation of fracture callus Osteoblasts originate from endothelial and perivascular cells
 Does not involve formation of fracture callus Osteoblasts originate from endothelial and perivascular cells.")
47
A cutting cone is formed that crosses the fracture site Osteoblasts lay down lamellar bone behind the osteoclasts forming a secondary osteon Gradually the fracture is healed by the formation of numerous secondary osteons A slow process

48
Contact Healing Direct contact between the fracture ends allows healing to be with lamellar bone immediately Gap Healing Gaps less than 200-500 microns are primarily filled with woven bone that is subsequently remodeled into lamellar bone Larger gaps are healed by indirect bone healing (partially filled with fibrous tissue that undergoes secondary ossification)
")
49
Figure from http://www.vetmed.ufl.edu/sacs/notes

50
Mechanism for healing in fractures that are not rigidly fixed. Bridging periosteal (soft) callus and medullary (hard) callus re-establish structural continuity Callus subsequently undergoes endochondral ossification Process fairly rapid - weeks
 callus and medullary (hard) callus re-establish structural continuity Callus subsequently undergoes endochondral ossification Process fairly rapid - weeks.")
51
Type of StabilizationPredominant Type of Healing Cast (closed treatment)Periosteal bridging callus and interfragmentary enchondral ossification Compression platePrimary cortical healing (cutting cone–type or haversian remodeling) Intramedullary nailEarly: periosteal bridging callus; enchondral ossification Late: medullary callus and intramembranous ossification External fixatorDependent on extent of rigidity: - Less rigid: periosteal bridging callus; enchondral ossification - More rigid: primary cortical healing; intramembranous ossification Inadequate immobilization with adequate blood supply Hypertrophic nonunion (failed enchondral ossification); type II collagen predominates Inadequate immobilization without adequate blood supply Atrophic nonunion Inadequate reduction with displacement at the fracture site Oligotrophic nonunion TYPE OF FRACTURE HEALING BASED ON TYPE OF STABILIZATION
Periosteal bridging callus and interfragmentary enchondral ossification Compression platePrimary cortical healing (cutting cone–type or haversian remodeling) Intramedullary nailEarly: periosteal bridging callus; enchondral ossification Late: medullary callus and intramembranous ossification External fixatorDependent on extent of rigidity: - Less rigid: periosteal bridging callus; enchondral ossification - More rigid: primary cortical healing; intramembranous ossification Inadequate immobilization with adequate blood supply Hypertrophic nonunion (failed enchondral ossification); type II collagen predominates Inadequate immobilization without adequate blood supply Atrophic nonunion Inadequate reduction with displacement at the fracture site Oligotrophic nonunion TYPE OF FRACTURE HEALING BASED ON TYPE OF STABILIZATION")
52
Growth FactorActionNotes Bone morphogenetic protein (BMP) Osteoinductive; stimulates bone formation Induces metaplasia of mesenchymal cells into osteoblasts Target cells of BMP are the undifferentiated perivascular mesenchymal cells; signal through serine/threonine kinase receptors. Intracellular molecules called SMADs serve as signaling mediators for BMPs. Transforming growth factor-β (TGF-β) Induces mesenchymal cells to produce type II collagen and proteoglycans Found in fracture hematomas; believed to regulate cartilage and bone formation in fracture callus; signal through serine/threonine kinase receptors Induces osteoblasts to synthesize collagen Coating porous implants with TGF-β enhances bone ingrowth. Insulin-like growth factor II (IGF-II) Stimulates type I collagen, cellular proliferation, cartilage matrix synthesis, and bone formation Signal through tyrosine kinase receptors Platelet-derived growth factor (PDGF) Attracts inflammatory cells to the fracture site (chemotactic) Released from platelets; signal through tyrosine kinase receptors GROWTH FACTORS OF BONE
 Induces mesenchymal cells to produce type II collagen and proteoglycans Found in fracture hematomas; believed to regulate cartilage and bone formation in fracture callus; signal through serine/threonine kinase receptors Induces osteoblasts to synthesize collagen Coating porous implants with TGF-β enhances bone ingrowth. Insulin-like growth factor II (IGF-II) Stimulates type I collagen, cellular proliferation, cartilage matrix synthesis, and bone formation Signal through tyrosine kinase receptors Platelet-derived growth factor (PDGF) Attracts inflammatory cells to the fracture site (chemotactic) Released from platelets; signal through tyrosine kinase receptors GROWTH FACTORS OF BONE.")
53
4 Properties Osteoconductive matrix—Acts as a scaffold or framework into which bone growth occurs Osteoinductive factors—Growth factors such as bone morphogenetic protein (BMP) and transforming growth factor-β (TGF-β that signal local factors to stimulate bone formation Osteogenic cells—Include primitive mesenchymal cells, osteoblasts, and osteocytes Structural integrity
 and transforming growth factor-β (TGF-β that signal local factors to stimulate bone formation Osteogenic cells—Include primitive mesenchymal cells, osteoblasts, and osteocytes Structural integrity")
54
Osteoarticular (osteochondral): immunogenic (cartilage is vulnerable to inflammatory mediators of immune response [cytotoxicity from antibodies and lymphocytes]); articular cartilage is preserved with glycerol or dimethyl sulfoxide (DMSO); and cryogenically preserved grafts leave few viable chondrocytes. Tissue-matched (syngeneic) osteochondral grafts produce minimal immunogenic effects and incorporate well. Vascularized bone grafts: allow more rapid union and cell preservation; best for irradiated tissues or large tissue defects (may be donor site morbidity)
![ Osteoarticular (osteochondral): immunogenic (cartilage is vulnerable to inflammatory mediators of immune response [cytotoxicity from antibodies and lymphocytes]); articular cartilage is preserved with glycerol or dimethyl sulfoxide (DMSO); and cryogenically preserved grafts leave few viable chondrocytes.](http://images.slideplayer.com/35/10288177/slides/slide_54.jpg "Tissue-matched (syngeneic) osteochondral grafts produce minimal immunogenic effects and incorporate well. Vascularized bone grafts: allow more rapid union and cell preservation; best for irradiated tissues or large tissue defects (may be donor site morbidity).")
55
Nonvascular bone grafts are more common than vascularized grafts Allograft bone: Type of Allograft fresh—increased immunogenicity fresh-frozen—less immunogenic than fresh BMP preserved freeze-dried (lyophilized)—loses structural integrity and depletes BMP, least immunogenic, purely osteoconductive, and lowest likelihood of viral transmission, commonly known as “croutons.” bone matrix gelatin (BMG, a digested source of BMP)—demineralized bone matrix (Grafton) is osteoconductive and osteoinductive
—loses structural integrity and depletes BMP, least immunogenic, purely osteoconductive, and lowest likelihood of viral transmission, commonly known as croutons. bone matrix gelatin (BMG, a digested source of BMP)—demineralized bone matrix (Grafton) is osteoconductive and osteoinductive")
56
Cortical bone grafts—Slower incorporation through remodeling of existing haversian systems via resorption (weakens the graft) followed by deposition of new bone (restores strength). Used for structural defects. Cancellous grafts—Revascularize and incorporate quickly; osteoblasts lay down new bone on old trabeculae, which are later remodeled (“creeping substitution”). Allografts must be harvested with a sterile technique, and donors must be screened for potential transmissible diseases
. Allografts must be harvested with a sterile technique, and donors must be screened for potential transmissible diseases.")
57
Silicate-based grafts—Incorporate the element silicon (Si) as silicate (silicon dioxide): bioactive glasses and glass-ionomer cement Calcium phosphate–based grafts—Capable of osseoconduction and osseointegration. These materials biodegrade at a very slow rate. Many are prepared as ceramics (heated apatite crystals fuse into crystals [sintered]). Tricalcium phosphate Hydroxyapatite (e.g., Collagraft Bone Graft Matrix [Zimmer, Inc, Warsaw, IN]); purified bovine dermal fibrillar collagen plus ceramic hydroxyapatite granules and tricalcium phosphate granules Calcium sulfate—Osteoconductive (e.g., OsteoSet [Wright Medical Technology Inc., Arlington, TN]). Calcium carbonate (chemically unaltered marine coral)—Is resorbed and replaced by bone (osteoconductive) (e.g., Biocora [Inoteb, France]). Coralline hydroxyapatite—Calcium carbonate skeleton is converted to calcium phosphate via a thermoexchange process (e.g., Interpore 200 and 500 [Interpore Orthopaedics, Irvine, CA]).
. Tricalcium phosphate Hydroxyapatite (e.g., Collagraft Bone Graft Matrix [Zimmer, Inc, Warsaw, IN]); purified bovine dermal fibrillar collagen plus ceramic hydroxyapatite granules and tricalcium phosphate granules Calcium sulfate—Osteoconductive (e.g., OsteoSet [Wright Medical Technology Inc., Arlington, TN]). Calcium carbonate (chemically unaltered marine coral)—Is resorbed and replaced by bone (osteoconductive) (e.g., Biocora [Inoteb, France]). Coralline hydroxyapatite—Calcium carbonate skeleton is converted to calcium phosphate via a thermoexchange process (e.g., Interpore 200 and 500 [Interpore Orthopaedics, Irvine, CA])..")
58
Properties GraftOsteoconductionOsteoinduction Osteogenic Cells Structural IntegrityOther Properties Autograft CancellousExcellentGoodExcellentPoorRapid incorporation CorticalFair ExcellentSlow incorporation AllograftFair NoneGood Fresh has the highest immunogenicity Freeze-dried is the least immunogenic but has the least structural integrity (weakest) Fresh-frozen preserves BMP CeramicsFairNone Fair Demineralized bone matrix FairGoodNonePoor Bone marrowPoor GoodPoor TYPES OF BONE GRAFTS AND BONE GRAFT PROPERTIES
 Fresh-frozen preserves BMP CeramicsFairNone Fair Demineralized bone matrix FairGoodNonePoor Bone marrowPoor GoodPoor TYPES OF BONE GRAFTS AND BONE GRAFT PROPERTIES")
Similar presentations



 Periosteum is external surface Endosteum lines internal surfaces Mineral component.>")




 called osteoid.>")












