Download presentation
Presentation is loading. Please wait.

1
scabies

2
Scabies is the term for infestation with the itch mite, Sarcoptes scabiei var humanus. The mite was first described in 1687, making scabies one of the first infectious diseases with a known cause. The disease is found worldwide, in all races and in all age groups. It can be transmitted sexually as well as by nonsexual close skin-to-skin contact, especially within the family and at school. When more than one member of a household is afflicted with an intensely pruritic eruption, scabies infestation must be considered.

3
CLASSIC SCABIES The hallmark of scabies is intractable pruritus, characteristically more severe at night. The itching, often disproportionately severe, is associated with lesions that initially appear on the web spaces, then the sides of the fingers, the flexor surfaces of the wrists, elbows and anterior axillary folds. Other common sites of lesions are the penis and scrotum, the areolae in women, the buttocks, and the sacral and periumbilical areas. Lesions may be eczematous and often are excoriated, but the pathognomonic lesion is the burrow ( , a short, wavy, dark line. The classical features are often obscured by excoriations.

4
SPECIAL FORMS Orkin described presentations of scabies that may present diagnostic difficulties or may suggest the diagnosis. Scabies in patients with good hygiene Easily misdiagnosed because lesions are sparse and burrows difficult to find. Scabies incognito Originally described in patients taking glucocorticoids, other immunosuppressive drugs also may lead to confusing presentations of scabies, including crusted scabies mimicking contact dermatitis or Darier's disease. Scabies must be considered whenever a widespread, scaly, pruritic dermatosis develops in an immunosuppressed patient.

5
Nodular scabies The lesions are reddish-brown, pruritic papules and nodules on covered areas (most frequently the male genitalia, groin, and axillary regions), which often persist long after adequate treatment for scabies. They probably represent a hypersensitivity reaction to retained mite parts or antigens.

6
Scabies in infants and young children In this age group, the face, scalp, palms, and soles may be involved; the most common presenting lesions are still papules, vesicopustules, and nodules, but the distribution may be atypical. Secondary eczematization and impetigenization are common, and burrows difficult to find. The prevalence of scabies is highest in infants younger than 2 years of age; the youngest child in the household is often affected because he or she is carried and hugged by affected adults .

7
Scabies in the elderly In this age group, scabies may be missed because the cutaneous changes may be minimal or atypical. The intense itching may be attributed to “senile pruritus,” xerosis, drugs or psychogenic causes. Older patients who spend prolonged periods of time in bed or in chairs may have involvement of the back. Scabies epidemics are frequently reported in group care facilities such as nursing homes, where a single patient with crusted scabies may be the index case leading to infection of other patients as well as health care workers and their families.

8
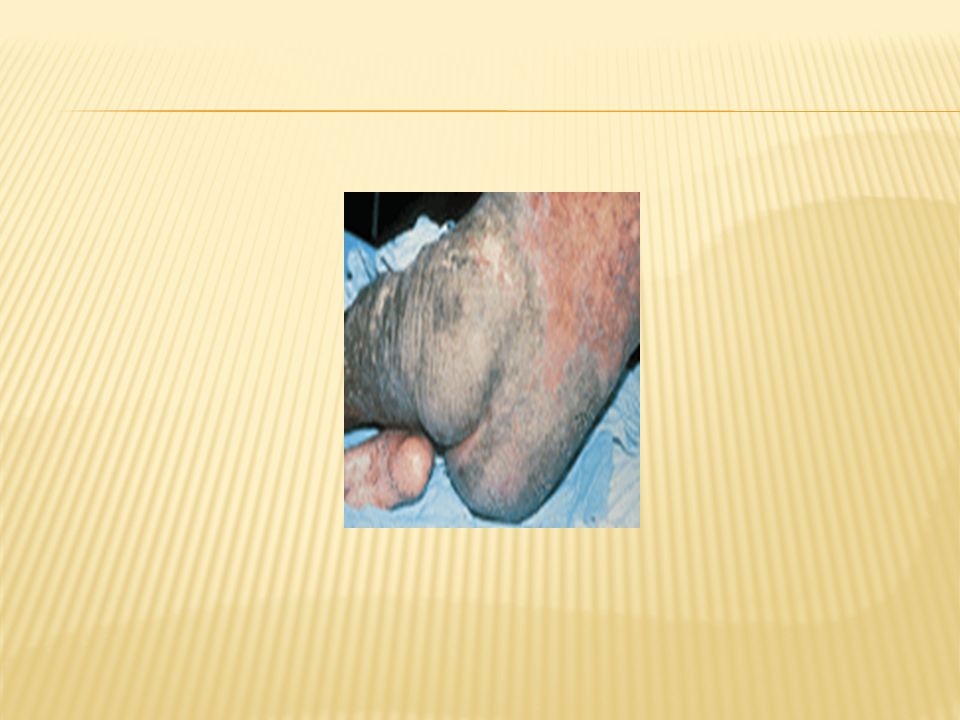
Crusted (Norwegian) scabies Historically, this condition has been associated with advanced age, debility, and developmental disabilities such as Down's syndrome. It is now also seen with immunosuppression of all types. Hyperkeratotic, nonpruritic lesions are most common, but the condition may range from crusting with or without pruritus to a pruritic, papular dermatitis and may mimic Darier's disease or psoriasis. Finger- and toenail involvement may simulate psoriasis or onychomycosis. Thousands to millions of organisms may be present in the scales and the nails.

9
In the absence of other predisposing conditions, patients with crusted scabies should be tested for AIDS. Patients with crusted scabies have developed bacteremias—occasionally fatal—as a consequence of infection of the fissured and excoriated skin.

11
Scabies of the scalp Scabies rarely involves the adult scalp; when it does, it may accompany or simulate seborrheic dermatitis. However, scalp lesions do occur in infants and children, the elderly, nursing home patients, those residing in tropical areas, and patients with crusted scabies, AIDS and, recently reported, patients with dermatomyositis.

12
Bullous scabies Vesicles are common in children with scabies but uncommon in adults. Bullous scabies may occur in adults, associated with an eruption indistinguishable from bullous pemphigoid clinically.

13
Differential Diagnosis
Scabies can be confused with almost any pruritic dermatosis but is most commonly confused with atopic dermatitis, papular urticaria, pyodermas, insect bites, and dermatitis herpetiformis.

14
Diagnosis Burrows are often difficult to find, and the usual clue to the diagnosis is the characteristic distribution; in males, papules, nodules and, rarely, ulcers on the penis, are a significant diagnostic feature. Definitive diagnosis rests on microscopic identification of the mites, eggs, or fecal pellets ( scyballa). Often mites cannot be found in spite of classical lesions of nodular scabies on the genitalia, or the typical rash with a history of other family members itching. It may be appropriate to treat such a patient with a presumptive diagnosis, but both overdiagnosis and underdiagnosis are common .
. Often mites cannot be found in spite of classical lesions of nodular scabies on the genitalia, or the typical rash with a history of other family members itching. It may be appropriate to treat such a patient with a presumptive diagnosis, but both overdiagnosis and underdiagnosis are common .")
15
DIRECT EXAMINATI On One or two drops of mineral oil are applied to the lesion, which is scraped or shaved with a scalpel blade to remove the tops of the burrows or papules. The scrapings, along with the oil, covered with a coverslip, are examined microscopically under low power. Potassium hydroxide should not be used, because it can dissolve the fecal pellets ( scyballa).
.")
16
POLYMERASE CHAIN REACTION Bezold et al
POLYMERASE CHAIN REACTION Bezold et al. reported the use of PCR to prove scabies in a patient presenting with clinically atypical eczema. Epidermal scales were PCR positive for S. scabiei DNA before, and negative 2 weeks after, therapy.

17
Treatment Scabicides should be applied thoroughly to the area behind the ears and from neck to soles, with special attention to intertrigenous areas such as between the fingers and the toes, the umbilicus, the groin, between the buttocks, and under the fingernails and toenails. Medication should be thoroughly washed off after the recommended time period. The morning after treatment, underwear, bed linens, and towels should be machine-washed and dried, using the hot cycles.

18
Patients should be cautioned that while the infestation has been adequately treated, itching and eczematization might persist for up to a month. All members of the affected household should receive topical treatment, although some physicians treat only those asymptomatic family members who have intimate contact with the patient (sharing a bed, sexual contact).
.")
19
SPECIFIC TOPICAL SCABICIDES Permethrin 5% cream (Elimite, Acticin), a synthetic pyrethroid, is an excellent scabicide, with low toxicity in humans even with overuse. It is minimally absorbed and rapidly metabolized. The cream is applied as described above and left on overnight. Many physicians prefer to use a second application 5 to 7 days later. Clinically significant resistance (properly termed tolerance) has not been reported. Permethrin should not be used in infants younger than 2 months of age or in pregnant or nursing women. The most common adverse reactions are mild and transient; burning, stinging or exacerbation or recurrence of pruritus, and rarely contact dermatitis may occur.
 has not been reported. Permethrin should not be used in infants younger than 2 months of age or in pregnant or nursing women. The most common adverse reactions are mild and transient; burning, stinging or exacerbation or recurrence of pruritus, and rarely contact dermatitis may occur.")
20
Lindane is left on for 8 h and then washed off
Lindane is left on for 8 h and then washed off. As with permethrin, some physicians prefer to retreat 1 week later. Central nervous system toxicity may occur, generally because of failure to follow instructions, either because too much of the medication was applied or it was applied too many times. Lindane should not be used in infants, young children, or pregnant or nursing women, or in patients with seizure disorders or other neurologic diseases. Clinically significant tolerance to lindane has not been reported.

21
Sulfur, usually prescribed as precipitated sulfur (6%) in petrolatum, must be compounded by the pharmacist. It may be applied nightly for 3 nights and washed off thoroughly 24 h after the last application. It smells, stains, and is greasy, but it is safe, effective. Crotamiton cream (Eurax) is not believed to be highly effective in the treatment of scabies; it is inferior to permethrin, but may be about as effective as benzyl benzoate and sulfur. Benzyl Benzoate 25% is an effective scabicide, but is not commercially available in the United States. It is probably as effective as lindane.
 is not believed to be highly effective in the treatment of scabies; it is inferior to permethrin, but may be about as effective as benzyl benzoate and sulfur. Benzyl Benzoate 25% is an effective scabicide, but is not commercially available in the United States. It is probably as effective as lindane.")
22
IVERMECTIN Ivermectin is an antiparasitic agent, approved by the FDA for onchocerciasis and strongyloidiasis in humans. Since 1993, there have been numerous reports indicating that ivermectin given in one or two oral doses of 200 μg/kg body weight is an effective treatment for scabies.

23
The pruritus of scabies often persists for several weeks after adequate therapy. Sedating antihistamines may reduce the pruritus, but a short course of topical or systemic glucocorticoids is generally more effective. In children, 1% hydrocortisone cream may be helpful; in adults triamcinolone cream (0.1%) may be used. For more severe itching, a 7- to 14-day course of prednisone or intramuscular triamcinolone acetonide, 40 to 60 mg, may give relief. Where excoriation has led to impetiginization, antibiotic therapy with topical mupirocin or a broad-spectrum antibiotic is appropriate.
 may be used. For more severe itching, a 7- to 14-day course of prednisone or intramuscular triamcinolone acetonide, 40 to 60 mg, may give relief. Where excoriation has led to impetiginization, antibiotic therapy with topical mupirocin or a broad-spectrum antibiotic is appropriate.")
24
CRUSTED SCABIES The scabicides used for classical scabies are effective in crusted scabies as well; however, repeated applications are usually required, clearing is slower than in noncrusted scabies, and sometimes the sequential use of two or more different agents is necessary. The entire skin should be treated, including the scalp, face (excluding the areas around the eyes, nose, and mouth), and particularly under the fingernails and toenails, brushing the medication under the free edges of the nails. Ivermectin, 200 to 250 μg/kg of body weight may be appropriate, alone or in combination with permethrin cream, followed by lindane or 6% to 10% sulfur ointment if necessary.
, and particularly under the fingernails and toenails, brushing the medication under the free edges of the nails. Ivermectin, 200 to 250 μg/kg of body weight may be appropriate, alone or in combination with permethrin cream, followed by lindane or 6% to 10% sulfur ointment if necessary.")
25
PEDICULOSIS

26
There are three types of lice known to infest humans; whether they are three or only two different species is controversial. The head and body lice may be variants within a single species, but are thought by most biologists to represent two distinct species.

27
The lice are tiny (1 to 4 mm) elongated, soft-bodied, wingless, dorsoventrally flattened, blood-sucking insects with six legs all terminating in small claws, which enable them to grasp hair shafts or clothing fibers. The third species, Pthirus pubis, is morphologically distinct from the others. The common term “crab louse” is an excellent description, the body being somewhat rounded like that of a crab, with small claws on the front pairs of legs and larger claws on the two rear pairs, which allow the louse to grip the widely spaced hairs of the pubic area, eyebrows and lashes, and other areas of short hairs.

28
Both head lice and pubic lice feed and reproduce on the human host, cementing their nits to the hair. Body lice, however, take their blood meals from the human host, but reproduce by attaching their eggs to the fibers of clothing. This has significance when treatment is considered. After an incubation period of 9 to 12 days, the nymphal stage emerges from the egg, or nit, and matures into an adult within another 10–15 days. Head and body lice may move as rapidly as 23 cm/min; the slower crab lice may travel only up to 10 cm/day.

29
Pediculosis Capitis (Head Lice)
ETIOLOGY AND EPIDEMIOLOGY Head lice are most common among children, infesting millions of elementary school students annually, spread by close physical contact as well as by the sharing of head gear, combs, brushes, and pillows. The lice are believed to survive for only about 24 to 48 h away from the human host, and therefore fumigation of homes is unnecessary.

30
Head lice affect all levels of society and all ethnic groups, although in the United States, the incidence is low among African Americans. Hair length is not an important factor. CLINICAL MANIFESTATIONS Pediculosis capitis is typically confined to the scalp . The most common symptom is itching, often intense, and the sight of schoolchildren scratching their heads often leads to the diagnosis. There may occasionally be a tiny hemorrhagic crust at the site to indicate the louse has taken its blood meal.

31
According to one study, bite reactions, pruritus, excoriations, lymphadenopathy, and conjunctivitis were the most common signs and symptoms, although lymphadenopathy was equally common in unaffected children of the same age.

32
DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS The most common diagnostic sign of head lice is the live nits on the proximal part of the hair shaft. These eggs are cemented to the hair by the female louse at the point where the hair exits the scalp. Thus the distance of the nit from the scalp along the hair shaft is evidence of the duration of the infestation. When all of the nits are noted to be a significant distance from the scalp (i.e., >1 cm) it is likely that the infection is no longer active and that these nits are not fertile. It is best to examine the hair under the microscope to assure that there are live larvae present within the nits and to exclude seborrheic scales, hair casts, and artifacts on the hair (e.g., hair spray) that may be brushed off easily.
 it is likely that the infection is no longer active and that these nits are not fertile. It is best to examine the hair under the microscope to assure that there are live larvae present within the nits and to exclude seborrheic scales, hair casts, and artifacts on the hair (e.g., hair spray) that may be brushed off easily..")
33
Pediculosis Corporis (Body Lice)
ETIOLOGY AND EPIDEMIOLOGY Pediculosis corporis is a disease of poverty, found almost exclusively among the indigent, the homeless, and groups living in crowded unsanitary conditions, such as refugees and, in wartime, the military—these patients are seen mainly in urban public hospitals. The body louse is about 30 percent larger than the head louse, but has essentially the same morphology. The infestation is usually transmitted by contaminated clothing or bedding.

34
CLINICAL MANIFESTATIONS AND DIAGNOSIS Occasionally, the macula cerulea (literally, sky-blue spot), a blue to slightly slate-colored macule, can be seen, particularly in areas where clothing binds, such as the waistband, and on the buttocks and thighs. It is an asymptomatic to slightly pruritic, somewhat bruiselike lesion, up to approximately 1.5 cm in diameter and often with a central punctum. More commonly, the only sign of body lice is excoriations, often linear and primarily on the trunk.

35
Postinflammatory pigmentation is seen in more chronic cases
Postinflammatory pigmentation is seen in more chronic cases. Adult lice are rarely seen except in heavy infestations. Diagnosis is made by closely examining the lining of the clothing, particularly at the seams, for the presence of nits. Body lice are medically important not because of the pruritus and secondary impetiginization, but because they may act as vectors for Rickettsia prowazekii and R. quintana (typhus and trench fevers. and Borrelia recurrentis (relapsing fever)
")
36
Pediculosis (Pthiriasis) Pubis (Pubic Lice)
ETIOLOGY AND EPIDEMIOLOGY Most often pubic lice are a sexually transmitted disease, commonly associated with other sexually transmitted diseases. There are no racial differences in incidence (unlike pediculosis capitis).
.")
37
CLINICAL MANIFESTATIONS As suggested by its name, this louse is most commonly found in the pubic hair, although in hirsute individuals the short hairs of the thighs, trunk, and perianal area may also be involved. All the hair-bearing skin should be examined. Occasionally, the beard, moustache, and even eyelashes may be involved. Infestation of the eyelashes and periphery of the scalp occur mainly in children, probably a result of contact with an infested parent.

38
Secondary infection because of excoriation may obscure the infestation and can lead to local lymphadenitis and fever. Maculae ceruleae (sky-blue macules) may be present as in pediculosis corporis and capitis . DIAGNOSIS The diagnosis is most frequently made by the patient him- or herself, often identifying the louse in the pubic area. Infested patients reportedly have an average of 10 to 25 or more adult organisms

41
Topical pediculicides 1
Topical pediculicides 1. pyrethrin products shampoo and others are available over-the-counter. They are applied to saturate the scalp and allowed to remain on for 10 min. The hair is then washed thoroughly, dried, and the nits can be removed with a fine-toothed comb which is often sold with the product. Permethrin, a synthetic pyrethrin, is marketed over the counter as Nix, a 1% cream rinse. After shampooing with regular shampoo, the hair and scalp are toweled dry and allowed to further air dry so as not to dilute the lotion. The hair and scalp are thoroughly saturated with the permethrin lotion, which is left in place for 10 min, rinsed thoroughly, and dried with a clean towel.

42
Malathion lotion 0.5% (Ovide; prescription only) appears to be the fastest-acting pediculicide, killing 100 percent of lice tested in less than 10 min. In the same study, malathion showed 100 percent ovicidal activity after a 10-min exposure. The FDA-approved directions recommend application to dry hair until the hair and scalp are thoroughly moistened, then allow it to dry and remain on the hair and scalp for 8 to 12 h, before washing out with nonmedicated shampoo.

43
Lindane (gamma-benzene hexachloride) 1% Enough shampoo is applied to dry hair to thoroughly wet the hair and scalp or skin of the affected and surrounding hairy areas. It is allowed to remain in place for 4 min, then, using just enough water to work up a good lather, it is rinsed out.

44
Ivermectin 200 μg/kg, two doses given 10 days apart
Ivermectin 200 μg/kg, two doses given 10 days apart. Although the reports to date are all anecdotal, ivermectin may emerge as the preferred treatment for the first half of the twenty-first century. There are also reports of the use of cotrimoxazole [trimethoprim-sulfamethoxazole (TMP-SMX)] for resistant head lice infestations, but it is premature to recommend the therapy at this time. Because neither ivermectin nor TMP-SMX is ovicidal, if used, they should be readministered in 7 to 10 days.
] for resistant head lice infestations, but it is premature to recommend the therapy at this time. Because neither ivermectin nor TMP-SMX is ovicidal, if used, they should be readministered in 7 to 10 days.")
45
PEDICULOSIS PUBIS Topical therapy is much the same as that for pediculosis capitis. The preparation should be applied to the infested area, paying particular attention to the pubic and perianal regions and adjacent hairy areas. A common cause of failure is treating only the pubic area in hairy individuals: the pediculicide should be applied to the thighs, trunk, and axillary regions because the mite can infest these areas as well.

46
PEDICULOSIS Corporis Because lice reproduce in the clothing and not on the skin, bathing, discarding or laundering infested clothing, and restoring proper hygiene should cure the infestation. Bedding should also be laundered with hot water, boiled, or discarded. Woolens and other nonwashables may be dry cleaned or ironed at home, with special attention given to the seams.

47
Complications Eczema, particularly in atopics, may be prominent both during the active infestation and after the scabies has cleared. Excoriation may lead to secondary pyoderma, and colonization with nephritogenic strains of streptococci may lead to acute glomerulonephritis. This complication is seen most commonly in tropical areas. Patients who have been successfully treated for scabies (or have never had scabies) may develop acarophobia or delusions of parasitosis .
 may develop acarophobia or delusions of parasitosis .")
Similar presentations