Download presentation
Presentation is loading. Please wait.

2
Toothbrushes, toothpastes, mouthwashes Dr Mahdi Kadkhodazadeh www.DrKadkhodazadeh.ir

3
"Forty years of experimental research, clinical trials, and demonstration projects in different geographical and social settings have confirmed that effective removal of dental plaque is essential to dental and periodontal health throughout life.“ 1998 European Workshop on Mechanical Plaque Control

4
نخستین مسواک مورداستفاده بشر : چوب درخت ارک اولین مسواک برس دار سال 500 میلادی در چین ساخته شد و در سال 1960 به دنیای غرب معرفی شد.

22
The dental profession relies on mechanical plaque control (i.e., daily cleaning with a toothbrush and other oral hygiene aids) as the most dependable way of achieving oral health benefits for all dental patients including periodontal patients.
 as the most dependable way of achieving oral health benefits for all dental patients including periodontal patients.")
23
Some toothbrush manufacturers claim superiority of design for such things as minor modifications of bristle placement, length, or stiffness. These claims are primarily based on demonstrations of plaque removal that are shown to be statistically significantly superior to comparable toothbrushes in one or more clinical studies.

25
The type of brush is largely a matter of individual preference. However, there is common agreement that use of a hard toothbrush, vigorous horizontal brushing, and possibly use of very abrasive dentifrice may lead to cervical abrasions of teeth and recession of gingiva.

26
In terms of recommending a particular toothbrush, superiority of clinical significance has not been demonstrated for any one type of toothbrush. Ease of manipulation by the patient is an important factor in brush selection, as is the patient's perception that the brush works well. The effectiveness of and potential injury from different types of brushes depend to a great degree on how the brushes are used.

27
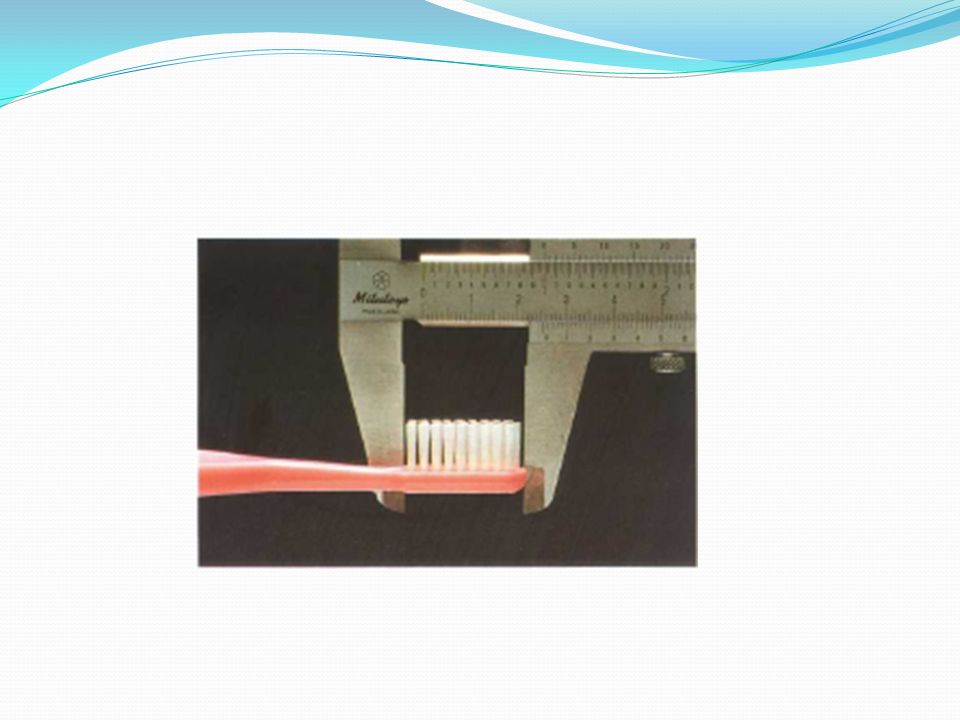
The American Dental Association has described the range of dimensions of acceptable brushes: a brushing surface 1 to 1.25 inches (25.4 to 31.8 mm) long and 5/16 to 3/8 inch (7.9 to 9.5 mm) wide, 2 to 4 rows of bristles, and 5 to 12 tufts per row.2 A toothbrush should be able to reach and efficiently clean most areas of the teeth.
 long and 5/16 to 3/8 inch (7.9 to 9.5 mm) wide, 2 to 4 rows of bristles, and 5 to 12 tufts per row.2 A toothbrush should be able to reach and efficiently clean most areas of the teeth.")
28
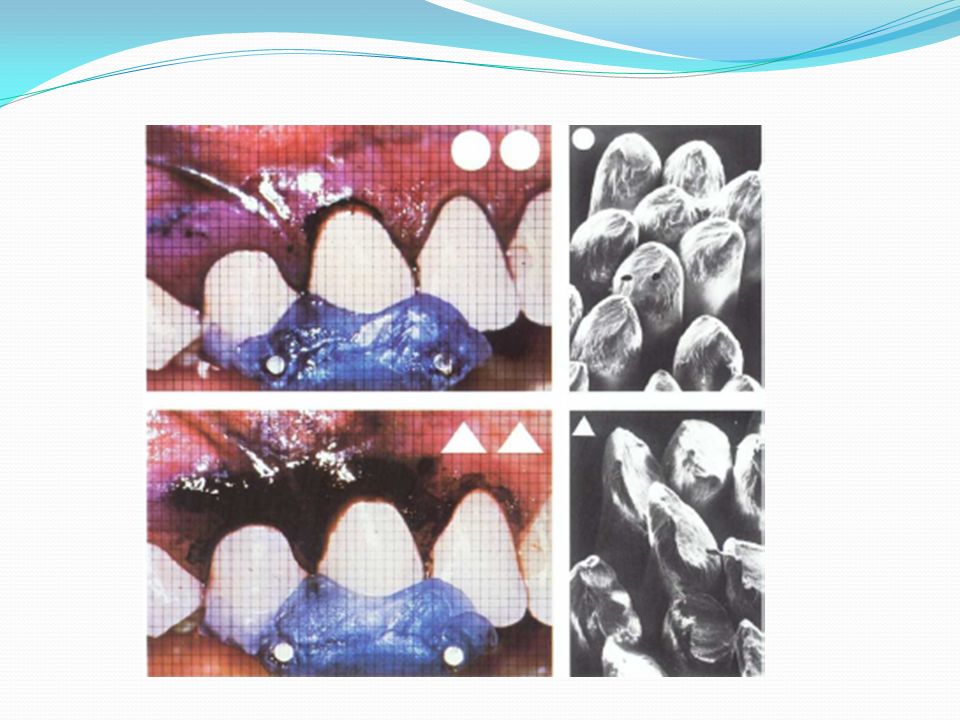
Toothbrush design (European workshop on mechanical plaque control 1998) A handle size appropriate to user age and dexterity A handle size appropriate to user age and dexterity A head size appropriate to the size of the patient’s mouth A head size appropriate to the size of the patient’s mouth End-rounded nylon or polyester filaments no larger than 0.225 mm in diameter End-rounded nylon or polyester filaments no larger than 0.225 mm in diameter Soft bristle configuration as defined by the acceptable international industry standards Soft bristle configuration as defined by the acceptable international industry standards Bristle patterns that enhance plaque removal in the approximal spaces and along the gum line Bristle patterns that enhance plaque removal in the approximal spaces and along the gum line
 A handle size appropriate to user age and dexterity A handle size appropriate to user age and dexterity A head size appropriate to the size of the patient’s mouth A head size appropriate to the size of the patient’s mouth End-rounded nylon or polyester filaments no larger than mm in diameter End-rounded nylon or polyester filaments no larger than mm in diameter Soft bristle configuration as defined by the acceptable international industry standards Soft bristle configuration as defined by the acceptable international industry standards Bristle patterns that enhance plaque removal in the approximal spaces and along the gum line Bristle patterns that enhance plaque removal in the approximal spaces and along the gum line")
30
Usually the smaller the better

31
Smallest heads(1.5cm):Infants Medium heads(2 cm):Young children Regular heads(2.5 cm):Adolescents
:Infants Medium heads(2 cm):Young children Regular heads(2.5 cm):Adolescents")
35
Infants’ brushes have large handles which facilitate manual dexterity

36
Bruun etal 1998: Toothbrush design has more effect on interproximal plaque than the brushing technique

37
Diameters of commonly used bristles range from 0.007 inch (0.2 mm) for soft brushes to 0.012 inch (0.3 mm) for medium brushes and 0.014 inch (0.4 mm) for hard brushes.
 for soft brushes to inch (0.3 mm) for medium brushes and inch (0.4 mm) for hard brushes.")
38
مطالعه تمیزی و حصاری 1374 مسواک کارون, مینا, مریم و خلال با باتلر, پروفشنال, جردن و فوکس مقایسه شد. خلال, کارون, مریم و پروفشنال در کاهش پلاک موثرتر شکل انتهای موهای مسواکهای مریم و خلال و فوکس و باتلر بهتر از بقیه فوکس نرمترین و خلال زبرترین معرفی شد.

39
مطالعه معین تقوی, صراف و آداوودی 1379 مسواک Oral – B و موژان مقایسه شد. هر دو در کاهش پلاک موثر بودند ولی موژان قیمت کمتر و مسواک Oral – B شکل مناسبتری داشت.

41
prevention through supragingival plaque control still remains the mainstay of controlling gingivitis and therefore the occurrence or re-occurrence of periodontitis

42
The importance of oral hygiene to outcome and long- term success of therapy for periodontal disease is hampered by the often ineffectiveness of mechanical cleaning to specific sites using a toothbrush and the limited or lack of use of interdental cleaning by many individuals

43
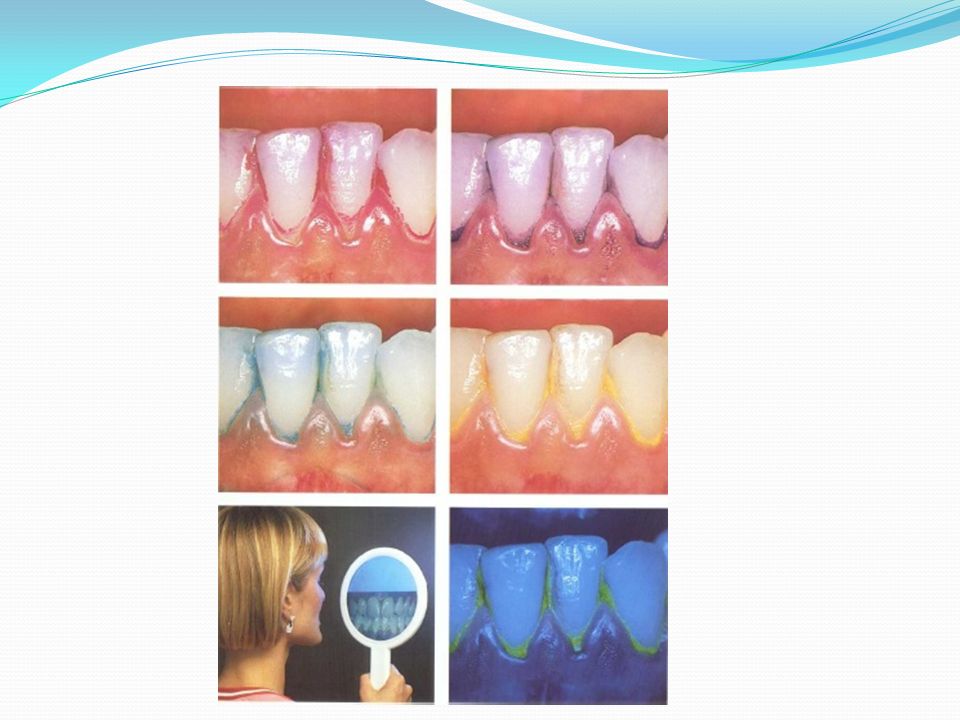
many individuals remove only around half of the plaque from their teeth even when brushing for 2 minutes (de la Rosa 1979). Presumably this occurs because certain tooth surfaces receive little or no attention during the brushing cycle (Rugg-Gunn & MacGregor 1978, MacGregor & Rugg-Gunn 1979).
..")
44
Taken with the microbial etiology of both gingivitis and periodontitis, this supports the concept of employing agents to control plaque which require minimal compliance and skill in their use. This is the concept that underlies chemical supragingival plaque control

45
The adjunctive use of chemicals would therefore appear a way of overcoming deficiencies in mechanical tooth cleaning habits as practiced by many individuals.

46
Ideal sites of action for chemicals which might influence plaque accumulation

47
At present most antiplaque agents are antimicrobial and prevent the bacterial proliferation phase of plaque development. Plaque formation could be controlled by antiadhesive or plaque removal agents, but these are not, as yet, available or safe for oral use. Alteration of bacterial plaque pathogenicity through chemical agents or bacterial modification would require a greater understanding of the bacterial etiology of gingivitis.

48
Many vehicles may be used to deliver antiplaque agents but most information relates to mouthrinses and toothpaste. Toothpaste appears the most practical and cost effective method for chemical plaque control for most individuals. In formulating antiplaque agents into toothpaste, potential inactivation by other ingredients must be considered. Minority groups, such as the handicapped, may benefit from other delivery systems.

49
Dentifrices Dentifrices are made up of abrasives such as silicon oxides, aluminum oxides, and granular polyvinyl chlorides; water; humectants; soap or detergent; flavoring and sweetening agents; therapeutic agents such as fluorides and pyrophosphates; and coloring agents and preservatives.

50
Chemical inhibitors of plaque and calculus incorporated in mouthwashes or dentifrices also play an important role in plaque control. Fluorides are essential for caries control. These products have been highly marketed and are commonly used as adjunctive agents to mechanical techniques.

51
Abrasives, commonly in the form of insoluble inorganic salts, make up 20% to 40% of a dentifrice. The proper use of a dentifrice can enhance the abrasive action of a toothbrush as much as 40 times. Tooth powders contain about 95% abrasives and are five times More abrasive than pastes. The abrasive quality of dentifrices affects enamel, but abrasion is more of a concern For patients with exposed roots because dentin is abraded 25 times faster and cementum 35 times faster enamel. This can lead to root surface abrasion and root sensitivity

52
Existing literature suggests that hard tissue damage from oral hygiene procedures is mainly due to abrasive dentifrices, whereas gingival lesions can be produced by the toothbrush alone

53
Abrasions are more prevalent on maxillary than on mandibular teeth and are found more frequently on the left than on the right half of the dental arch. This suggests that access and right- or left-handedness may also contribute to the abrasion.

54
Dentifrices that provide the effectiveness required for plaque control with a minimum of abrasion are preferable. There is considerable interest in improving dentifrices by using them as vehicles for chemotherapeutic agents to inhibit plaque, calculus, caries, or root hypersensitivity.

56
Abrasive :calcium carbonate, calcium pyrophosphate, aluminium silicate Anti bacterial agents: sodium lauryl sulphate, zink citrate trihydrate, triclosan, metal ions Anti caries agents: sodium monofluorophosphate,sodium fluoride,stannous fluoride Desensitizing agents: strotium salts, sodium flouride,formalin Filler and thickeners: sodium carboxymethyl cellulose Humectant:glycerine Detergent: sodium lauryl sulphate Flavoring agents: mint Coloring agent Sweetener: sodium saccharin

57
To achieve caries preventive effect, free fluoride ions must be available in the paste, not bound to the ingredients in the abrasive system. Correct amount of flouride=1000-1100 ppm.

58
Tartar control toothpastes with the active ingredient pyrophosphate This ingredient interferes with crystal formation in calculus and does not affect the fluoride ion in the paste or increase tooth sensitivity. This type of dentifrice has reduced the formation of new supragingival calculus by 30% or more

59
خمیردندانهای فلورایده : 25% NaF: crest-Improved crest NaF: crest-Improved crest NaMFP: Aim-colgate-Aqua fresh NaMFP: Aim-colgate-Aqua fresh signal-Macleans signal-Macleans SnF2: SnF2:

60
Mouth washes

61
Chlorhexidine Essential Oil Mouthrinse Cetylpyridinium chloride (quaternary ammonia compounds) Fluorides Oxygenating agents Povidone iodine Triclosan Delmopinol Sanguinarine Persica
 Fluorides Oxygenating agents Povidone iodine Triclosan Delmopinol Sanguinarine Persica")
62
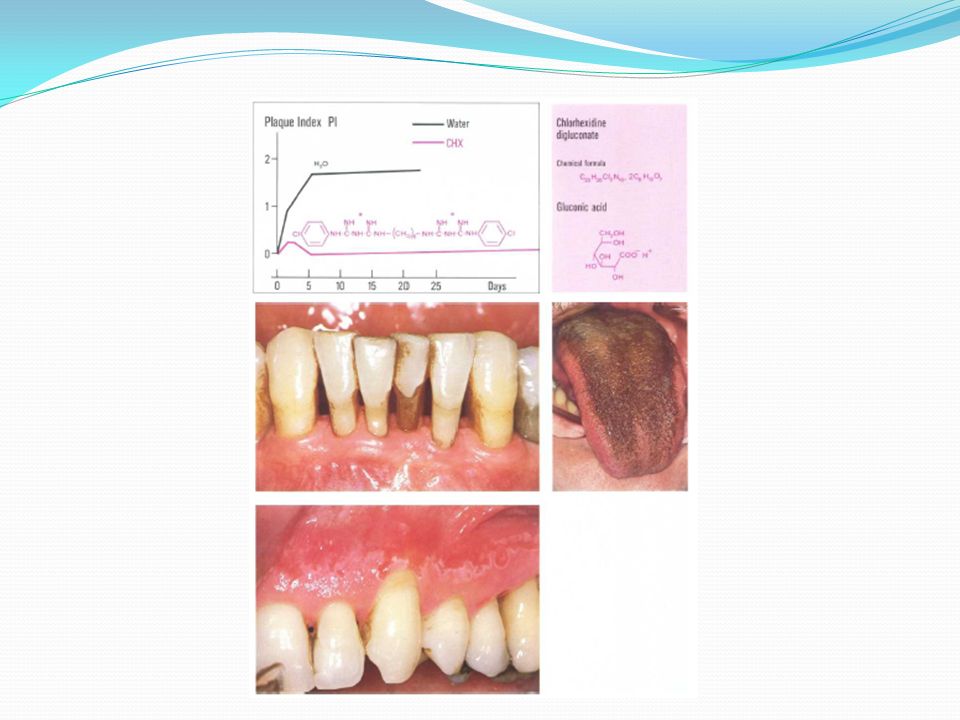
Chlorhexidine Synthetic Used since 1953 Increase in cellular membrane permeability followed by coagulation of the cytoplasmic macromolecules Is more effective in preventing plaque accumulation on a clean tooth surface than in reducing pre-existing plaque deposits Long substantivity High safety

63
Mouth rinse 0.2% Toothpaste 1% Sugar free chewing gum (containes 20 mg) Side effects: unpleasant taste, brown stain, mucosal erosion, parotid swelling
 Side effects: unpleasant taste, brown stain, mucosal erosion, parotid swelling")
64
Quaternary ammonium compounds Cetylpyridinium chloride Moderate inhibitory activity Greater initial oral retention and equivalent antimicrobial activity to chlorhexidine Less effective in inhibiting plaque and gingivitis Monocathionic

65
Phenolic antiseptic Listerine Essential oil/phenolic mouthwash Moderate plaque inhibitory effect and some anti- gingivitis effects (due to antioxidative activity) Poor oral retention
 Poor oral retention")
66
Povidone iodine No significant antiplaque activity(1% mouth wash) Absorption of significant levels of iodine Iodine sensitivity
 Absorption of significant levels of iodine Iodine sensitivity")
67
Triclosan Shina (Daroogar) mouthwash and toothpaste Non-ionic anticeptic Lacks of staining effects Moderate plaque inhibitory effects when used as a mouthwash in combination with zinc Anti inflammation effect due to inhibition of both cyclo- oxygenase and lipooxygenase Plaque inhibitory effects is dependent upon the presence of copolymers in formulation to increase the oral retention Anti inflammatory effect depends upon its ability to penetrate into the gingival tissues and in turn it is dependent upon the nature of the solvents in the mouthwash formulation
 mouthwash and toothpaste Non-ionic anticeptic Lacks of staining effects Moderate plaque inhibitory effects when used as a mouthwash in combination with zinc Anti inflammation effect due to inhibition of both cyclo- oxygenase and lipooxygenase Plaque inhibitory effects is dependent upon the presence of copolymers in formulation to increase the oral retention Anti inflammatory effect depends upon its ability to penetrate into the gingival tissues and in turn it is dependent upon the nature of the solvents in the mouthwash formulation")
68
Delmopinol Amine alcohol Inhibit plaque accumulation due to interference with plaque matrix formation and reduction of bacterial adherence It is suitable for a pre-brush mouth rinse

69
Metal ions Zinc,copper and tin Local side effect of staining(copper and tin) Stannous fluoride and amine fluoride Zinc is retained by dental plaque and inhibits its regrowth without disrupting the oral ecology
 Stannous fluoride and amine fluoride Zinc is retained by dental plaque and inhibits its regrowth without disrupting the oral ecology")
70
Carbamide peroxide Irsha: essential oil ( Ecalyptol) pre-brushing (containing fluoride) Oral-B: Naf Kimia :Naf Persica:salvadora persica, mint,yorrow Sinamol
 pre-brushing (containing fluoride) Oral-B: Naf Kimia :Naf Persica:salvadora persica, mint,yorrow Sinamol")
Similar presentations






















 ‘ Brushing Up on Mouth Care ’ Education.>")
 Click here to launch video Click here to download print activity.>")







 What’s so great about them?>")








