Download presentation
Presentation is loading. Please wait.

1
The Case for Rate Control: In the Management of Atrial Fibrillation Charles W. Clogston, M.D. Cardiologist CHI St. Vincent Heart Clinic Arkansas April 25, 2015

2
Atrial Fibrillation Atrial Fibrillation is the most common sustained arrhythmia Associated with increased mortality (1.5-1.9 by Framingham Study) Associated with increased morbidity (both in stroke and limiting symptoms)
 Associated with increased morbidity (both in stroke and limiting symptoms)")
3
Atrial Fibrillation Consequences Deterioration in hemodynamics (due to increased HR and loss of AV synchrony) Increased risk of stroke secondary to left atrial thrombi Progressive dysfunction of the left atrium and left ventricle
 Increased risk of stroke secondary to left atrial thrombi Progressive dysfunction of the left atrium and left ventricle")
4
Goals of Therapy in Atrial Fibrillation Symptom Control Improved by both rhythm and rate control Prevention of thromboembolism Achieved with anticoagulation with warfarin or newer novel anticoagulants

5
Management Strategies for Atrial Fibrillation Rhythm Control -- uses antiarrhythmic drug therapy, radiofrequency catheter ablation and/or surgical (Maze) ablation therapy at time of open heart surgery. Still requires rate slowing drugs. Rate Control – uses drugs that block or slow conduction thru the AV-node such as beta blockers, non-dihydropyridine calcium channel blockers or digoxin. AV-node ablation with ventricular pacing may be used when drugs are ineffective. Both therapies require anticoagulation to prevent thromboembolism.

6
Thromboembolic Risk with Atrial Fibrillation Thromboembolism is the most important adverse outcome. Maintaining NSR does not reduce the frequency despite cardioversion and antiarrhythmic drugs recurrence rate is 35- 60% at one year by intermittent monitoring and as much as 88% by continuous monitoring for more than 18 months.

7
Thromboembolic Risk with Atrial Fibrillation Up to 90% of recurrences are asymptomatic 17% of asymptomatic events last >48 hours In a study of pacemakers for arrhythmia detection in patients with no history of AF, AF duration of >5 min. increased risk of thrombo- embolism >6 fold compared with patients with similar CHADS2 scores and no AF.

8
Risk factor-based point-based scoring system - CHA2DS2-VASc Risk FactorScore Congestive Heart Failure/ LV Dysfunction1 Hypertension1 Age ≥ 75 years2 Diabetes Mellitus1 Stroke/ TIA/ Thrombo-embolism2 Vascular Disease*1 Age 65-741 Sex Category (i.e. female sex)1 Maximum Score9
1 Maximum Score9.")
9
Adjusted stroke rate according to CHA2DS2-VASc score

10
Approach to Anticoagulation in AF

11
Presumed Benefits of Maintaining NSR Fewer symptoms/better exercise tolerance Lower risk of stroke Long-term anticoagulation may not be needed if sinus rhythm is successfully maintained Better quality of life Better survival

12
Trials of Rate vs Rhythm Control

13
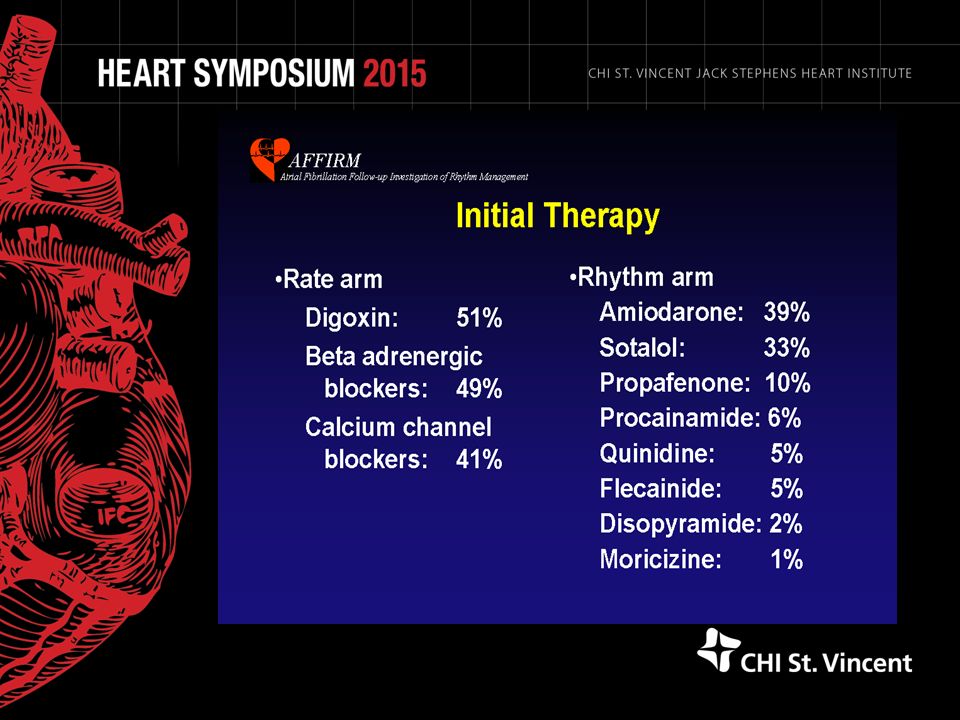
AFFIRM Baseline Characteristics Age = 69.7 ± 9 years 39% female >2 days of AF in 69% CHF class > II in 9% Symptomatic AF in 88%

14
Studies Comparing Rate and Rhythm Control AFFIRM Randomized 4060 patients with recurrent AF Goal for rate control of VR<80 bpm at rest and <110 bpm with 6 minute walk test Both received anticoagulation but rhythm control could remove if patient maintained NSR. (82 and 63% of patients at 1 and 5 years)
.")
17
AFFIRM Cross Over Rates Cross over to Rate Control arm occurred in 17 and 38% of patients in Rhythm Control arm at 1 and 5 years due to inability to maintain NSR or drug intolerance. Cross over to Rhythm Control arm occurred in 8 and 15% in Rate Control arm due to failure to control symptoms or CHF.

20
AFFIRM Findings At 3.5 years there was almost a significant decrease in all cause mortality (primary endpoint) in rate control arm There was no significant difference in the composite secondary endpoint of death, ischemic stroke, anoxic encephalopathy, major bleeding or cardiac arrest There was no significant difference in global functional status or quality of life in the initial report Number of patients requiring hospitalization was lower in the Rate Control arm (73 vs 80%)
 in rate control arm There was no significant difference in the composite secondary endpoint of death, ischemic stroke, anoxic encephalopathy, major bleeding or cardiac arrest There was no significant difference in global functional status or quality of life in the initial report Number of patients requiring hospitalization was lower in the Rate Control arm (73 vs 80%)")
21
RACE Trial Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation Study Similar to AFFIRM but Enrolled only patients with persistent atrial fibrillation who had been cardioverted at least once prior to enrollment and were in recurrent atrial fibrillation Primary end point was a composite of cardiovascular death, heart failure, thromboembolism, bleeding, pacemaker insertion, or severe side effects of antiarrhythmic drugs

22
Rate Control versus Electrical Cardioversion for Persistent Atrial Fibrillation (RACE) Trial (n=522)
 Trial (n=522)")
24
AF-CHF Results No difference in primary endpoint of CV death between groups (Figure) Cardioversion 39% vs 8% Also no difference in total mortality (31.8% vs. 32.9%, p = 0.73), stroke (2.6% vs. 3.6%, p = 0.32), worsening heart failure (27.6% vs. 30.8%, p = 0.17), or composite (42.7% vs. 45.8%, p = 0.20) Higher hospitalization rates (46% vs 39% p=.006) and cost with rhythm control Bradyarrhythmias ↑ in rhythm control group
, stroke (2.6% vs. 3.6%, p = 0.32), worsening heart failure (27.6% vs. 30.8%, p = 0.17), or composite (42.7% vs. 45.8%, p = 0.20) Higher hospitalization rates (46% vs 39% p=.006) and cost with rhythm control Bradyarrhythmias ↑ in rhythm control group.")
25
Cost Effectiveness of Rate Control over Rhythm Control AFFIRM Trial Cost Effectiveness Analysis Patients in the rate-control group used fewer resources, such as hospital days, cardioversions, and emergency department visits Estimated cost savings per patient treated with rate control ranged from $2189 to $5481 per person

26
Conclusions Ventricular rate control is equally (or more) effective than rhythm control in terms of survival, quality of life and other end points Current antiarrhythmics have a relatively low efficacy while having significant cardiac and non- cardiac side effects compared with rate control agents There are significant cost savings with rate control compared with rhythm control
 effective than rhythm control in terms of survival, quality of life and other end points Current antiarrhythmics have a relatively low efficacy while having significant cardiac and non- cardiac side effects compared with rate control agents There are significant cost savings with rate control compared with rhythm control")
Similar presentations








 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")

>")











 Trial Presented at The American College of Cardiology Scientific Session 2006 Presented by Dr. Carlo.>")
