Download presentation
Presentation is loading. Please wait.

1
The Abscess NORTON UNIVERSITY SURGICAL SEMIOLOGY Ass Prof. SEANG Sophat

2
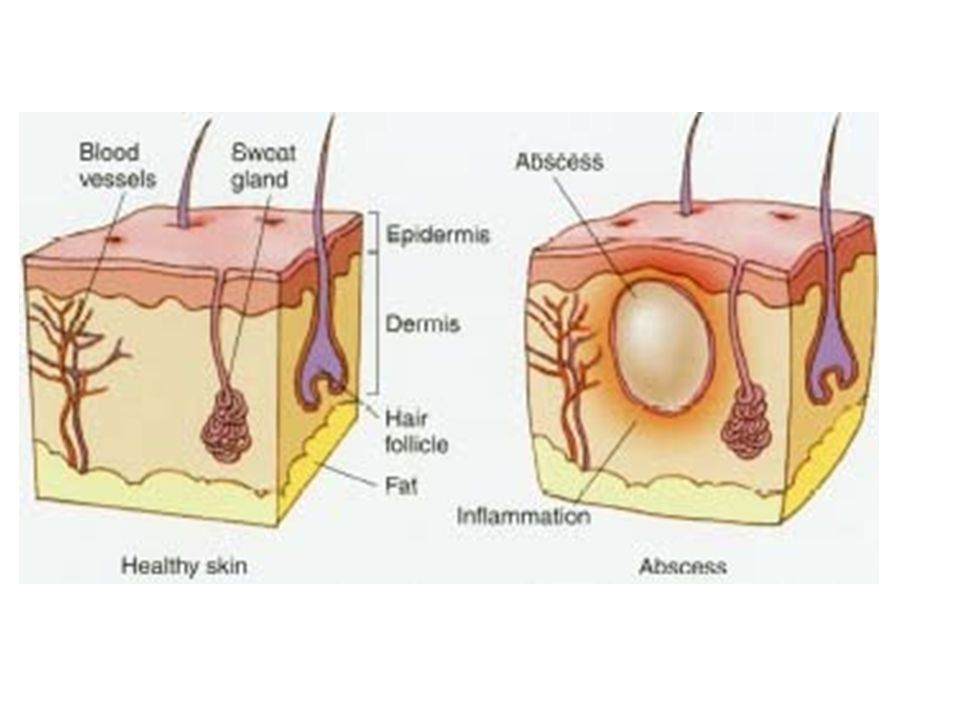
= collection of pus (= alterated polynuclear + necrotic tissue + bacteria and represent the difference with cellulitis) in a neoform cavity usually due to bacterial infection in tissues, organs and confined spaces. It can be also defined as a localized collection of pus in a cavity lined by granulation tissue. ex: skin abscess: Nb: here we are talking about warm abscesse

4
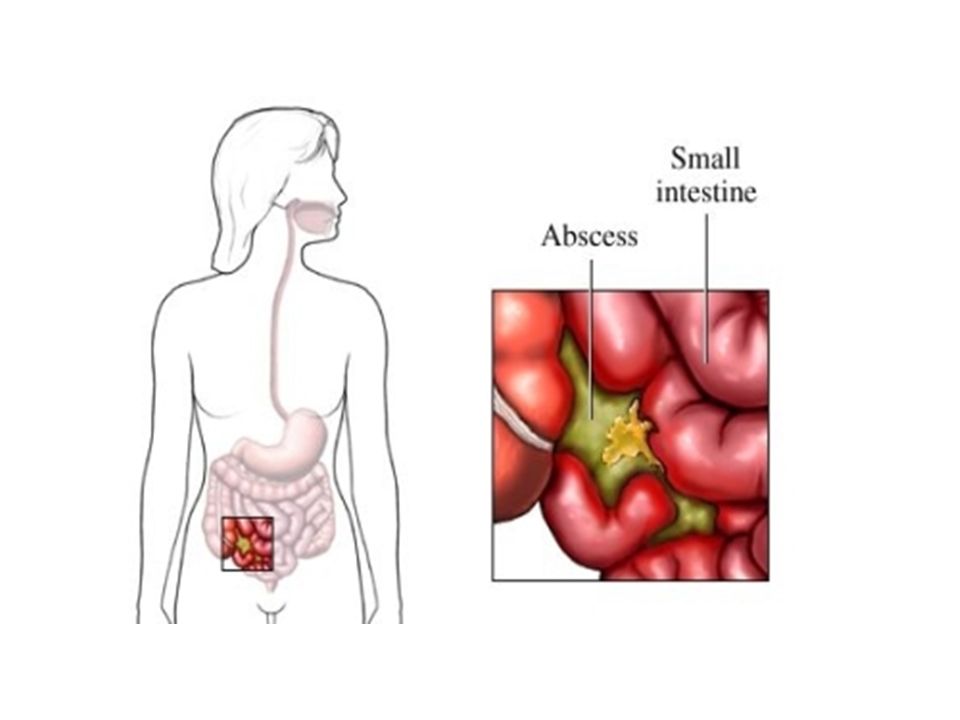
Pathogenesis Organisms causis abscess may enter the tissues by: Direct implantation: penetrating trauma with a non sterile object Spread from an established contigue infection Dissemination via lymphatic or hematogenous road from a distant site Migration from a location where they are resident into a adhesent normally sterile of natural barrier. Perforation of an abdominal tissue causing an intra- abdominal abscess:

6
Ethiology White staphylococcus and/or staphylococcus aureus or other organisms (streptococcus; pneumococcus; gonococcus; E.Coli; rare anaerobical microorganisms) Other causes: After introducing chemical irritating substances in the hypoderma (but it is not enough to create a abscess... it must be follow by a contact with a microorganism).
..")
7
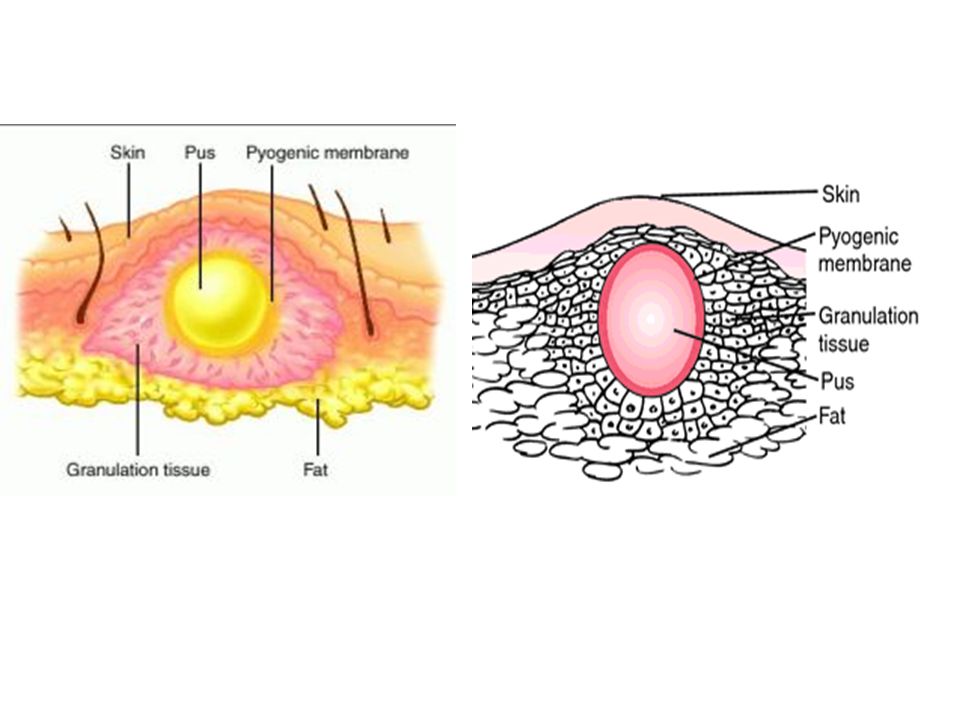
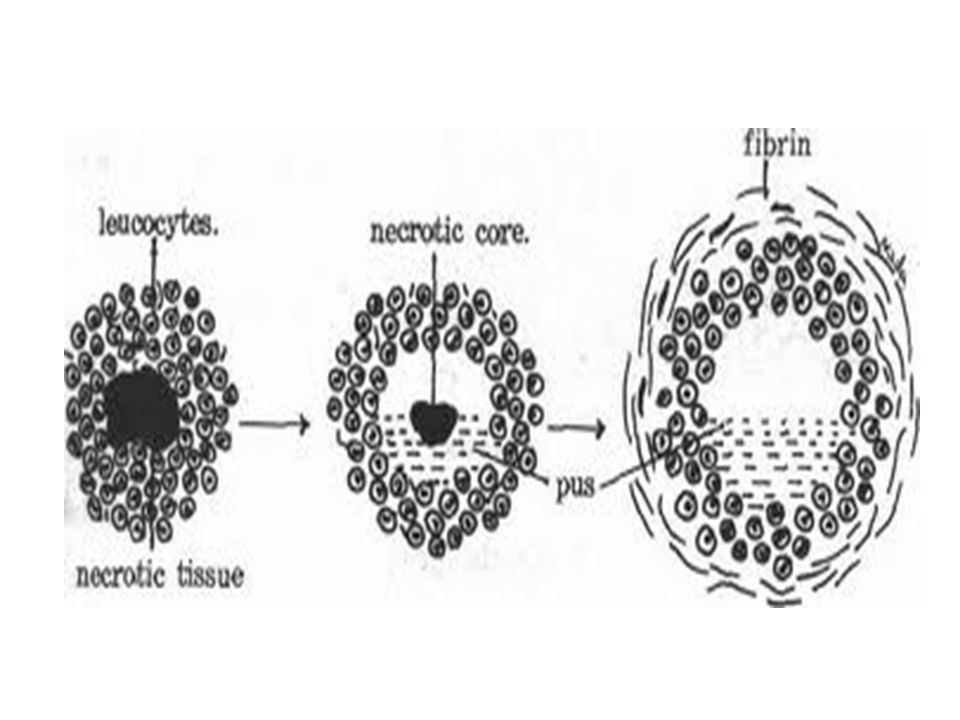
Structure of the abcess Infection leads to tissue necrosis and pus formation which is hyperosmolar, draws in fluid and the resulting increased intracavitary pressure causes throbbing pain. Pus has liquified necrotic tissue and dead and dying leukocytes that release damaging cytokinines, oxygen free and radicals and other molecules.

8
Structure of the abcess The cavity has an: Internal wall = it is the other name for the pyogenic membrane which the pus producing membrane or fibrinoleukocytar membrane (present the leukocyte + the fibrinous exudate). It separates normal tissue to pathological tissue> stop the propagation of the infection.

10
Structure of the abcess Middle wall = conjunctive tissue External wall= strong consistence conjunctive tissue = granulation tissue- macrophages, angiogenesis and fibroblast= sclerosis Contents of the cavity of the abcess is the pus

12
Aspect of the pus (it is very important because can orientate the diagnose): Yellow cream pus is generated by staphylococcus aureus Fluid aspect pus is generated by steptococcus Green aspect is generated by pneumococcus Grey and brown aspect is generated by anaerobical micro-organisms Yellow-green aspect and fetid smell (like putrefaction) is generated by E.Coli It is compulsory to remove the pus and realise a bacteriological exam + antibiogram
: Yellow cream pus is generated by staphylococcus aureus Fluid aspect pus is generated by steptococcus Green aspect is generated by pneumococcus Grey and brown aspect is generated by anaerobical micro-organisms Yellow-green aspect and fetid smell (like putrefaction) is generated by E.Coli It is compulsory to remove the pus and realise a bacteriological exam + antibiogram")
13
Clinical manifestation Local manifestation: Celsus signs: Tumor Calor Dolor Rubor Functio laesa

14
General manifestation: Fever Chills Cephalea Anorexia Insomnia Alteration of the general state

15
General manifestation: The abcess normally open itself with time (spontaneous rupture) and > disparition of the symptoms If it does not rupture spontaneously > infection of lymph vessel (> lymphangitis > lymphagadenitis)or blood vessel (> septicemia> death).
 and > disparition of the symptoms If it does not rupture spontaneously > infection of lymph vessel (> lymphangitis > lymphagadenitis)or blood vessel (> septicemia> death).")
16
Biological investigation: Leukocytosis Increased ESR

17
Complications Local: lymphangitis + lymphadenitis General: septicemia The evolution of the abcess occurs bet 2 days to 7 days

18
Treatment Only surgical treatment is recommanded = large incision + remove the pus + lavage by antiseptical solution (ie: H2O2 is compulsory for anaerobical bacteria> there is an effervescence which remove also necrotic tissue + we add betadine) + drainage („mèche „or tube)
 + drainage („mèche „or tube)")
19
Treatment The incision is done at the level of the apex of the cavity The „mèche” is very important because it allow to drain the secretions (without it a new abscess is generated) + to slow the speed of healing allowing regenerate the tissue properly. The dressing must be change + area clean with antiseptic + change the „mèche” every day the first week and 2 times by weak after

20
Treatment After the surgical operation (and only then) we use antibiotics + ice (to limitate the inflammation + infection) Nb: in case of phlegmon the delimitation is not as well obvious as in the abcsess
 we use antibiotics + ice (to limitate the inflammation + infection) Nb: in case of phlegmon the delimitation is not as well obvious as in the abcsess")
Similar presentations
 Closed wound: Skin is intact (not opened) include crushing injury and contusions. Wounds A) Skin involvement: 1) Open wound: when the whole thickness.>")


 –Swelling (tumor) –Warm (calor) –Tender (dolor) –Loss of function.>")









. >")
 is inflammation.>")




