Download presentation
Presentation is loading. Please wait.

1
e-learning, learning, and e
Dr. Stephen Bostock Advisor for Technology and Learning Keele University, UK

2
Summary E Learning Face to Face e-learning, an example
Online e-learning Blended learning, an example Conclusion

3
The e in e-learning Borrowed from e-commerce: electronic transactions between businesses and with customers E-learning: buying degrees online? Learning is far more complex than e-commerce – the wrong connotations (commercialization, commodification)
")
4
The learning in e-learning
eLearning is learning A cognitive-social-constructivist view Learning requires intellectual activity, engagement Students expect a personal transaction with a teacher Education is a personal service, not a commodity, not publishing “E-learning” – we’re stuck with it

5
Types of Teaching-Learning Activities and technology support
Pedagogy should drive the choice and use of technology – what supports the chosen learning activities? There are many classifications of activities necessary for learning! E.g. Laurillard’s 10; Shuell’s 12; Salmon’s 32 e-tivities; Biggs 16; etc. Level of detail, fine-grained or coarse Five will do here; they map to the others

6
Student modes of engagement in TLAs
Information transmission/reception teacher talk or writing about content, student listening, reading & note taking Multimedia transmission/reception listening, watching content, realism Individual activity doing, practising Interactivity in student groups discussing, proposing, defending, reflecting Student – teacher interactivity individual feedback to and from a teacher To sum up this first half, the traditional lecture traps students in a passive role that is unhelpful to learning. We can enhance the presentation, or get students to perform activities alone or in small groups, or interact with them as a group through technology, And we can combine any or all modes within one session.

7
The when and where

8
TLA type mode of engagement F2F TLA examples
Technology support example Online TLA examples Technology support examples 1 transmission /reception Didactic lecture Microphone Chalk? PowerPoint? Shovelware Set text Resource files 2 multimedia transmission /reception Images, video demonstration debate + projector and DVD, VCR, IAW Images, video, audio + multimedia files, streaming 3 Individual activity Answer, question, read, reflect handout, calculator, pen, Web, Google, Word, simulation 4 Student interactivity Discussion, PBL, collaboration Groupware? IAW Small group work CMC: , discussion board, chat 5 Student/ teacher interactivity Tutorial, interactive lecture Voting PRS Tutorial, Q&A + FAQs, tests, tutorial, voting integrated into Computer console, IAW Virtual Learning Environment

9
Information Transmission
With many students interaction is impossible, students cannot demonstrate knowledge, not get individual feedback, participation is voluntary. Listening and maybe writing are not good activities for learning. Tutors can be trapped into delivering content. One way information flow, and not even very efficient delivery. open loop. 4 things we can do about it: 4 strategies

10
Enhanced presentation
1. Enhance the presentation to make it memorable: add media or multimedia, demonstrations, video, realism (but not just PPT text slides)
")
11
Individual activity 2. Give student learning activities , individuals – problems, tasks,- But difficult to collect the results from may small groups.

12
Interactivity 3. Give student learning activities , individuals – problems, tasks,- or small groups even in lecture halls – discuss, compare, agree… But difficult to collect the results from may small groups.

13
Student-teacher interactivity
4. We can enable tutor-student interactivity so individuals can respond, but we need a technology, a mechanism.

14
How many modes of engagement are there in student groups?
1 Vote A 2 Vote B 3 Vote C 4 Vote D 5 Vote E 6 Vote F

15
Cheap, simple alternatives to electronic voting
A show of hands Any questions? Volunteers Random selection of students Coloured cards CommuniCubes

16
Being used in DH theatre 1
First year Psychology

17
Second year Law 2nd yr Law. With smaller groups no display is needed.

18
Response technologies
Electronic voting handsets anonymous but can opt out automatic counting and display electronic: high risk for teacher, training needed expensive Similar pedagogy CommuniCubes partially anonymous manual counting/ estimating low tech, low risk, no training cheap

19
Types of questions with a Personal Response System
“Concept check”: Multiple choice quiz on content just delivered Multiple choice quiz/problem solving at start to diagnose initial understanding Students self-report relevant experience Students self-report level of understanding Students opt for a revision topic Combine MCQ with activity, interactivity, and presentations. What could we do if we had such a system? Here are some ideas. We could give

20
Net advantage: modal answer was ‘a significant advantage’
Net advantage: modal answer was ‘a significant advantage’. Just one student thought they were worse than neutral.

21
Vote Vote for: Continue to the next topic
Say more about electronic Personal Response Systems Say more about CommuniCubes Say more about student evaluation of CommuniCubes

22
TLA type mode of engagement F2F TLA examples
Technology support examples Online TLA examples 1 transmission /reception Didactic lecture Microphone Chalk? PowerPoint? Shovelware Set text Resource files 2 multimedia transmission /reception Images, video demonstration debate + projector and DVD, VCR, IAW Images, video, audio + multimedia files, streaming 3 Individual activity Answer, question, read, reflect handout, calculator, pen, Web, Google, Word, simulation 4 Student interactivity Discussion, PBL, collaboration Groupware? IAW Small group work CMC: , discussion board, chat 5 Student/ teacher interactivity Tutorial, interactive lecture Voting PRS Tutorial, Q&A + FAQs, tests, tutorial, voting integrated into Computer console, IAW Virtual Learning Environment

23
Online learning Basic functions
Learning resources the Web, subject gateways, course web site, e-library, e-journals e.g. Keele Learning Server (modes 1, 2) Tools e.g. Google, Scholar, Word (mode 3) Discussion boards for asynchronous group text e.g. BSCW (modes 4,5) Computer Assisted Assessment testing and quizzing e.g. QuestionMark (mode 5)
 Tools e.g. Google, Scholar, Word (mode 3) Discussion boards for asynchronous group text e.g. BSCW (modes 4,5) Computer Assisted Assessment testing and quizzing e.g. QuestionMark (mode 5)")
24
Additional functions in Virtual Learning Environments
Easy organization of small groups within courses Student work submission, integration with plagiarism detection Activity tracking of cohorts and individuals Selective release of resources, tests, discussions etc. for individuals depending on activity Calendar, announcements, and other utilities Real-time chat: text, voting, shared whiteboard Many teacher administrative tools: Virtual Teaching Environments

25
Blended learning Adopted by HEFCE after their e-learning strategy consultation: normal practice! Our daily lives are a blend of F2F and online (cyberspace) activity; so should education be, for similar reasons What is the optimum (effective and efficient) mix of TLAs, traditional and technology-based? F2F and online? An example: engagement mode 4, blending traditional with electronic, F2F with online
 activity; so should education be, for similar reasons. What is the optimum (effective and efficient) mix of TLAs, traditional and technology-based F2F and online An example: engagement mode 4, blending traditional with electronic, F2F with online.")
26
TLA type mode of engagement F2F TLA examples
Technology support examples Online TLA examples 1 transmission /reception Didactic lecture Microphone Chalk? PowerPoint? Shovelware Set text Resource files 2 multimedia transmission /reception Images, video demonstration debate + projector and DVD, VCR, IAW Images, video, audio + multimedia files, streaming 3 Individual activity Answer, question, read, reflect handout, calculator, pen, Web, Google, Word, simulation 4 Student interactivity Discussion, PBL, collaboration Groupware? IAW Small group work CMC: , discussion board, chat 5 Student/ teacher interactivity Tutorial, interactive lecture Voting PRS Tutorial, Q&A + FAQs, tests, tutorial, voting integrated into Computer console, IAW Virtual Learning Environment

27
A 2004-5 example PBL in UG medicine
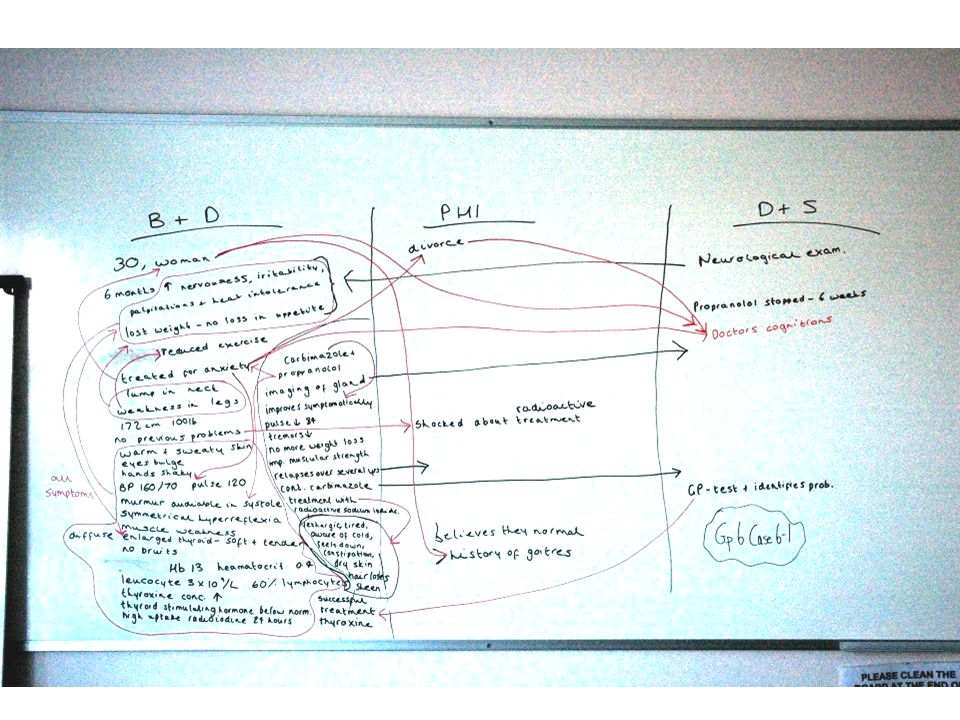
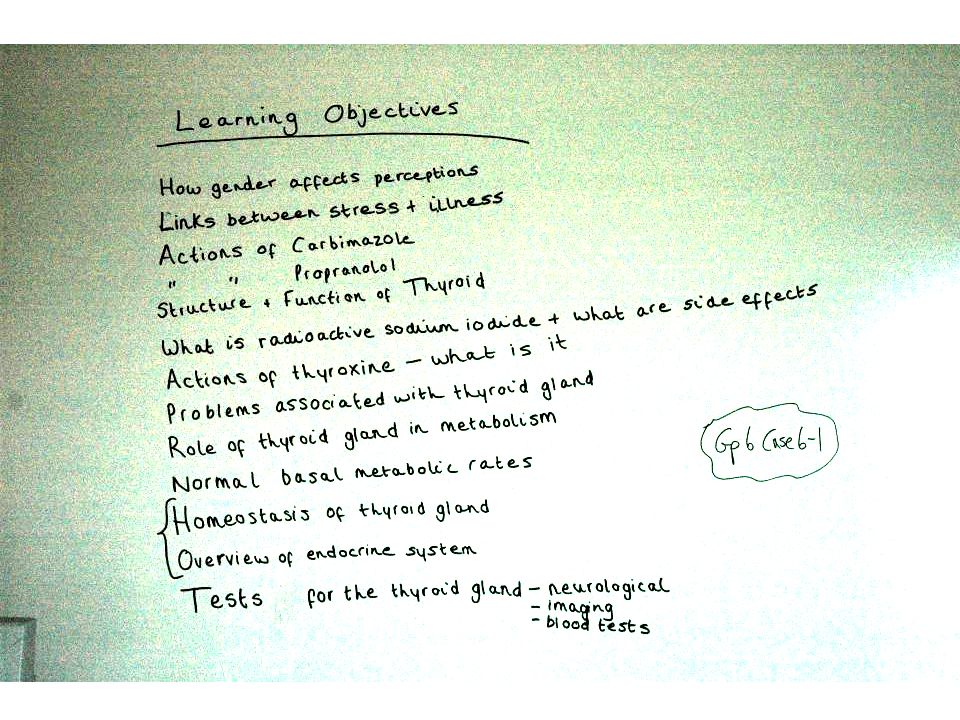
Groups of 8-12 students with a facilitator A rotating Chair and Scribe 3 one-hour meetings per case, per week Process: Definitions: words they don’t know Cues, of three types Links between cues, and their explanations Learning objectives: questions to answer All recorded on a whiteboard and then lost, unless on a flipchart

28
Traditional whiteboards from an example PBL case

36
Why introduce an “interactive whiteboard”?
All the work could be saved electronically A shared record to be printed or distributed to all group members Added to in later sessions

37
First semester plan Two year 1, two year 2 groups, four facilitators
Student scribe to use “flipchart” software by handwriting or typing Training sessions offered for hardware and software Tutors to convert flipchart files to Word or PowerPoint files and distribute by after each session Questionnaire at end of semester: features helpful and unhelpful to learning, and net worth to learning

40
First semester results 27% response
Many groups preferred typing to hand writing “Nice, neat, readable notes.” Liked file distribution “Allowed everyone in the group to have a copy of the same notes.” and re-editing “Access to previous notes quickly and accurately”

41
However, Many thought the software slow, it crashed too much, and handwriting was not readable Year 1 groups liked IAW at least as much as traditional technology, year 2 groups did not. On a scale of 0 (unhelpful) to 10 (helpful), net advantage:
 to 10 (helpful), net advantage:")
42
Second semester Watching the four PBL groups at work: what will save them time? PowerPoint 2003 instead of flipchart software Allows annotation No conversion to Office files needed Case texts prepared on slides, for highlighting and linking Notes stored on the Web instead of ing – web spaces with passwords for each PBL group Simpler process, fewer risks, less dependence on tutor

43
7 - Marta Marta (54) is a slim, well-dressed woman who is financially secure and has never needed to work. Her pride and joy are her three sons: the youngest has just graduated from university. Marta is a keen gardener. She and her husband have an active social life that includes ballroom dancing. Recently, she has found it difficult to keep up with him on the dance floor; she blames this on getting old. Suddenly, whilst digging the garden, Marta has an intense chest pain that quickly spreads to the left side of her jaw and her back. The pain goes away after she stops digging but it recurs the next month when she is again working in the garden and the weather is unusually cold. She goes to her GP who asks questions about chest pains during the previous year. All that Marta recalls is a few bouts of indigestion during the last 6 months. She admits to being a social smoker, but says she has decided to stop, insisting this will not be a problem because she has a lot of will power. Her father died from a heart attack in his 50s and her mother from a stroke in her 60s. Despite this family history, Marta is confident that her female hormones will protect her from heart disease. The GP measures her blood pressure and does a resting ECG (both are normal) and takes a venous blood sample for lipid analysis. He writes a prescription for glyceryl trinitrate (GTN) tablets (1 prn under the tongue), instructs Marta to start taking half an aspirin tablet a day and to return in 5 days. By then the hospital pathology service sends him the lipid data: serum cholesterol 6.8 mmol/L [desirable value <5.0]; low density lipoprotein (LDL) 5.2 mmol/L [desirable value <3.5]. On Marta’s next visit, she gets a prescription for simvastatin. For 2 years, until she is 56, Marta’s occasional chest pain is controlled by GTN. But, whilst clearing autumn leaves, she has a chest pain that is so bad and long lasting that her husband dials 999 for an ambulance. She arrives in A & E pale and clammy. Her pulse is a regular 60/min and her arterial pressures are 100/60 mmHg. The ECG has elevated ST segments and inverted T waves. A blood sample shows raised cardiac enzymes. Initial treatment includes oxygen by mask, and intravenous infusions of streptokinase, morphine sulphate and GTN. After 3 hours in A & E she is admitted to the coronary care unit (CCU). Her condition gives rise to concern because she is still complaining of chest pain. Emergency coronary angiography is undertaken and an immediate angioplasty is performed on her circumflex artery. The procedure is alarming and painful, but it stops the pain. She is sedated and closely monitored for several days – initially in coronary care and then on a medical ward. When she goes home on day 7, her drug treatment comprises atenolol, aspirin and simvastatin plus GTN when needed. Marta is invited to join the cardiac rehabilitation group at the hospital gym as the start of a comprehensive rehabilitation programme. Marta’s son shows her how to search the internet to find if such programmes work before she takes up the offer. But she turns it down saying “she had never been the sporty type” and “it would not suit her”. She is not keen to be “out of action” and intends to be back to normal soon.
 is a slim, well-dressed woman who is financially secure and has never needed to work. Her pride and joy are her three sons: the youngest has just graduated from university. Marta is a keen gardener. She and her husband have an active social life that includes ballroom dancing. Recently, she has found it difficult to keep up with him on the dance floor; she blames this on getting old. Suddenly, whilst digging the garden, Marta has an intense chest pain that quickly spreads to the left side of her jaw and her back. The pain goes away after she stops digging but it recurs the next month when she is again working in the garden and the weather is unusually cold. She goes to her GP who asks questions about chest pains during the previous year. All that Marta recalls is a few bouts of indigestion during the last 6 months. She admits to being a social smoker, but says she has decided to stop, insisting this will not be a problem because she has a lot of will power. Her father died from a heart attack in his 50s and her mother from a stroke in her 60s. Despite this family history, Marta is confident that her female hormones will protect her from heart disease. The GP measures her blood pressure and does a resting ECG (both are normal) and takes a venous blood sample for lipid analysis. He writes a prescription for glyceryl trinitrate (GTN) tablets (1 prn under the tongue), instructs Marta to start taking half an aspirin tablet a day and to return in 5 days. By then the hospital pathology service sends him the lipid data: serum cholesterol 6.8 mmol/L [desirable value <5.0]; low density lipoprotein (LDL) 5.2 mmol/L [desirable value <3.5]. On Marta’s next visit, she gets a prescription for simvastatin. For 2 years, until she is 56, Marta’s occasional chest pain is controlled by GTN. But, whilst clearing autumn leaves, she has a chest pain that is so bad and long lasting that her husband dials 999 for an ambulance. She arrives in A & E pale and clammy. Her pulse is a regular 60/min and her arterial pressures are 100/60 mmHg. The ECG has elevated ST segments and inverted T waves. A blood sample shows raised cardiac enzymes. Initial treatment includes oxygen by mask, and intravenous infusions of streptokinase, morphine sulphate and GTN. After 3 hours in A & E she is admitted to the coronary care unit (CCU). Her condition gives rise to concern because she is still complaining of chest pain. Emergency coronary angiography is undertaken and an immediate angioplasty is performed on her circumflex artery. The procedure is alarming and painful, but it stops the pain. She is sedated and closely monitored for several days – initially in coronary care and then on a medical ward. When she goes home on day 7, her drug treatment comprises atenolol, aspirin and simvastatin plus GTN when needed. Marta is invited to join the cardiac rehabilitation group at the hospital gym as the start of a comprehensive rehabilitation programme. Marta’s son shows her how to search the internet to find if such programmes work before she takes up the offer. But she turns it down saying she had never been the sporty type and it would not suit her . She is not keen to be out of action and intends to be back to normal soon.")
44
7 - Marta Marta (54) is a slim, well-dressed woman who is financially secure and has never needed to work. Her pride and joy are her three sons: the youngest has just graduated from university. Marta is a keen gardener. She and her husband have an active social life that includes ballroom dancing. Recently, she has found it difficult to keep up with him on the dance floor; she blames this on getting old. Suddenly, whilst digging the garden, Marta has an intense chest pain that quickly spreads to the left side of her jaw and her back. The pain goes away after she stops digging but it recurs the next month when she is again working in the garden and the weather is unusually cold. She goes to her GP who asks questions about chest pains during the previous year. All that Marta recalls is a few bouts of indigestion during the last 6 months. She admits to being a social smoker, but says she has decided to stop, insisting this will not be a problem because she has a lot of will power. Her father died from a heart attack in his 50s and her mother from a stroke in her 60s. Despite this family history, Marta is confident that her female hormones will protect her from heart disease. The GP measures her blood pressure and does a resting ECG (both are normal) and takes a venous blood sample for lipid analysis. He writes a prescription for glyceryl trinitrate (GTN) tablets (1 prn under the tongue), instructs Marta to start taking half an aspirin tablet a day and to return in 5 days. By then the hospital pathology service sends him the lipid data: serum cholesterol 6.8 mmol/L [desirable value <5.0]; low density lipoprotein (LDL) 5.2 mmol/L [desirable value <3.5]. On Marta’s next visit, she gets a prescription for simvastatin. For 2 years, until she is 56, Marta’s occasional chest pain is controlled by GTN. But, whilst clearing autumn leaves, she has a chest pain that is so bad and long lasting that her husband dials 999 for an ambulance. She arrives in A & E pale and clammy. Her pulse is a regular 60/min and her arterial pressures are 100/60 mmHg. The ECG has elevated ST segments and inverted T waves. A blood sample shows raised cardiac enzymes. Initial treatment includes oxygen by mask, and intravenous infusions of streptokinase, morphine sulphate and GTN. After 3 hours in A & E she is admitted to the coronary care unit (CCU). Her condition gives rise to concern because she is still complaining of chest pain. Emergency coronary angiography is undertaken and an immediate angioplasty is performed on her circumflex artery. The procedure is alarming and painful, but it stops the pain. She is sedated and closely monitored for several days – initially in coronary care and then on a medical ward. When she goes home on day 7, her drug treatment comprises atenolol, aspirin and simvastatin plus GTN when needed. Marta is invited to join the cardiac rehabilitation group at the hospital gym as the start of a comprehensive rehabilitation programme. Marta’s son shows her how to search the internet to find if such programmes work before she takes up the offer. But she turns it down saying “she had never been the sporty type” and “it would not suit her”. She is not keen to be “out of action” and intends to be back to normal soon.
 is a slim, well-dressed woman who is financially secure and has never needed to work. Her pride and joy are her three sons: the youngest has just graduated from university. Marta is a keen gardener. She and her husband have an active social life that includes ballroom dancing. Recently, she has found it difficult to keep up with him on the dance floor; she blames this on getting old. Suddenly, whilst digging the garden, Marta has an intense chest pain that quickly spreads to the left side of her jaw and her back. The pain goes away after she stops digging but it recurs the next month when she is again working in the garden and the weather is unusually cold. She goes to her GP who asks questions about chest pains during the previous year. All that Marta recalls is a few bouts of indigestion during the last 6 months. She admits to being a social smoker, but says she has decided to stop, insisting this will not be a problem because she has a lot of will power. Her father died from a heart attack in his 50s and her mother from a stroke in her 60s. Despite this family history, Marta is confident that her female hormones will protect her from heart disease. The GP measures her blood pressure and does a resting ECG (both are normal) and takes a venous blood sample for lipid analysis. He writes a prescription for glyceryl trinitrate (GTN) tablets (1 prn under the tongue), instructs Marta to start taking half an aspirin tablet a day and to return in 5 days. By then the hospital pathology service sends him the lipid data: serum cholesterol 6.8 mmol/L [desirable value <5.0]; low density lipoprotein (LDL) 5.2 mmol/L [desirable value <3.5]. On Marta’s next visit, she gets a prescription for simvastatin. For 2 years, until she is 56, Marta’s occasional chest pain is controlled by GTN. But, whilst clearing autumn leaves, she has a chest pain that is so bad and long lasting that her husband dials 999 for an ambulance. She arrives in A & E pale and clammy. Her pulse is a regular 60/min and her arterial pressures are 100/60 mmHg. The ECG has elevated ST segments and inverted T waves. A blood sample shows raised cardiac enzymes. Initial treatment includes oxygen by mask, and intravenous infusions of streptokinase, morphine sulphate and GTN. After 3 hours in A & E she is admitted to the coronary care unit (CCU). Her condition gives rise to concern because she is still complaining of chest pain. Emergency coronary angiography is undertaken and an immediate angioplasty is performed on her circumflex artery. The procedure is alarming and painful, but it stops the pain. She is sedated and closely monitored for several days – initially in coronary care and then on a medical ward. When she goes home on day 7, her drug treatment comprises atenolol, aspirin and simvastatin plus GTN when needed. Marta is invited to join the cardiac rehabilitation group at the hospital gym as the start of a comprehensive rehabilitation programme. Marta’s son shows her how to search the internet to find if such programmes work before she takes up the offer. But she turns it down saying she had never been the sporty type and it would not suit her . She is not keen to be out of action and intends to be back to normal soon.")
45
Prepared slide from case book
USEFUL CAL PACKAGES: • Coronary circulation • Cardiovascular tutorial • CVS histology • ECGs ON THE MANCHESTER WEBSITE: • Drugs and the heart • Psychology of heart disease Social and Behavioural Science Activities • Talk to some lay people about what they think causes coronary heart disease. Compare this with the published literature. • Investigate what cardiac rehabilitation programmes are available in Manchester and which kinds of health care professionals usually run them. • Identify the British Heart Foundation’s statement on evidence for efficacy of cardiac rehabilitation. Prepared slide from case book

46
Definitions Stroke – a sudden attack of weakness affecting one side of the body Aka - apoplexy Heart attack – death of a segment of the heart muscle due to interruption of its blood Supply Simvastatin – drug used to lower abnormally high amount of blood cholesterol PRN – pro re nata: as required Streptokinase – enzyme produced by certain strains of streptococcus that can liquefy blood clots Angiography- radiographic technique where radio opaque contrasts material is injected into the blood vessel Atenolol – oral beta blocker Angioplasty – method of treating a narrowing or blocake of blood vessel, inflating a balloon inside the vessel to open narrowing

47
Objectives Coronary arteries, cardiac pacemakers and conducting system, autonomic innervation of the heart, hormonal affect on heart – anatomy and physiology Atheroma Angina Ischemia, anoxia and infarction Drugs – streptokinase, atenolol, simvastatin, GTN, Aspirin and effects of cardio tonic drugs Angiography & angioplasty Serum cholesterol & LDL ECG and the changes with a myocardial infarction and ischemia Cardiac rehabilitation Personality type Risk factors for cardiac disease (Framingham )
")
48
Objectives Coronary arteries Left and right coronary arteries are first branches of the ascending aorta Come off just after the aortic valve Left coronary artery divides into circumflex artery and anterior interventricular artery Coronary veins – they drain into the coronary sinus (posterior side of the heart) in between the ventricle and atria. Coronary sinus drain into the right atrium next to vena cave Conducting system Sino atrial node situated in the wall of the right atrium (group of pace maker cells) Wave of depolarization moves to the AV node located in the right atrium The sa node is the group of cells that has the fastest rate of pace making ability. There are other cells in the heart with this ability but their not as fast Hearts myogenic
 in between the ventricle and atria. Coronary sinus drain into the right atrium next to vena cave. Conducting system. Sino atrial node situated in the wall of the right atrium (group of pace maker cells) Wave of depolarization moves to the AV node located in the right atrium. The sa node is the group of cells that has the fastest rate of pace making ability. There are other cells in the heart with this ability but their not as fast. Hearts myogenic.")
49
2) Atheroma Atherosclerosis – thickening of arteries as well as a loss of elasticity mainly affecting medium and large size arteries. Atheroma – describes plaque Plaque – consists of fibrous scar tissue, cholesterol and cholesterol esters, fat and inflammatory cells. LDL – taken up by macrophages and oxidised to form foam cells – may or may not lead to fibrosis plaque (appearance of fatty streaks) – accumulate under the endothelium – more lipid collects fibrous plaque consists of smooth muscle cells and elastic fibres forms. Complicated plaque – small deposits of fibrous material and then calcification. Why plaque development in arteries compared to veins? Incorrect repair process lead to the development of plaque Pressure on the wall leads to collagen build up Difference in diameter of vessel veins wider therefore less prone Process of calcification? – objective
 – accumulate under the endothelium – more lipid collects fibrous plaque consists of smooth muscle cells and elastic fibres forms. Complicated plaque – small deposits of fibrous material and then calcification. Why plaque development in arteries compared to veins Incorrect repair process lead to the development of plaque. Pressure on the wall leads to collagen build up. Difference in diameter of vessel veins wider therefore less prone. Process of calcification – objective.")
50
Atheroma cont… 75% occlusion leads to ischemia developing and possible MI plaque – thrombus – embolus – distal arteries causing occlusion – ischemia embolus may also form directly from the plaque below 75% occlusion, vessels dilate to compensate for reduced blood flow Angina Definition: characterised by paroxysmal and usually recurrent attacks of sub-sternal chest discomfort caused by myocardial ischemia which does not cause necrosis Systolic stretch In MI - necrosis – leads to ventricular walls become thin – compression causes the thin walls to bulge – thereby reducing contracting ability (enlarged Heart) Types Chronic stable angina/ exercised induced Unstable angina/ crescendo angina (pain increases in frequency and duration)
 Types. Chronic stable angina/ exercised induced. Unstable angina/ crescendo angina (pain increases in frequency and duration)")
51
Angina Cont… Variant angina/prinzmetal Pain starts from sub- sternal region – left pectorals muscle – shoulder Afferent nerve fibre from heart and cutaneus cells join the spinal cord at the same segment – relaying message to the brain via a common pathway MI Affects two areas Sub-endocardial - Which is limited to the inner third of ventricle wall or Transmural (whole of the ventricle wall) most affects left as this where the greatest oxygen demand is present Risk factors Hyper tension Smoking
 most affects left as this where the greatest oxygen demand is present. Risk factors. Hyper tension. Smoking.")
52
Drugs Simvostatin – HMG CoA reductase inhibitor competitively inhibits the rate limiting step of cholesterol synthesis Inhibits the conversion of HMG CoA – mevalonate Result is Fall in cholesterol Cells can regulate cholesterol synthesis, can increase enzyme production that results in reduced cholesterol and therefore increased LDL receptors because the cells cant compensate for drop in cholesterol level. Atenelol Comp antagonises beta 1 adreno-receptors on cardiac cells Reducing heart rate , contraction blood pressure Hydrophilic leass absorbed from the gut Increased diastole period giving time for coronary arteries to fill up

53
ECG MI ST elevation Inverted T wave Abnormal Q waves Lack O2 – cells die – therefore no conduction through these cells and thereby no contraction of these cells - MI Monitor cardiac enzymes to determine death of cells Rehabilitation Just as effective as drugs Improvement of lifestyle – exercise, risk factor modification – stop smoking, reduce salt intake, psychological Personality type – A Use family and existing social activities to educate about exercise

54
Links Digging in garden - chest pain increased O2 requirement because of exercise–increased cardiac output required to supply tissues– heart muscle workload increases - (Exercise induced angina) Not a problem with lungs because Marta is not breathless Cold weather – chest pain Trying to maintain core temp – metabolic rate increased via symp system –vasodilatation of blood vessels – increased cardiac workload – chest pain Chest pain – left side of jaw arm and back Nerves share the common pathway from the spinal cord C4 –T4 and therefore the brain is unable to distinguish which area the pain is from Female hormones – protection from cardiac disease Oestrogen protects from cardiac disease but the number of females with cardiac disease increase after the age of menopause.
 Not a problem with lungs because Marta is not breathless. Cold weather – chest pain. Trying to maintain core temp – metabolic rate increased via symp system –vasodilatation of blood vessels – increased cardiac workload – chest pain. Chest pain – left side of jaw arm and back. Nerves share the common pathway from the spinal cord C4 –T4 and therefore the brain is unable to distinguish which area the pain is from. Female hormones – protection from cardiac disease. Oestrogen protects from cardiac disease but the number of females with cardiac disease increase after the age of menopause.")
55
Genetic link Familial raised cholesterol level – increased risk of cardiac disease Normal resting ECG – = angina - rules out other cardiac disease Elevated level of cholesterol and LDL – simvastatin given to prevent cholesterol synthesis GTN – Chest pain + normal ECG = possible blockage of blood vessels GTN vasodilator compensate for areas of blockage. Pale and clammy Chest pain -Stimulation of symp system – vasoconstriction (pale) – sweat glands increased production Reduced pulse rate and BP Due to reduced cardiac output – part of the cardiac muscle has necrosed Raised cardiac enzymes – ischemia - (damage to cardiac cells) Monitor over days as levels fluctuate
 – sweat glands increased production. Reduced pulse rate and BP. Due to reduced cardiac output – part of the cardiac muscle has necrosed. Raised cardiac enzymes – ischemia - (damage to cardiac cells) Monitor over days as levels fluctuate.")
57
Case 2 - Mohammed and Nusrat want a Baby Mohammed and Nusrat Ahmed have been unable to conceive and their GP referred them to St. Mary's Hospital. Mohammed is 36 years old and is an industrial safety officer. Nusrat is 26 years old and is a primary school teacher. They have been married for three years and trying to conceive for the last two. Nusrat had her first period at the age of 15. Her periods have always been very irregular, bleeding occurring for between 3 and 10 days every 5 to 8 weeks. At the age of 18 her GP prescribed the oral contraceptive pill in order to regulate her cycle. She had regular withdrawal bleeds and continued the pill until her final year at college when she stopped taking it because she read a magazine article reporting side effects with prolonged use. However, she did use oral contraception during the first year of her marriage. Nusrat has always been overweight and thinks she is currently 3 stones too heavy. She has also noticed an increasing, embarrassing growth of hair on her upper lip, chin and thighs. Her periods are very infrequent. There is no other relevant personal or family history. Mohammed is fit and healthy. He has never been in hospital and is not taking any drugs. His work does not expose him to any toxic chemicals. Mohammed and Nusrat both felt stressed by their infertility and this was causing strains in their married and sexual life. They found it difficult to discuss these issues with their GP; when they presented with the problem initially he dismissed their worries claiming they had not been trying for long enough and, later, he refused to refer them for in vitro fertilisation (IVF) because of its low success rate. They joined the local branch of “Issue”, where they were encouraged to insist on treatment for their infertility. However, they felt a little overwhelmed with the amount of information the organisation gave them. Subsequently, they were referred to the Department of Reproductive Medicine at St. Mary's Hospital. Result of Investigations at St. Mary’s Hospital Nusrat Height 1.62m, weight 84kg, BMI 32, BP 120/70, pulse 72 regular Increased hair on face, breasts, sternum, abdomen and thighs. Breasts normally developed. No masses. No secretion from nipples. Pelvis: external genitalia normal, no clitoromegaly. Vagina, uterus and cervix normal. Endocrine investigations (ELISA assays): luteinising hormone 28IU/l (normal range 2-14 IU/l), follicle stimulating hormone 5IU/l (normal range 2-15 IU/l) on day 3 of her cycle, prolactin 548mU/l (normal up to 425mU/l), testosterone 5.1 nmol/l (normal up to 3.2 nmol/l), androstenedione 14.4 nmol/l (normal range 2-12 nmol/l), sex hormone binding globulin 17 nmol/l (normal range nmol/l), free androgen index 18.2 (normal up to 7.5). Pelvic ultrasound: bilateral enlarged ovaries with multiple small cysts. Normal uterine cavity with patent fallopian tubes Hysterosalpingogram: available in DR resource area normal uterine cavity with patent fallopian tube. Mohammed Mohammed's semen will be analysed in the physiological practical. The size of his testes was normal and serum testosterone was in the normal range. Treatment Nusrat's initial treatment, involving stimulation of her ovaries, was unsuccessful. Consequently the couple were finally accepted into an IVF programme. The IVF was carried out by standard procedures. Eighteen days after replacement of the embryos (at the 4-cell stage), Nusrat had not menstruated and a urine pregnancy test was positive.
 because of its low success rate. They joined the local branch of Issue , where they were encouraged to insist on treatment for their infertility. However, they felt a little overwhelmed with the amount of information the organisation gave them. Subsequently, they were referred to the Department of Reproductive Medicine at St. Mary s Hospital. Result of Investigations at St. Mary’s Hospital Nusrat Height 1.62m, weight 84kg, BMI 32, BP 120/70, pulse 72 regular Increased hair on face, breasts, sternum, abdomen and thighs. Breasts normally developed. No masses. No secretion from nipples. Pelvis: external genitalia normal, no clitoromegaly. Vagina, uterus and cervix normal. Endocrine investigations (ELISA assays): luteinising hormone 28IU/l (normal range 2-14 IU/l), follicle stimulating hormone 5IU/l (normal range 2-15 IU/l) on day 3 of her cycle, prolactin 548mU/l (normal up to 425mU/l), testosterone 5.1 nmol/l (normal up to 3.2 nmol/l), androstenedione 14.4 nmol/l (normal range 2-12 nmol/l), sex hormone binding globulin 17 nmol/l (normal range nmol/l), free androgen index 18.2 (normal up to 7.5). Pelvic ultrasound: bilateral enlarged ovaries with multiple small cysts. Normal uterine cavity with patent fallopian tubes Hysterosalpingogram: available in DR resource area normal uterine cavity with patent fallopian tube. Mohammed Mohammed s semen will be analysed in the physiological practical. The size of his testes was normal and serum testosterone was in the normal range. Treatment Nusrat s initial treatment, involving stimulation of her ovaries, was unsuccessful. Consequently the couple were finally accepted into an IVF programme. The IVF was carried out by standard procedures. Eighteen days after replacement of the embryos (at the 4-cell stage), Nusrat had not menstruated and a urine pregnancy test was positive.")
58
IVF Stimulation of overies Urine preg tests Hormone tests? contraceptive pill – 3 types Over weight 84kg and BMI 32 Depression? Irregular periods High Testosterone Increased hair face chin breasts and sternum polycystic ovaries Enlarged ovaries Increased hormones The pill Irregular periods ? Embarrassed by her appearance so no sex not able to conceive Irregular periods decrease in sbh Increase free androgen Increase in LH Increase in androstenedione Triggered by increase in insulin over weight No conception Complex issue of weights relationship with fertility

59
WebResources Polycystic Ovarian Syndrome Association Infertility Network UK

60
Learning objectives Mechanisms of oral contraception and side effects Out line of female reproductive system and its development Causes of infertility (polycystic ovaries, delayed puberty, weight) male What is IVF what do they do? What is prolactin and the other hormones mentioned and what do they do? What is an ultra sound? Procedures for infertile couples? Biology of conception both natural and ivf? Efficiency of conception How does the pregnancy test work ?
 male. What is IVF what do they do What is prolactin and the other hormones mentioned and what do they do What is an ultra sound Procedures for infertile couples Biology of conception both natural and ivf Efficiency of conception. How does the pregnancy test work")
64
Polycystic ovaries

68
3 main oestrogens Oestradiol Oestone Oestriole Aromatase Oestrone Androstenedione Cholesterol progesterone Testosterone oestriole Oestradiol

71
Semester 2 evaluations “A lot better now using Powerpoint. Easy to read and quick to use Interactive whiteboard“ They found helpful: Helps group process, saves time, notes are more readable Remote access to a permanent copy Ease of use Continuity between sessions Web access during session

72
However, for some Sem 2 IAW yr2 gp6 IAW yr1 gp8 IAW yr 1 gp1 Median
Slows down the work, difficult to draw diagrams System crashed (more training?) One Year 2 group now also liked the IAW but now one Year 1 group did not! Big differences between groups or tutors Sem 2 IAW yr2 gp6 IAW yr1 gp8 IAW yr 1 gp1 Median 7.5 8 1
 One Year 2 group now also liked the IAW but now one Year 1 group did not! Big differences between groups or tutors. Sem 2. IAW yr2 gp6. IAW yr1 gp8. IAW yr 1 gp1. Median")
73
Next year … Initial student training in PowerPoint 2003 as part of IT skills, emphasizing Ink Annotations Put PowerPoint 2003 (with PCs, projectors) in all PBL rooms, for use with/without an IAW The PCs in all PBL rooms to load the web spaces without dependence on tutors Case texts ready in PowerPoint in web spaces Let PBL groups mix traditional whiteboards and flipcharts with PowerPoint-IAW-Web
 in all PBL rooms, for use with/without an IAW. The PCs in all PBL rooms to load the web spaces without dependence on tutors. Case texts ready in PowerPoint in web spaces. Let PBL groups mix traditional whiteboards and flipcharts with PowerPoint-IAW-Web.")
74
Some conclusions from the PBL example
Mixing traditional/technology + online/F2F group support in this way is not “out of the box” Not the intended use of any of the technology (Web, VLEs or IAWs) so unexpected problems (eg handwriting) and unexpected benefits (eg web access to images) Exploring the affordances of the technology blend Success factors: Helping student productivity Student view is different: creating a set of notes (product not PBL process) Minimum effort and risk (familiar software, robust technology) Informal plus formal evaluation Experimentation, discussion, reflection
 so unexpected problems (eg handwriting) and unexpected benefits (eg web access to images) Exploring the affordances of the technology blend. Success factors: Helping student productivity. Student view is different: creating a set of notes (product not PBL process) Minimum effort and risk (familiar software, robust technology) Informal plus formal evaluation. Experimentation, discussion, reflection.")
75
The e in e-Learning Exciting Exhausting Efficient Effective Enhancing
B C D E

76
The e in e-Learning Experiment - Evaluate

78
Personal Response Systems PRS
Infrared or radio handsets with unique codes in a set. Codes are detected and numbers fed to software to display/store results, maybe through PowerPoint. Can be anonymous or use non-anonymous class register Cost £ per handset Staff training needed Risk of technical failure?

79
CommuniCubes Coloured cards and triangles have been used for voting
Cubes refine the idea and give 5 number choices Best in a raked lecture hall with benching or seminar with tables Pedagogic practice similar to PRS; participation is enforced; mix with other modes Anonymous to different degrees Different uses in seminars Intellectual Property Rights: Stephen Bostock

80
Two ways of displaying the results of a vote
Two ways of displaying the results of a vote. A spreadsheet ready to display a pie chart, and a mechanical pie chart if you don’t have a projector.

81
CommuniCubes – an initial evaluation
Foam and printed cubes made in Keele university First semester used in groups of in Education, Computer Science and Law; and with 120 in a 2nd year Law lecture Second Semester used in 250 1st year Psychology students (10 returns) 31 students in 2nd and 3rd year in Law tutorials (100% return) Two questionnaires: on first use and after several sessions Now a report on the use of the cubes. Thanks to Julie and Mark.
 31 students in 2nd and 3rd year in Law tutorials (100% return) Two questionnaires: on first use and after several sessions. Now a report on the use of the cubes. Thanks to Julie and Mark.")
82
1st year Psychology after several sessions: reasons cubes are helpful
Score: high= most important 12. Gave me feedback on my understanding 12. It was fun, made lecture interesting 8. Participation, made me think, contribute, be involved, express an opinion 6. (Mention of) “interactive” The reasons for and against them varied with the groups. In the large lecture, these were the factors given. These reasons were postcoded from the free text answers, and weighted by whether they were given as the most, second, or third most important reason. So a high score indicates more students thought them more important. Getting feedback on their answers to multiple choice quizzes was uppermost, plus statements about being interesting and fun.
 interactive The reasons for and against them varied with the groups. In the large lecture, these were the factors given. These reasons were postcoded from the free text answers, and weighted by whether they were given as the most, second, or third most important reason. So a high score indicates more students thought them more important. Getting feedback on their answers to multiple choice quizzes was uppermost, plus statements about being interesting and fun.")
83
After several sessions : 1st year Psychology - reasons unhelpful
Score: high= most important 12: Get answer from seeing others’ votes 9: A distraction, irrelevant 7: Slowed things down, wastes time Reasons against their use in PSy was that they were not completely anonymous – they thought of it as a test and thought others were cheating.

84
After several sessions : 3rd year Law - reasons helpful
Score: high= most important 39: Participation, made me think, contribute, be involved, express an opinion 5: Preparation for sessions improved 4: Gave me feedback on my learning 3rd yr law was similar. A few students mentioned helping preparation for seminars.

85
After several sessions : 3rd year Law - reasons unhelpful
Score: high= most important 13: Can get the answer from seeing others’ vote 9: Wasted time 8: Had to make a decision too quickly or when undecided They also worried about others copying a response. Also, there is always a time overhead, which a few students mentioned.

86
Evaluation conclusion
Most students found them helpful to learning: modal value is “significant advantage” A few (able?) students may dislike them In first year lectures the main reasons were getting feedback on understanding and fun In second and third year seminars the reason was the enforced participation The learning gains will depend on appropriate use, of course In conclusion, after this initial experiment… If anyone wants to use the cubes or handsets next year, contact me, I need volunteers.
 students may dislike them. In first year lectures the main reasons were getting feedback on understanding and fun. In second and third year seminars the reason was the enforced participation. The learning gains will depend on appropriate use, of course. In conclusion, after this initial experiment… If anyone wants to use the cubes or handsets next year, contact me, I need volunteers.")
87
TLA type mode of engagement F2F TLA examples
Technology support examples Online TLA examples 1 transmission /reception Didactic lecture Microphone Chalk? PowerPoint? Shovelware Set text Resource files 2 multimedia transmission /reception Images, video demonstration debate + projector and DVD, VCR, IAW Images, video, audio + multimedia files, streaming 3 Individual activity Answer, question, read, reflect handout, calculator, pen, Web, Google, Word, simulation 4 Student interactivity Discussion, PBL, collaboration Groupware? IAW Small group work CMC: , discussion board, chat 5 Student/ teacher interactivity Tutorial, interactive lecture Voting PRS Tutorial, Q&A + FAQs, tests, tutorial, voting integrated into Computer console, IAW Virtual Learning Environment

Similar presentations

















>")


 Dr. Stephen Bostock Advisor for Technology and Learning.>")



, the PC has become the tool.>")










 Dr. Stephen Bostock Advisor.>")
