Download presentation
Presentation is loading. Please wait.

1
PHYSICAL DISABILITIES

2
Physical Disabilities May Be A Result Of...
Neuromuscular (Spina Bifida, Spinal Cord Injury) Orthopaedic (Amputations) Cardiovascular (Stroke) Pulmonary disorders (COPD, Cystic Fibrosis)
 Orthopaedic (Amputations) Cardiovascular (Stroke) Pulmonary disorders (COPD, Cystic Fibrosis)")
3
WE ARE GOING TO FOCUS ON....

4
Spina Bifida Dr. Amanda Faith Casey Department of Human Kinetics
St. Francis Xavier University

5
What is Spina Bifida? What? Congenital defect of spinal column involves failure of vertebrae to completely enclose the spinal cord or it’s coverings (meninges). When?: 4th- 6th week of pregnancy. Bifida: Latin word “cleft” or “split into two parts”. How many? 11,000 children born each year (CDC, 2010).
. When : 4th- 6th week of pregnancy. Bifida: Latin word cleft or split into two parts . How many 11,000 children born each year (CDC, 2010).")
6
Important Considerations…
Lack of fusion of the bone plates that form the spinal arch may affect any level of the vertebrae. Several vertebrae may be fused together (shorter back). Bony protrusion in the midline of the back. Leg, bladder and bowel difficulty possible (Shin, 2010)
. Bony protrusion in the midline of the back. Leg, bladder and bowel difficulty possible (Shin, 2010)")
7
Diagnosis Of Spina Bifida Prenatal Tests
1. Alpha-fetoprotein (AFP) Test Between 16 and 18 weeks Blood sample taken from mother High AFP reading linked to Spina Bifida 2. Ultrasounds Spinal defects visible. 3. Folic acid ↓ folic acid = ↑ risk of Spina Bifida - There are several ways to diagnosis but the three most common forms of diagnosing for spina bifida are:
 Test. Between 16 and 18 weeks. Blood sample taken from mother. High AFP reading linked to Spina Bifida. 2. Ultrasounds. Spinal defects visible. 3. Folic acid. ↓ folic acid = ↑ risk of Spina Bifida. - There are several ways to diagnosis but the three most common forms of diagnosing for spina bifida are:")
8
What are the Causes??? Exact cause = mystery.
Suspect multifactoral: Genetic, nutrition, environment. Chromosone abnormalities Low folic acid. Medication e.g. Valproate, lamotrigine. Maternal diabetes Obesity

9
Types of Spina Bifida Type 1: Spina Bifida Occulta
Type 2: Spina Bifida Meningocele Type 3: Spina Bifida Myelomeningocele

10
Occulta Mildest form. Affects any level of the spine.
Signs (Williamson, 1987) A tuft of hair Birthmarks Dimple mark on the occulta Mainly in the lower part of the back. Symptoms Back stiffness and pain Fat pat over the occulta Skin covers spinal deformity. Does NOT cause paralysis or muscle weakness Associated with adult back problems.
 A tuft of hair. Birthmarks. Dimple mark on the occulta. Mainly in the lower part of the back. Symptoms. Back stiffness and pain. Fat pat over the occulta. Skin covers spinal deformity. Does NOT cause paralysis or muscle weakness. Associated with adult back problems.")
11
Meningocele Meninges push through the hole in the vertebrae
When Sac (meningocele) NOT covered by skin surgery becomes urgent. Hydrocephalus may occur. May have few/no symptoms or Incomplete paralysis with urinary and bowel dysfunction. A fluid filled sac protruding from the spinal cord.
 NOT covered by skin surgery becomes urgent. Hydrocephalus may occur. May have few/no symptoms or. Incomplete paralysis with urinary and bowel dysfunction. A fluid filled sac protruding from the spinal cord.")
12
Myelomeningocele Most severe .
Differs from meningocele in that the spinal cord is also pushed through the hole in the vertebrae. Classified as defect of the neural tube. Death 10% of infants. Bowel/ bladder control problems. ADHD or other learning disabilities. Some paralysis (Tarby, 1991) Severity depends on where opening occurs on the back. The higher the position = More severe paralysis. 80-90% hydrocephalus (Shin, 2010).
 Severity depends on where opening occurs on the back. The higher the position = More severe paralysis % hydrocephalus (Shin, 2010).")
13
Hydrocephalus... Cerebral spinal fluid (CSF) does not flow properly and builds up in the ventricles of the brain causing pressure. Surgically relieved by shunting procedure. Shunts (tubes or catheters) sometimes become clogged and must be replaced. Symptoms of shunt problems: Headaches irritability Vomiting swelling Seizures Lethargy No activity restrictions except avoidance of trauma to the head. Only visible evidence of shunt is a small scar behind the ear.
 sometimes become clogged and must be replaced. Symptoms of shunt problems: Headaches -irritability. Vomiting -swelling. Seizures. Lethargy. No activity restrictions except avoidance of trauma to the head. Only visible evidence of shunt is a small scar behind the ear.")
14
Treatment: Pre Versus Post Natal Surgery????
Traditionally post natal surgery performed. Surgical repair of a spinal birth defect before birth may improve mobility and reduce risk of serious complications from MM. New research: Infants who received prenatal surgery less likely to need follow-up procedure to divert or shunt, fluid away from the brain. Prenatal surgery resulted in significant improvements to both mental and motor functions. Children in prenatal surgery twice as likely to be able to walk without orthotics or crutches (42%) as children who received postnatal surgery (21%). Prenatal surgery more likely to cause preterm labour. See Adzick et al., 2011
 as children who received postnatal surgery (21%). Prenatal surgery more likely to cause preterm labour. See Adzick et al.,")
15
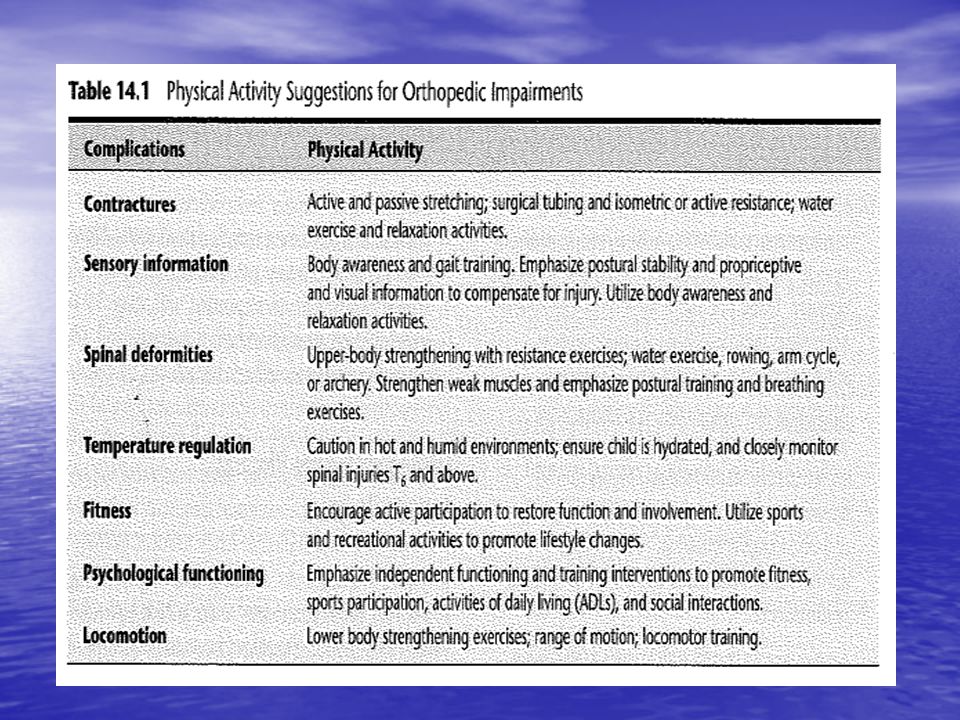
Planning Physical Activity
Initiate PA early to facilitate functional movement. Need to ascertain movement potential. Exercise should involve wide-range of activities (Horvat, 2007). Flexibility exercise – To delay contractures. Resistance exercise – To increase functional strength Aerobic training – To promote healthy lifestyle & aid weight management. Aquatics may offset weakness in lower extremities. HR elevated 20-45mins (ACSM, 2010). Teach gross motor skills to facilitate coordination. Triceps & shoulders important to train as aid in wheelchair transfers (O’Connell, 1992). Latex Allergy Possible weight gain added complication to reduced functional status (Dixon & Rekate, 1991). Complete fitness program = decreased obesity, stronger bones, better bowel function (Horvat, 2007)
. Flexibility exercise – To delay contractures. Resistance exercise – To increase functional strength. Aerobic training – To promote healthy lifestyle & aid weight management. Aquatics may offset weakness in lower extremities. HR elevated 20-45mins (ACSM, 2010). Teach gross motor skills to facilitate coordination. Triceps & shoulders important to train as aid in wheelchair transfers (O’Connell, 1992). Latex Allergy. Possible weight gain added complication to reduced functional status (Dixon & Rekate, 1991). Complete fitness program = decreased obesity, stronger bones, better bowel function (Horvat, 2007)")
17
Benefits of Physical Activity for Individuals w/ Spina Bifida
Researcher Participants Purpose Results Wright, C.M., Parker, L., Lamont, D., & Craft, W. (2001). 932 members of thousand families 1947 birth cohort. 412 attended for clinical examination. To determine whether being overweight in childhood increases adult obesity and risk of disease. BMI at age 9 was significantly correlated with BMI at age 50. Only children who were obese at 13 showed an increased risk of obesity as adults. Andrade,C-A., Kramer, J., Garber, M., & Longmuir, P. (1990). 16 children with SB born between 1976 and boys and 8 girls (10 community ambulators and 6 wheel chair users). Documented self-concept, cardiovascular endurance & isometric muscular strength of children with SB, and examine the changes during a 10 week exercise program. Improved self-concept, cardiovascular endurance, and isometric strength. An, J., & Goodwin, D.L. (2007). Seven mothers of children with SB. Each of their children used wheelchairs as a mode of transportation. This study was examining the role mothers play in inclusive physical education for students with SB, and what their perspectives were on it. Analysis revealed three main themes: a) a good thing but… b) connection to sports & c) beyond the curriculum. Mita et al. (1993) 35 chidren with spina bifida and 129 children without a disability were a control group. To determine the percentage body fat of children with SB, using underwater weighing and skinfold thickness to assess their obesity. The percentage body fat of children with hydrocephalus was significantly greater than children without hydrocephalus. Skinfold error was not substantial compared to underwater weighing (Nagamine & Suzuki method). Groff, D., Lawerence, E., & Grivna, S. (2006) 11-year-old male who had cerebral palsy, was deaf, and cortical visual impairment. To increase the boys physical activity to prevent physical regression of his physical abilities while responding to a medical treatment. The aerobic endurance, muscular strength and gross motor skills of the boy were slightly improved. Rimmer, J.H., Connor-Kuntz, F., Winnick, J.P., & Short, F.X. (1997) 32 children and adolescents with spina bifida.(11 have thoracic lesions and 21 have lumbar lesions). Seventeen females and 15 males from years old. To determine the feasibility of the TAMT in a group of children and adolescents with SB++. That TAMT was accurate for assessing moderate activity for people with spina bifida.
. 932 members of thousand families 1947 birth cohort. 412 attended for clinical examination. To determine whether being overweight in childhood increases adult obesity and risk of disease. BMI at age 9 was significantly correlated with BMI at age 50. Only children who were obese at 13 showed an increased risk of obesity as adults. Andrade,C-A., Kramer, J., Garber, M., & Longmuir, P. (1990). 16 children with SB born between 1976 and boys and 8 girls (10 community ambulators and 6 wheel chair users). Documented self-concept, cardiovascular endurance & isometric muscular strength of children with SB, and examine the changes during a 10 week exercise program. Improved self-concept, cardiovascular endurance, and isometric strength. An, J., & Goodwin, D.L. (2007). Seven mothers of children with SB. Each of their children used wheelchairs as a mode of transportation. This study was examining the role mothers play in inclusive physical education for students with SB, and what their perspectives were on it. Analysis revealed three main themes: a) a good thing but… b) connection to sports & c) beyond the curriculum. Mita et al. (1993) 35 chidren with spina bifida and 129 children without a disability were a control group. To determine the percentage body fat of children with SB, using underwater weighing and skinfold thickness to assess their obesity. The percentage body fat of children with hydrocephalus was significantly greater than children without hydrocephalus. Skinfold error was not substantial compared to underwater weighing (Nagamine & Suzuki method). Groff, D., Lawerence, E., & Grivna, S. (2006) 11-year-old male who had cerebral palsy, was deaf, and cortical visual impairment. To increase the boys physical activity to prevent physical regression of his physical abilities while responding to a medical treatment. The aerobic endurance, muscular strength and gross motor skills of the boy were slightly improved. Rimmer, J.H., Connor-Kuntz, F., Winnick, J.P., & Short, F.X. (1997) 32 children and adolescents with spina bifida.(11 have thoracic lesions and 21 have lumbar lesions). Seventeen females and 15 males from years old. To determine the feasibility of the TAMT in a group of children and adolescents with SB++. That TAMT was accurate for assessing moderate activity for people with spina bifida.")
Similar presentations








 or myelomeningocele (MY-eh-lo-me-NING-oh-seel )>")




 Will Hinckle (Still only 1/3 of a Paramedic)>")





