Download presentation
Presentation is loading. Please wait.

1
Arthroscopy Of the Ankle Mr. T.D.Tennent FRCS(Orth)
")
2
Ankle Arthroscopy Anatomy Patient setup Portal placement Procedures
Complications

3
Anatomy

4
Portals Anterior Anteromedial Anterolateral Anterocentral Posterior
Posterolateral Posteromedial Transachilles Tendon

5
Portals Anterior Anteromedial medial to tibialis anterior
saphenous nerve and vein are medial

6
Portals Anterior Anterolateral lateral to peroneus tertius
between branches of superficial peroneal nerve (6.5cm prox to tib of fibula)
")
7
Portals Anterior Anterocentral
between tendons of extensor digitorum communis dorsalis pedis artery and deep branch of peroneal nerve lie between tendons of EDC and EHL

8
Portals Accessory Anterior Portals Accessory anteromedial
1cm inferior and anterior to anterior border of medial malleolus Accessory anterolateral 1cm anterior and at or below tip of lateral malleolus

9
Anterior Portals

10
Portals Posterior Posterolateral
adjacent to lateral edge of achilles tendon cm above tip of fibula sural nerve and small saphenous vein

11
Portals Posterior Posteromedial
medial to achilles tendon at the joint line posterior tibial artery and tibial nerve Tendons of FHL and FDL calcaneal nerve branches

12
Portals Posterior Transachilles Tendon
at same level as the posteromedial but through center of achilles tendon

13
Portals Accessory Posterior Portals Accessory Posterolateral
1-1.5 cm lateral to posterolateral portal, slightly higher sural nerve and small saphenous vein

14
Portals Accessory Portals Transmalleolar Transtalar

15
Posterior Portals

16
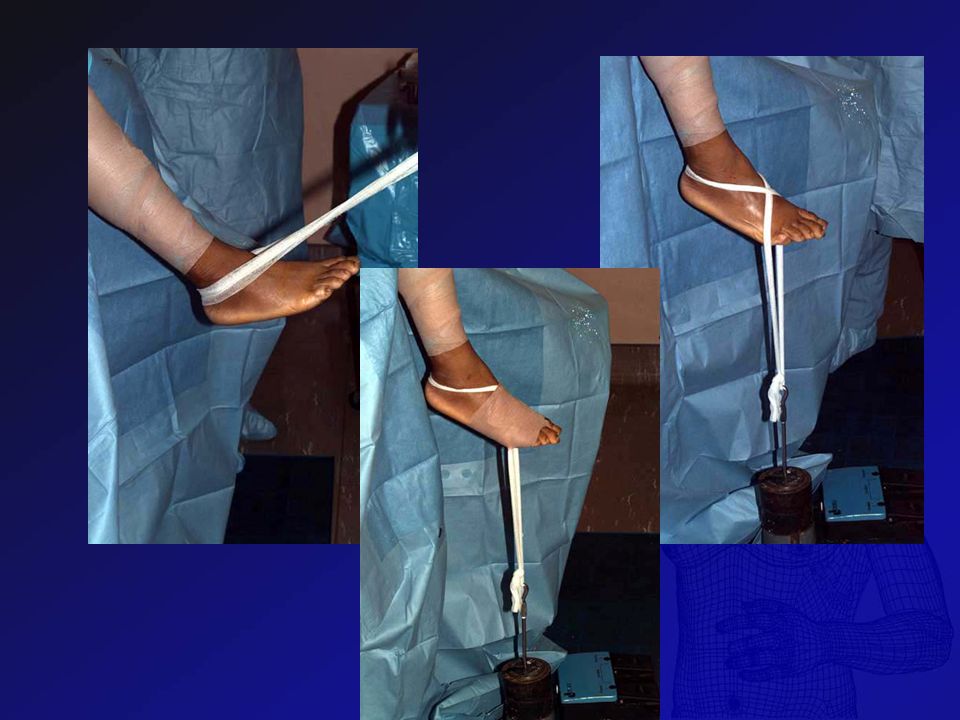
Patient Setup

19
Making Portals

25
Normal Ankle Examination
21 Point examination (Ferkel) 8 anterior (anteromedial portal) 6 central (anteromedial portal) 7 posterior (posterolateral portal)
 8 anterior (anteromedial portal) 6 central (anteromedial portal) 7 posterior (posterolateral portal)")
26
Normal Ankle Examination
Anterior 1: Deep portion deltoid ligament 2: Medial gutter 3: Medial talar dome 4: Medial talus articulation with plafond sagittal groove

27
Normal Ankle Examination
5: Lateral talus 6: Talofibular articulation “trifurcation” distal lateral tibial plafond lateral talar dome fibula 7: Lateral gutter 8: Anterior gutter

28
Anterior Examination

29
Normal Ankle Examination
Central 9: Medial dome of talus & corresponding plafond 10: Central portion of talus & plafond 11: Articulation lateral talar dome with tibia & fibula

30
Normal Ankle Examination
Posterior 12: Posterior inferior tibiofibular ligament 13: Transverse tibiofibular ligament 14: Capsular reflection of FHL

31
Central Examination

32
Normal Ankle Examination
Posterior (from posterolateral portal) 15: Deltoid ligament, posteromedial gutter 16: Posterior medial talar dome, tibial plafond 17: Central talus and distal tibia 18: Lateral talar dome, posterior tibia
 15: Deltoid ligament, posteromedial gutter. 16: Posterior medial talar dome, tibial plafond. 17: Central talus and distal tibia. 18: Lateral talar dome, posterior tibia.")
33
Normal Ankle Examination
19: Posterior talofibular articulation 20: Lateral gutter 21: Posterior gutter

34
Posterior Examination

35
Procedures Arthrodesis Osteochondral Defects Instability
Post Sprain Pain Anterior Impingement Meniscoid Lesions

36
Arthrodesis

37
Arthrodesis Zvijac (Arthroscopy Jan 2002) 21 patients Mean age 52.7
Av. FU 34 months 20/21 fusion Av. time to union 8.9 weeks

38
Arthrodesis 9 excellent: no pain, limp, or occupational restriction
11 good: mild pain, occasional limp 1 poor: failed union and pain extensive AVN approximately 50% talus

39
Arthrodesis Advantages: high fusion rate decreased time to fusion
decreased cost No or mild angular deformity No AVN greater than 30% of the talus.

40
Arthrodesis Cameron (Arthroscopy Feb 2000) 15 cases FU 1-3 years
100% fusion Average of 11.5 weeks

41
Arthrodesis 5 patients required further surgical treatment
2/5: infections 2 required hardware removal 1 screws symptomatic subcutaneously 1 screw penetrated the subtalar joint

42
Osteochondral Defects
Ogilvie-Harris (Arthroscopy Dec 1999) 33 patients duration of symptoms 2.3 years FU 7.4 years Osteocartilaginous fragment removed Defect debrided with a power shaver Base abraded
 33 patients. duration of symptoms 2.3 years. FU 7.4 years. Osteocartilaginous fragment removed. Defect debrided with a power shaver. Base abraded.")
43
OCD 79% were able to return to unrestricted sports
3% (1 pt) was unable to return to any sport Minor degenerative changes in 2 cases
 was unable to return to any sport. Minor degenerative changes in 2 cases.")
44
OCD Lahm (Arthroscopy April 2000) 42 patients
22 underwent percutaneous drilling 13 cancellous bone grafting 4 refixation 3 curettage

45
OCD 24 lateral talus all had trauma 11/18 lesions at the medial talus
no evidence of trauma

46
OCD K-wire drilling reached an average of 87 points
No significant difference in the lesions at the medial or lateral talus

47
Ankle instability Ogilvie-Harris (Arthroscopy Nov 1994) 19 patients
Clinical features of disruption of the syndesmotic ligaments Positive external rotation stress test

48
Ankle instability Common triad:
Disruption of the posterior inferior tibiofibular ligament Rupture of the interosseous ligament Chondral fracture of the posterolateral portion of the tibial plafond

49
Ankle instability Arthroscopic resection of the torn portion of the interosseous ligament and the chondral pathology Successfully relieved the symptoms in most of the patients

50
Post sprain pain Ogilvie-Harris (Arthroscopy Oct 1997) 100 patients
Failed to respond to conservative treatment for at least 6 months

51
Post sprain pain 3 groups: Instabilities (lateral and syndesmotic)
Impingements (anterior and anterolateral) Articular lesions (chondral and osteochondral).
 Articular lesions (chondral and osteochondral).")
52
Post sprain pain Significant improvements : Chondral fractures
syndesmotic instability anterior and anterolateral impingement Chondral fractures stable ankle : 75% good unstable ankles: 33% good

53
Post sprain pain Arthroscopy offered little to the management of lateral instability Minimal improvements for the patients with nonspecific diagnoses

54
Anterior Impingement Anterior ankle pain ? aetiology

57
Meniscoid Lesion Persistent pain in the anterior part of the upper ankle Portions of hyalinized tissue following an inversion sprain of the ankle Trapping of this formation between the lateral cheek of the talus and the fibula is supposed to be responsible for pain

58
Meniscoid lesion Lahm (Arthroscopy Sept 1998)
59 arthroscopic procedures Meniscoid lesions were seen in 19 cases Only 1 of these 19 patients showed lateral and anterior instability

59
Osteoarthritis Ogilvie-Harris (Arthroscopy Aug 1995) 27 patients
4 years symptoms FU 45 months 17/27 patients improved only 2 ankles were restored to normal function

60
Osteoarthritis Statistically significant improvement in Pain Swelling
Stiffness Limp Activity level Feeling of instability failed to reach significance

61
Outcomes Amendola (Arthroscopy Oct 1996) 79 arthroscopies
minimum 2-year follow-up

62
Outcomes 21 OCD 14 post-ankle fracture scarring
11osteoarthritis and chondromalacia 14 anterior bony impingement 15 anterolateral soft tissue impingement or synovitis

63
Outcomes 63 of 79 patients benefited in some way
Theraputic only: 36 of 44 (82%) of the patients benefited
 of the patients benefited.")
64
Outcomes Best results: Localized osteochondral lesion of the talus
Localized bony or soft tissue impingement Localized lateral plica

65
Outcomes Worse results: Osteoarthritis Posttraumatic chondromalacia
Arthrofibrosis

66
Outcomes 3 significant neurological complications
2 partial deep peroneal nerve neuropraxia 1 superficial peroneal nerve irritation

67
Complications RD Ferkel (Arthroscopy 1996) 612 patients
overall 9.0%, 27 neurological (4.4%) 15 superficial peroneal nerve 6 sural nerve 5 saphenous nerve 1 deep peroneal nerve
 15 superficial peroneal nerve. 6 sural nerve. 5 saphenous nerve. 1 deep peroneal nerve.")
68
Complications Mariani (Arthroscopy April 2001) pseudoaneurysm
 pseudoaneurysm")
69
Summary Useful technique Advantages over open surgery in some cases
Potential neurovascular complications Strict adherence to portal technique

70
Thank You

Similar presentations













 Radiographic Evaluation of the Ankle>")













