Download presentation
Presentation is loading. Please wait.

1
Oral and maxillofacial trauma in sports
Dr. A. Khayampour DDS, MS, OMFS

2
Objectives discuss scope of maxillofacial injuries in sports
discuss on-field assessment of maxillofacial injuries Review common maxillofacial injuries PREVENTION IS KEY

3
Scope of the problem Boys: 3-9 times more maxillofacial injuries
%50 of facial trauma occurs in mouth and teeth Low Speed elbows & fists soft tissue lacerations & contusions High Speed balls, pucks, sticks Bone / tooth fractures

4
Scope of the problem Face is the most vulnerable area of the body and is usually the least protected 11-40% of sports injuries are sports related Sports related facial injuries: 8% of all facial injuries Direct trauma from ball or player to player contact Health care providers for athletes should be familiar with facial anatomy, facial trauma from sports and initial management of facial injuries

5
Scope of the problem The most common injuries are occurred in facial soft tissue and T- zone(nose, zygoma and mandible) Some injuries can be managed in the field and some others need transfer to ER and specialist’s care

6
Scope of the problem Maclsaac et al: the most common age group in children are YO (40.7%) Baseball and softball: 44.3% of craniofacial fractures Basketball: 7.2%, Football: 3.0% Throwing, catching or hitting ball: 34.1% Collision between players: 24.5%

7
Scope of the problem Nasal Fx: 35.9%(50% in some literature)
Orbital:33.5% Skull: 30.5% Maxillary: 12.6% Mandible: 7.3% ZMC: 4.2% NOE: 1.2%

8
Scope of the problem Proper initial diagnose and management may prevent unfavorable results The main goal is to help athletes to recover functionally and aesthetically from facial trauma and to return to competition in a timely manner

9
Facial anatomy Facial blood supply is derived from contributions of both the external and internal carotid arteries: ischemic tissue flaps and infections are uncommon. The underlying facial muscles account for the tension lines and rhytides of the skin. These skin lines become more prominent with age and the loss of skin elasticity and should be observed during the repair of soft tissue injuries to avoid unnatural scarring.

10
The sensation of the face is supplied mainly by the 3 branches of the trigeminal nerve (ophthalmic [V1], maxillary [V2], mandibular [V3]). The muscles of mastication that control the opening and closing of the jaw are also innervated by the motor division of the trigeminal nerve. The muscles of facial expression are innervated by the 5 branches of the facial nerve (frontal, zygomatic, buccal, marginal mandibular, and cervical)
![The sensation of the face is supplied mainly by the 3 branches of the trigeminal nerve (ophthalmic [V1], maxillary [V2], mandibular [V3]).](http://slideplayer.com/slide/4271357/14/images/10/The+sensation+of+the+face+is+supplied+mainly+by+the+3+branches+of+the+trigeminal+nerve+%28ophthalmic+%5BV1%5D%2C+maxillary+%5BV2%5D%2C+mandibular+%5BV3%5D%29..jpg "The muscles of mastication that control the opening and closing of the jaw are also innervated by the motor division of the trigeminal nerve. The muscles of facial expression are innervated by the 5 branches of the facial nerve (frontal, zygomatic, buccal, marginal mandibular, and cervical)")
14
Facial skeleton series of horizontal and vertical bony buttresses that support the architecture of the face against internal and external applied forces. The facial buttresses are designed to withstand forceful impacts in order to protect the underlying vital elements such as the brain, the eyes, and other neurovascular structures

15
Facial skeleton The upper third: frontal bone and ends at the level of the supraorbital ridge. Fractures in this area most often involve the frontal sinus. The middle third :the most prominent and complex. It extends from below the supraorbital rims to the incisal edges of the upper teeth. orbits, the nasal bones, the zygoma, and the maxillary bones. The lower third of the face is the mandible and the teeth it supports. The condylar processes are considered a part of the lower third, even though they articulate with the temporal bone to form the temporomandibular joint.

18
On field assessment ABC s always come first C-spine precautions Airway
Breathing Circulation Don’t get distracted! C-spine precautions

19
A= airway ability to maintain protective oral and pharyngeal reflexes and clearance of their own airway of saliva, blood, or vomitus is preserved. Dislodged tooth fragments, dental appliances, or mandibular structural collapse may compromise the airway and should be noted. Emergent tracheostomy is seldom needed, even in severe facial fractures, unless a concomitant injury to the cranium, neck, or chest exists.

20
B= bleeding maxillary artery, superficial temporal artery, angular artery. Direct pressure is usually sufficient for initial hemostasis, followed by ligation of the bleeding vessel through the wound if it is clearly visible. If no clear source of bleeding is identified, the airway should be protected, a compressive facial dressing applied, and the athlete transferred to the nearest acute care center

21
Neurologic evaluation
Every maxillofacial injury should be considered a head injury, and patients with such injuries should be given the appropriate neurologic evaluation. The unconscious athlete is assumed to have head and neck injuries, and proper immobilization of the neck and spine should be applied immediately.

22
Sideline examination Inspection Obvious deformity Asymmetry Swelling
Bleeding, LOF Otorrhea Rhinorrhea Ecchymosis Raccoon’s eyes Battle’s sign Dysfunction Neuro exam (esp EOM) dental exam
 dental exam.")
23
Sideline Examination Palpate Special tests Orbital rims
Maxilla & malar areas Zygomatic arches Nasal bones Midface stability Jaw & alveolar ridges Temporal mandibular joints Teeth for dental trauma Malocclusion Special tests Ring test for CSF Septal hematoma Hemotympanum

26
Detailed examination Once the potentially life-threatening injuries are excluded, any soft tissue injuries and obvious asymmetries of the facial contour (suggesting underlying bony fractures) are documented. A detailed examination of the face follows. Each health care provider should develop a systematic routine in order to provide a thorough examination. A common approach is starting at the scalp and working down.
 are documented. A detailed examination of the face follows. Each health care provider should develop a systematic routine in order to provide a thorough examination. A common approach is starting at the scalp and working down.")
27
Upper third examination
confirming the integrity of the frontal branch of the facial nerve and the stability of the supraorbital rims. Having patients elevate their eyebrows is sufficient to confirm the integrity of the nerve and the frontalis muscle. Lightly touch the forehead to test for ophthalmic division of the trigeminal nerve. Gentle palpation over the supraorbital rims that elicits pain, crepitus, or the presence of a step-off suggests underlying fractures. Examine for laceration and hematoma of the scalp that may indicate underlying skull fracture.

28
Middle third examination
The eyes, the nose, the zygoma, and the maxilla make up the middle third of the face. The examination of the eyes is the most important, as injuries such as hyphema, ruptured globe, or retrobulbar hematoma are ophthalmologic emergencies.Initial determination of vision is imperative; practical methods are to ask the athletes to read the scoreboard or any printed material. Gross discrepancy of visual acuity is highly indicative of the presence of an injury. The athletes should be able to close their eyes tightly, which tests for facial nerve and orbicularis oculi muscles. Have the patients gaze in all directions in an "H" pattern to test the extraocular muscles. Limitation of or diplopia with upward gaze often suggests orbital floor fractures. Use a penlight to look for pupillary symmetry and light response. Epiphora, pain, or photophobia may indicate corneal abrasion.

29
Middle third examination
Palpate the infraorbital rims for stability. Look for discrepancy of globe position in the bony orbit (exophthalmos, enophthalmos, vertical dystopia, and telecanthus), which also suggests fracturing of the orbit.
, which also suggests fracturing of the orbit.")
30
Middle third examination
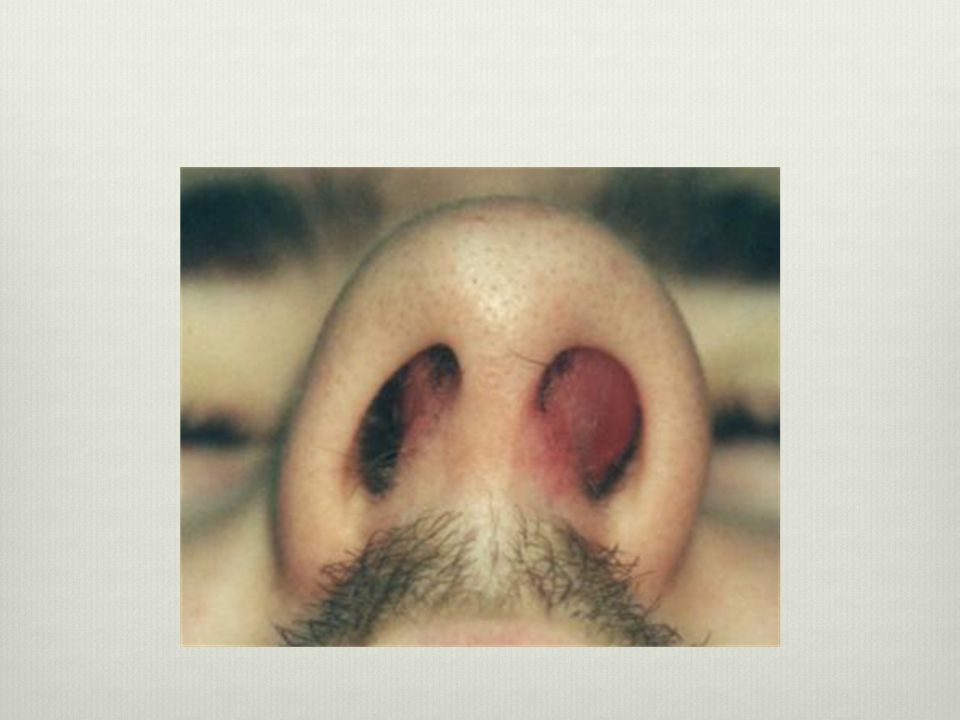
The examination of the nose includes the nasal bone, the septum, and the cartilage. The prominence of the nose leads to its frequent injuries. Deviation of the nasal dorsum, epistaxis, and edema should prompt the examiner to look for septal dislocation and septal hematoma. Failure to identify a septal hematoma may result in necrosis of the septal cartilage and subsequent perforation and collapse

31
Middle third examination
flattening of the zygomatic arch and the widening of the mid face associated with fractures. Viewing the mid face from an inferior view facilitates the detection of these asymmetries. Lightly touch the malar region to test for dysesthesia of the trigeminal nerve infraorbital branch

34
Middle third examination
Abnormal mobility of the maxilla or hard palate can be detected by grasping the anterior maxillary teeth and firmly attempting to move the maxilla in all directions while stabilizing the forehead. Examination of teeth occlusion is combined with examination of the mandible

35
Lower third examination
The lips, tongue, and cheeks are very susceptible to lacerations when compressed against the dentition. Lacerations involving the vermillion border of the lip require delicate reapproximation to avoid a visible cosmetic defect. Ask patients to pucker their lips, grin, and show their teeth to test the facial nerve branches to this area. The oral cavity must be cautiously inspected for the presence of sublingual ecchymosis, which is the pathognomic sign of a mandibular fracture.

36
Lower third evaluation
Mandibular injuries are often accompanied by pain, numbness of the jaw and teeth, trismus, and malocclusion with the maxillary teeth. The inability of an injured athlete to close his or her mouth should alert the examiner to the possibility of temporomandibular joint dislocation or fracture. Dentition should be inspected for instability or tooth fracture

37
History How? Other Injuries? Other symptoms Concussion?
Respiratory symptoms? Concussion? Symptoms Leakage of fluid (LOF)? Able to move jaw? Teeth mesh normally?
 Able to move jaw Teeth mesh normally")
38
Contusions and abrasions
Contusions represent injury of the soft tissue layers between the underlying facial skeleton and the overlying skin and are associated with varying degrees of tenderness, swelling, and ecchymosis. Keeping the head elevated and applying ice to the affected area for minutes every 2 hours is the mainstay of treatment for facial contusions. These injuries can be expected to resolve over several days to weeks. Abrasions are partial-thickness losses of skin caused by shearing forces within the compressed epidermal and dermal layers. Adequate cleansing with an antiseptic or antibacterial soap followed by twice-daily topical antibiotic ointment is usually adequate.

41
Lacerations the most common type of facial injury encountered in the athletic setting. When blunt trauma occurs over a bony prominence of the facial skeleton, a linear or stellate laceration may result. The latter is termed a burst-type laceration and, with its jagged skin edges, repair and a good aesthetic outcome are more challenging. Because of the abundant blood supply to the facial soft tissues, bleeding from a laceration may be brisk and copious. Immediate management is directed toward achieving hemostasis by applying direct pressure over the involved area with a sterile gauze pad. Once hemostasis is obtained, underlying structures can be seen more easily and should be examined carefully. Facial lacerations may be adequately cleaned with sterile saline delivered under pressure via an 18-gauge needle attached to a 20-mL syringe. This adequately removes bacteria and other debris from the wound

43
Facial lacerations After appropriate cleansing, superficial lacerations without separation of the wound edges may be closed using adhesive bandages (eg, Steri-Strips) or by applying a skin adhesive.
 or by applying a skin adhesive.")
44
Intraoral laceration Intraoral lacerations are treated much like skin lacerations. Following thorough irrigation, reapproximate the intraoral mucosa with absorbable suture material. Because delayed healing and excessive scar tissue may occur, primarily repair mucosal lacerations, including those of the tongue, whenever possible

45
Lip lacerations Compression of lip on teeth
Look for associated dental and other hard tissue injury

47
Lip lacerations Mucosa-only lacs heal well w/o sutures
Deep or thru & thru lacerations require layered repair Vermilion border: approximate border FIRST, then repair remainder (consider referral) Prophylactic abx or chlorhexidine rinse bid
 Prophylactic abx or chlorhexidine rinse bid.")
48
Tongue lacerations Irrigate, remove foreign bodies
Repair muscle with 3-0 absorbable if deeper than 5mm Repair mucosa if still necessary, absorbable is fine

49
Hematoma A collection of blood within the muscle, fascial, and dermal layers represents hematomas, which are generally seen over the zygomatic and periorbital regions. These generally resolve with the application of ice and compression. Auricular and septal hematomas deserve special attention because of their potential for perichondral injury and subsequent necrosis. A septal hematoma appears as a purple, grapelike swelling from the nasal septum. Incision and drainage followed by anterior nasal packing may prevent the possibility of septal necrosis, impaired breathing, and altered cosmesis. An auricular hematoma may result from blunt trauma as might be sustained in a boxing or wrestling match. It is noted as a firm, ecchymotic collection in the helical portion of the ear. Treatment is by incision and drainage of the hematoma, closure of incision with fine monofilament interrupted sutures, and a compressive dressing conforming to the helix and antihelix for 3 days

52
Facial bone fractures Most athletes who sustain facial bones fractures should not return to the game. A second impact to a facial bone that is already fractured may compound the fracture and convert a simple nonoperative fracture into a complex and disfiguring surgical challenge. When evaluating an athlete with a potential facial fracture, the care provider should maintain a high index of suspicion and promptly refer the patient to a facility that can adequately image and manage the injury. The following fractures discussed are those most commonly encountered in sports-related facial trauma

53
Nasal bone fracture 50% of sports-related facial fractures
The common perception of the broken nose as innocuous may account for its high rate of undertreatment. a poorly managed acute nasal fracture leads to chronic nasal deformities and, sometimes, breathing difficulties that may impair the performance of competitive athletes

56
Nasal injuries

57
Nasal bone fracture epistaxis, swelling and tenderness of the nasal dorsum, bruising around the eyes, and an obvious nasal deformity. Palpation of the nasal bones can demonstrate mobility, irregular surface, or crepitus. If the injured athlete reports a nasal obstruction during inspiration, the examiner should strongly consider a nasal/septal fracture or dislocation. The intranasal examination should be conducted under proper lighting with a nasal speculum. The examiner can spray the intranasal structures with a vasoconstrictor such as phenylephrine or oxymetazoline if that would allow for better visualization

58
Nasal bone fracture immediate cessation of the match.
Swelling that occurs over time obscures the deformity and makes acute closed reduction difficult. If swelling has also occurred, waiting at least 4-7 days for the swelling to subside before treating the nasal fracture is prudent. Treatment can be limited to a simple closed reduction of the nasal bones using topical and local anesthesia in a physician's office setting or can be a more involved open reduction of a fractured or severely dislocated septum in the operating room. The realigned septum or nasal bones are then splinted externally and internally. The splints are usually removed in 7-10 days

59
Nasal bone fracture Carefully consider the decision to return the athlete to competition and the need for nasal protection. The nasal bones generally heal sufficiently within 4-8 weeks, allowing the athlete to return to competition in contact sports. If the athlete resumes competition soon after repair, strongly recommend that he or she use a protective facial device of sufficient strength to prevent further injury

60
Orbital fracture Although common in athletes, eye injuries can almost always be prevented with the use of protective eyewear. The risk of injury to the eye is highly related to the type of sport. High-risk sports are those with high-speed projectile objects, clubs, or aggressive body contacts

61
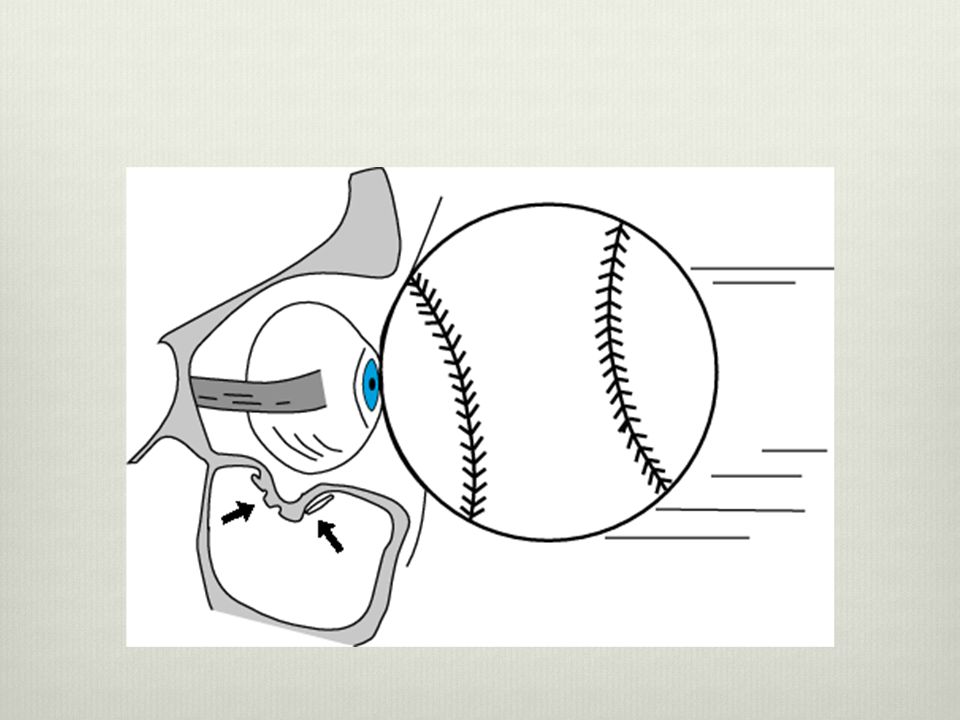
Orbital fracture The aperture of the circumferential bony rim does not allow objects with a radius greater than 5 cm to penetrate to the globe. During the examination, the circumferential bony rim should be palpated. Fractures of the orbital rim can occur at any point on the rim; however, fractures of the inferior rim are most common. These fractures can occur independently or in combination with interior wall fractures; interior wall fractures can also occur alone

62
Orbital fracture Sometimes a blow to the eye can cause an increase in intraorbital pressure, with or without fracturing the orbital rim. The thin bones of the orbital floor actually fracture to increase the volume of the orbit and dissipate the pressure that would otherwise rupture the globe. This protective fracturing is the so-called orbital blowout fracture. It can manifest with ecchymosis, enophthalmos, vertical dystopia, and numbness of the area on the ipsilateral cheek supplied by the infraorbital nerve

65
Eye injuries

66
Lid laceration repair Sequence of layered repair Tarsus 6-0 Vicryl
Orbicularis muscle 6-0 Vicryl Lid margin 6/7-0 non-abs Remainder of skin

67
Ocular blunt trauma

68
Lid laceration

69
Trap door fracture Orbital floor fracture usually in blunt trauma

70
Trap door fracture

71
Blow-out fracture

72
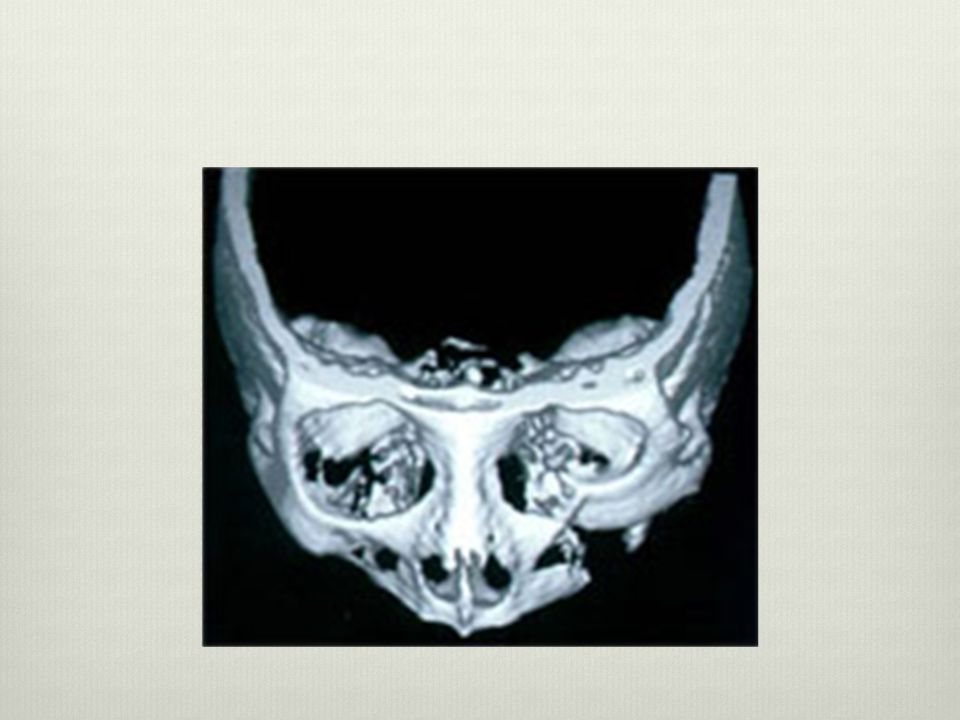
Orbital fracture Diplopia upon upward gaze can be due to a restriction of movement of the eye because of herniation of orbital fat and inferior rectus muscle through the orbital floor or due to swelling or contusion of the muscle. A facial bone CT scan with coronal views evaluating the floor of the orbit can help to differentiate the causes. Forced duction test is also helpful in differentiating the causes of diplopia and gaze limitation. In the forced duction test, the affected eye is anesthetized with a topical anesthetic, the sclera is grasped with a fine-toothed forceps at the level of the insertion of the inferior rectus muscle, and the eye is gently moved in a superior and inferior direction. If the globe moves easily, entrapment of the ocular contents can be excluded

74
Orbital fracture After the injury, if the player returns to competition before 4-8 weeks have passed, strongly recommend protective facial devices sufficient to prevent reinjury.

75
ZMC& maxillary fracture
10% of all athletic facial fractures. periorbital ecchymosis, numbness in the distribution of the infraorbital nerve over the cheek, enophthalmos, restriction of movement of the eye upon upward gaze, and depression of the cheekbone with an associated downward slant of the eye. The medial and lateral canthal tendons that support the eye attach to the medial and lateral orbital rims, respectively, so that any change in the position of the rim bones changes the axis of the intercanthal line. Any combination of these signs and symptoms may be evident.

76
ZMC& maxillary fracture
Treatment varies depending on the severity of the fracture. If surgical repair is needed, perform it within 7-10 days to prevent early fracture consolidation. Rigid fixation of these fractures is usually obtained with titanium miniplates and screws specifically designed to be used on the facial bones, using surgical approaches that minimize facial scars. research has shown that rigid internal fixation is not as strong as the patient's own intact facial skeleton. A similar blow to the repaired fracture site before the bones have healed puts the athlete at risk for a more severe fracture pattern than the initial injury, and the risk of damage to the underlying vital structures is significant. Therefore, strongly recommend that the athlete refrain from practice or competition for at least 6-8 weeks to allow the fractured bones to heal. Protective facial devices, if properly constructed, may allow the athlete to return to competition earlier

77
Facial fractures

78
ZMC fracture

79
ZMC fracture

80
Mandibular fracture 10% of all sports-related facial fractures. Results from a recent study in Austria indicate that sports accidents are the most common cause of mandibular fractures, occurring in 31.5% of the patients in that series. The mandible is a horseshoe-shaped structure that articulates with the base of the skull at the temporomandibular joints. It is a strong cortical bone that has several weak areas. It is thin at the angles, at the neck of the condyles, and at the distal body where the long root of the canine tooth and the mental foramen are located. Because of the mandible's arched shape and several weak, thin areas, the mandible commonly fractures in more than one place.

81
Mouth and jaw injuries

82
Facial fractures

83
Mandibular fracture Malocclusion, pain, swelling, difficulty opening the mouth, and intraoral bleeding are the most common signs and symptoms of a lower jaw fracture. Palpation of the mandible, visible step-offs between the teeth, and pain upon stressing the mandible also aid in the diagnosis of a fracture. Panorex view and facial bone CT (combined) are the reliable image modalities for diagnosing even the smallest mandibular fractures.
 are the reliable image modalities for diagnosing even the smallest mandibular fractures.")
84
Mandibular fractures Athletes with fractured jaws should not be allowed to return to play until healing has occurred and they are out of maxillomandibular fixation (which generally takes 6-8 weeks). A protective cage or helmet with a jaw extension can allow athletes in selected sports to return to competition earlier
. A protective cage or helmet with a jaw extension can allow athletes in selected sports to return to competition earlier.")
85
Mandibular fracture The subcondylar regions are the most commonly fractured areas of the lower jaw. These areas are thinner than the rest of the mandible, and forces generated at impact are transmitted to these areas. Subcondylar fractures can have devastating, long-term functional and cosmetic sequelae. The condylar region of the lower jaw is considered a growth center. Fractures of this region in a younger athlete who has not completed growth can result in a shortened height of the mandible with associated occlusal problems. Injuries to this region can also result in hemorrhage into the temporomandibular joint spaces and lead to fibrosis and possibly ankylosis with associated inability to move the joint

86
TMJ dislocation Cause: jaw suddenly depressed
Condyle dislocates anteriorly Spasm pulls it superiorly Signs Chin deviated to side OPPOSITE d-l Unable to close mouth Treatment: reduction ASAP Hook thumbs on third molars bilat Apply postero-inferior pressure Analgesics, soft diet, avoid opening wide for 1 week or more after dislocation

87
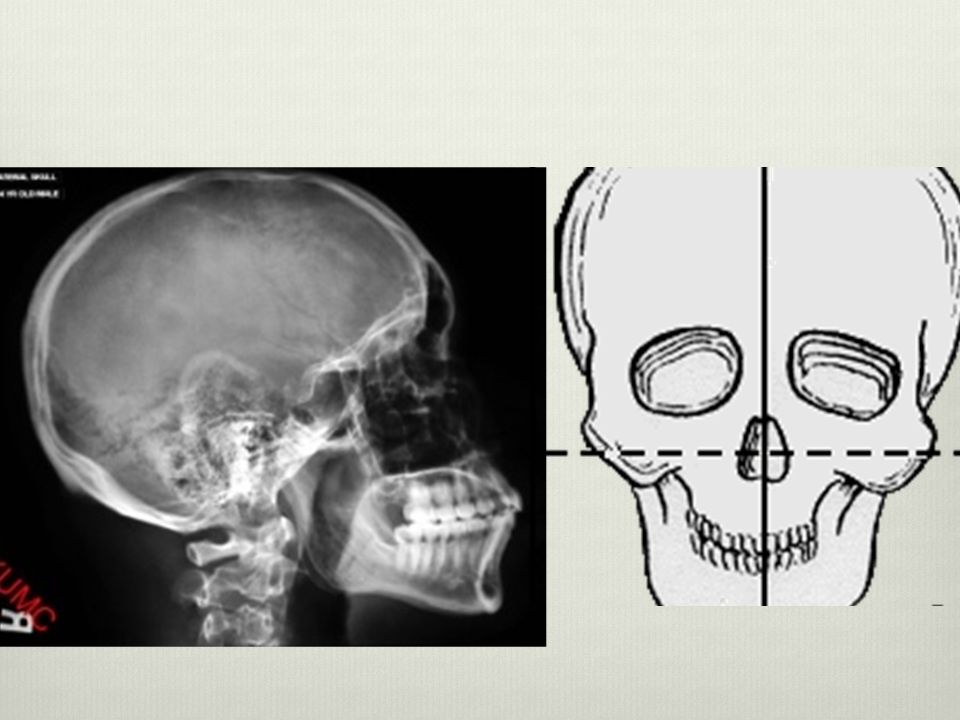
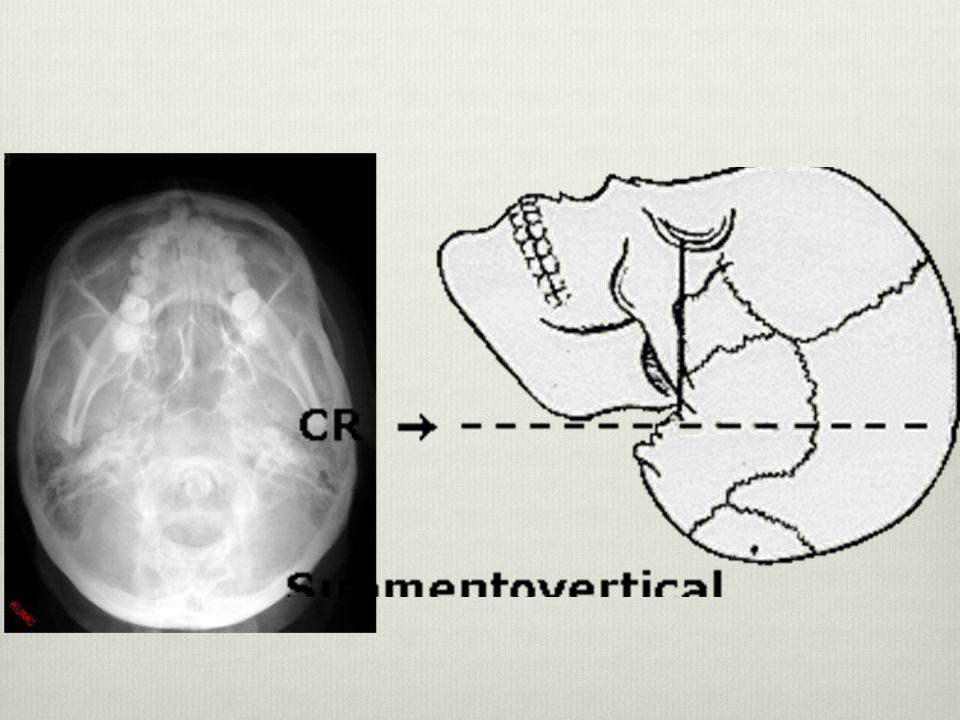
Diagnostc images Plain film x-rays CT Scan – (Hi Res) Facial series
Waters view (Occipitomental) Caldwell (PA) view Lateral Submentovertex view Lower face series Panorex Lateral oblique Other views CT Scan – (Hi Res)
 Caldwell (PA) view. Lateral. Submentovertex view. Lower face series. Panorex. Lateral oblique. Other views. CT Scan – (Hi Res)")
95
Prevention

96
Thanks for your attention

Similar presentations