Download presentation
Presentation is loading. Please wait.

1
Heart Failure in Pregnancy
Council on Women’s Health Philippine Heart Association

2
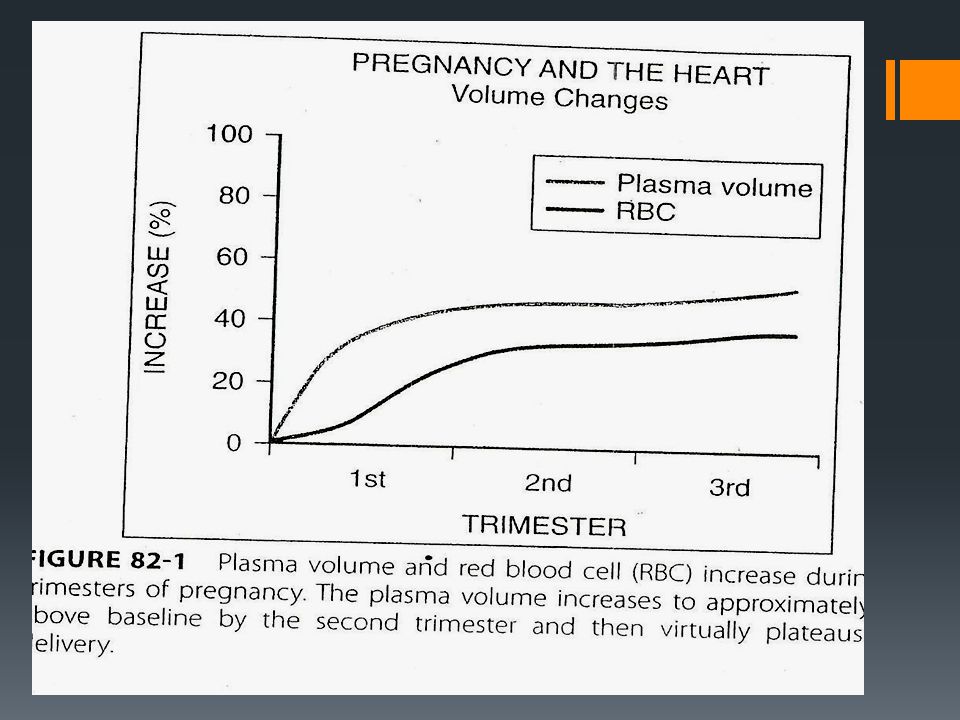
Introduction About 2% of pregnancies involve maternal cardiovascular disease Increased risk to both mother and fetus Cardiac disease may sometimes be manifested for the 1st time in pregnancy because of the hemodynamic changes Signs and symptoms of a normal pregnancy may mimic the presence of cardiac disease

3
Case Presentation AB a 22 year old married, bank teller
Visited for the first time an obstetrician 5 months PTC she had a positive pregnancy test Felt perfectly well prior to consult Few days ago started to have shortness of breath on climbing 2 flights of stairs, easy fatigability on walking 2 blocks and had palpitations

4
Pertinent PE BP- 100/60 CR- 89/min RR- 21 cycles/min
Heart-AB at 5th ICS LMCL, regular rhythm, loud S1, Grade 3/6 mid-diastolic rumbling murmur at the apex Referred by the obstetrician to a cardiologist

5
Questions Does AB have heart disease?
Is she experiencing heart failure symptoms? What are the hemodynamic changes occurring in her? What are the differential diagnoses? How should you go about managing her? Medical? Surgical? Timing? Can she tolerate the pregnancy? What is the safest mode of delivery?

6
Question: Does AB have heart disease?

10
Question: Is she experiencing heart failure symptoms?

12
Pregnancy Clinical features mimicking heart disease:
Dyspnea- due to hyperventilation, elevated diaphragm Pedal edema Cardiac impulse diffuse and shifted laterally from elevated diaphragm Jugular veins may be distended and JVP raised Systolic ejection murmurs in LPSB in 96% of pregnant women

13
Question: Evaluation of Heart Failure in Pregnancy
How should we go about evaluating AB? Evaluation of Heart Failure in Pregnancy 1. Detailed Hx and PE to determine FC 2. 12 lead ECG 3. Chest Xray - Optional 4. 2D Echo Doppler 5. Plasma B Type natriuretic peptide 6. Blood works-CBC,electrolytes, renal and thyroid function 7. TEE (seldom) 8. Fetal echocardiography
 8. Fetal echocardiography.")
14
Differential Diagnoses of Heart Failure in Pregnancy
Pneumonia Pulmonary embolism Amniotic fluid embolism Renal failure with volume overload Acute lung injury

15
High risk pregnancies Pulmonary hypertension
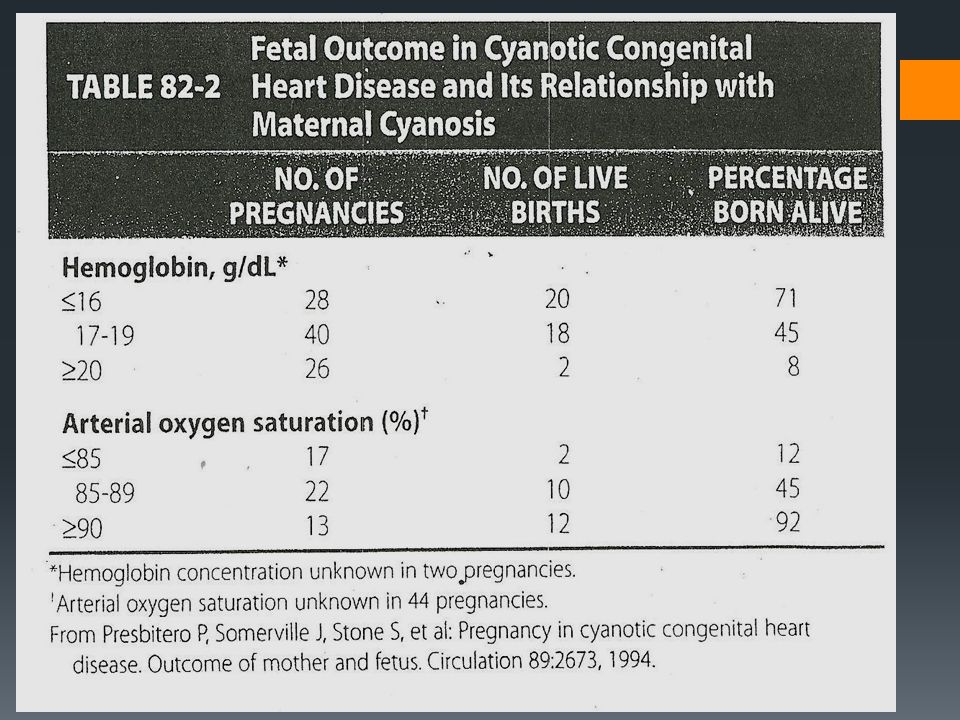
Dilated cardiomyopathy, EF≤40% Symptomatic obstructive lesions AS,MS,PS,CoA Marfan syndrome with aortic root ≥40mm Cyanotic lesions Mechanical prosthetic valves

17
Question: Cardiac Diseases in Pregnancy Risk Score Risk Scores
1. A prior cardiac event ( arrhythmia,stroke,TIA,HF) 2.Baseline NYHA FC≥II or cyanosis(saturation≤ 90% 3. Systemic ventricular systolic dysfunction 4. Left heart obstruction - MVA ≤ 2 cm - aortic valve area≤ 1.5 cm - peak flow gradient ≥ 30mm Hg What is the risk of AB? Can she tolerate her pregnancy? Risk Scores 0 - 5% risk (low) 1 - 27% risk (interm) >1 - 75% (high)
 2.Baseline NYHA FC≥II or cyanosis(saturation≤ 90% 3. Systemic ventricular systolic dysfunction. 4. Left heart obstruction. - MVA ≤ 2 cm. - aortic valve area≤ 1.5 cm. - peak flow gradient ≥ 30mm Hg. What is the risk of AB Can she tolerate her pregnancy Risk Scores % risk (low) % risk (interm) >1 - 75% (high)")
18
Management Medical NYHA Class I or II -Limit strenuous exercise
-Provide adequate rest -Supplemental iron and vitamins -Low salt diet -Regular cardiac and obstetric evaluation NYHA III and IV -May need hospitalization for close monitoring

20
Management Percutaneous valvotomy? Timing?

21
Management Surgical Cardiac surgery seldom necessary and should be avoided if possible Higher risk of fetal malformations and loss May induce premature labor Optimal time wk gestation Extracorporeal circulation- normothermic Higher pump flow rate, higher pressure with a mean of 60 mmHg Advise short bypass time

22
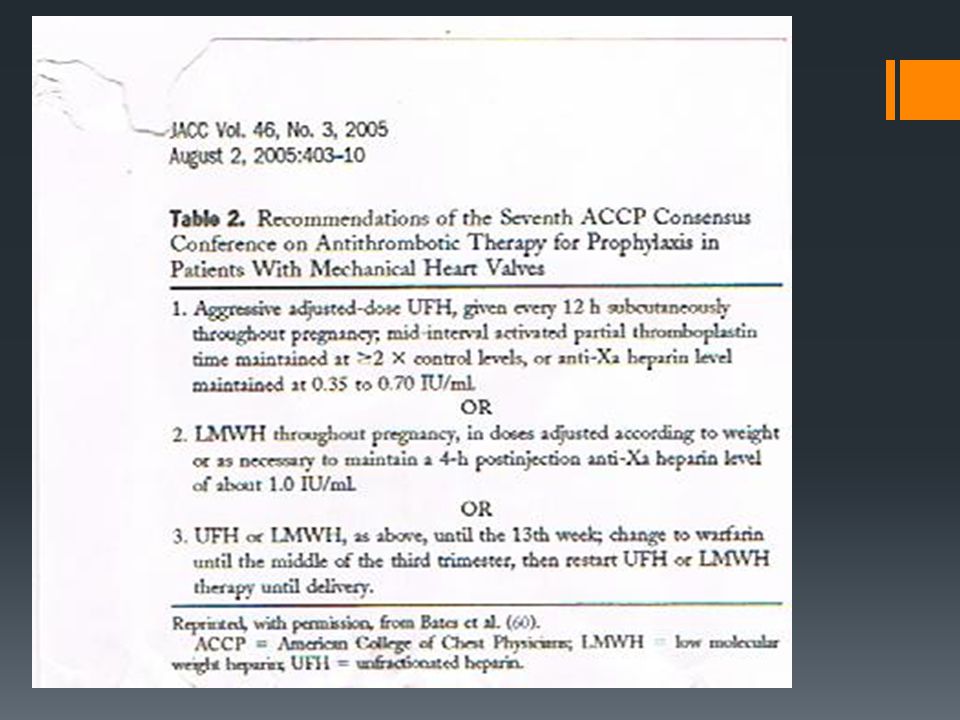
Management Anticoagulation? Warfarin Unfractionated Heparin
Low Molecular Weight Heparin

23
What is Warfarin Embryopathy?
Used in 1st trimester- teratogenic in 15-25% of cases 1. nasal cartilage hypoplasia 2. stippling of bones 3. IUGR 4. brachydactyl

24
SBE Prophylaxis? Antibiotic – a) 2 gm ampicillin IV plus 1.5 mg/Kg gentamicin IV prior to procedure, followed by one more dose of ampicillin 8 hours later If with allergy from ampicillin, 1 gm vancomycin may be used.
 2 gm ampicillin IV plus 1.5 mg/Kg gentamicin IV prior to procedure, followed by one more dose of ampicillin 8 hours later. If with allergy from ampicillin, 1 gm vancomycin may be used.")
25
What is the Safest Mode of Delivery?
Vaginal delivery is feasible and preferable CS is for an obstetric indication Exception are anticoagulated patients CS may be indicated in 1. Marfan syndrome, 2. severe pulmonary HPN 3. severe obstructive lesions eg AS

26
Physiologic Changes during Labor and Puerperium
First stage- Cardiac output increased by 15%. Each uterine contraction releases 500 ml of blood leading to increases in CO and BP, later reflex bradycardia. Second stage- Increase in intra-abdominal pressure(valsalva) causes decrease in venous return and CO Third stage- Blood loss during delivery. Vaginal- 400 ml CS- 800 ml - these lead to reduced blood volume and CO
 causes decrease in venous return and CO. Third stage- Blood loss during delivery. Vaginal- 400 ml CS- 800 ml. - these lead to reduced blood volume and CO.")
27
Hemodynamic Changes after Delivery
Abrupt increase in venous return because of autotransfusion from the uterus. Baby no longer compress the uterus. Autotransfusion of blood continues hrs after delivery. Pulmonary edema may occur.

28
Thank You Thank you

Similar presentations








 Department of Clinical Pharmacy Salman Bin AbdulAziz University College Of Pharmacy.>")










 Blood pressure ↓ Fall in TM 1 and 2, returns to baseline.>")





