Download presentation
Presentation is loading. Please wait.

1
“Oh great! We have a transplant patient on our service” Transplant for the Non-Transplant Clinician
Nicole A. Weimert, PharmD, BCPS Clinical Specialist, Solid Organ Transplantation Assistant Clinical Professor, USC-COP Medical University of South Carolina Department of Pharmacy Services

2
Objectives Provide a brief review of transplant immunology and immunosuppression Review common drug, disease, immunosuppression interactions Describe situations and solutions related to administration of immunosuppressants Discuss common case-based scenarios related to the presentation of transplant recipients with non-transplant related issues

3
Immunology 101

4
Maintaining the Balance
Infection Malignancy Life Saving Procedure Graft Function

5
Transplanted Organ = Antigen “Antigen” – any substance that causes the production of an immune response The transplanted organ is non-self and its cell surface protiens are functional antigens

6
Cells of the Immune System
Antigen Presenting Cell T cell Y Y Y Y B cell Y Y Y

7
9 steps……

8
The antigen presenting cell (APC) envelops circulating antigen
The antigen is processed within the APC into small protein fragments called peptides APC’s envelope circulating antigens of the transplanted kidney within the body and the transplanted kidney

9
The peptides bind to human leukocyte antigen (HLA)
APC The peptides bind to human leukocyte antigen (HLA) The HLA/peptide complex migrate to the cell membrane of the APC
 The HLA/peptide complex migrate to the cell membrane of the APC.")
10
The APC presents the HLA/peptide complex to T cells
T cell receptors (TCR) on T cells recognize a specific HLA/peptide T cell activate and initiate proliferation via a complex pathway TCR CD3 T cell
 on T cells recognize a specific HLA/peptide. T cell activate and initiate proliferation via a complex pathway. TCR. CD3. T cell.")
11
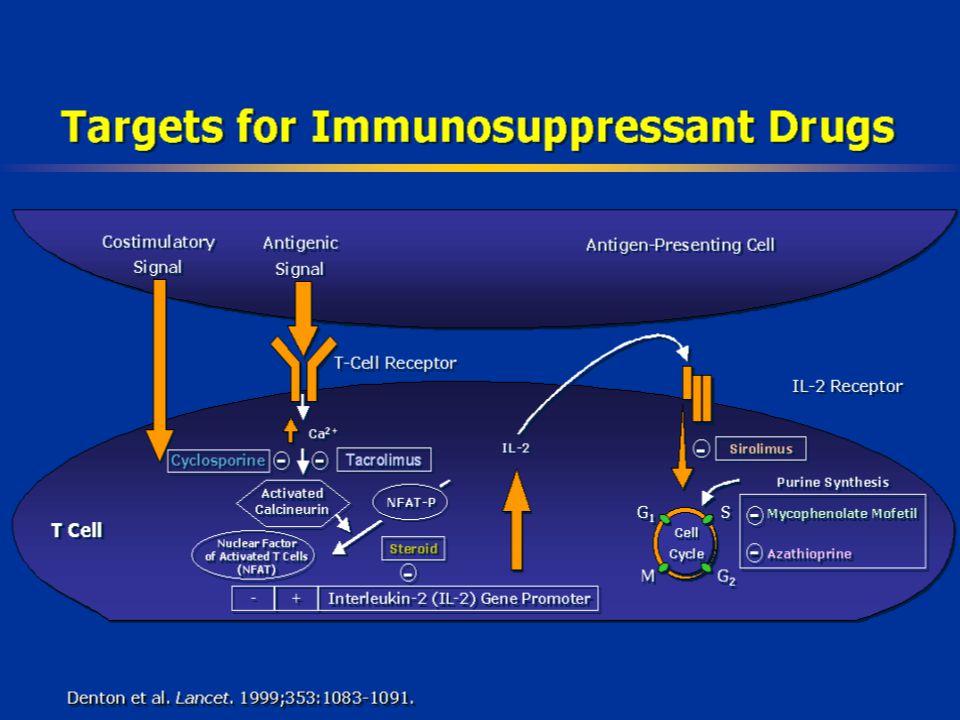
APC A T Cell cytokines IL-2 R HLA IL-2 IL-2 IL-2 Calcineurin TCR NF-AT
Binding of the TCR to the HLA/peptide complex A NF-AT DNA synthesis IL-2 gene T Cell

12
B cell activation Y Y Y Y Y Y Y
cytokines Y B cell Y Plasma cell T cell Y Y Y Y Y Cytokines activate and induce proliferation of B cells B cells produce antibodies specific to the antigen

13
Rejection Y Y Y Y Y Y Y T cells directly attack the transplanted organ
B cell Y Y Y Y Y T cells directly attack the transplanted organ Antibodies produced by B cells lead to the destruction to the transplanted organ

14
The Immune System Specificity : distinguish between non-cross reacting antigens. Memory: quick and vigorous response to a subsequent but similar pathogen or antigen Mobility: local reactions to provide systemic protection. Replication: amplifies the immune response. Redundancy: produce components with the same biological effect but produced from multiple cell lines

21
Review of Drug Disease State Interactions
Common Issues Review of Drug Disease State Interactions

22
Question: This transplant patient was admitted for urosepsis
Question: This transplant patient was admitted for urosepsis. What should we do with their immuosuppression?

23
Infection and Transplant
Facts: Inefficient immune systems Be aggressive with initial treatment Consider the consequences of organ dysfunction if immunosuppression is held How far out from transplant

24
Infection and Transplant
Facts: Inefficient immune systems Consider the consequences of organ dysfunction if immunosuppression is held Heart versus Kidney How far out from transplant

25
Infection and Transplant
Facts: Inefficient immune systems Consider the consequences of organ dysfunction if immunosuppression is held How far out from transplant Risk of acute rejection decreases further out from transplant Have they had a recent rejection episode Are they compliant

26
What should we stop first?
Pick the agent that has the broadest spectrum of activity: Corticosteroids Mycophenolic Acid Tacrolimus Cyclosporine

27
What should we stop first?
Pick the agent that has the broadest spectrum of activity: Corticosteroids Mycophenolic Acid Tacrolimus Cyclosporine Why can’t we just stop the corticosteroids?

28
Adrenal Axis Suppresion
Exposure to corticosteroids for < 3 weeks rarely induces clinical adrenal suppression Kronenberg: Williams Textbook of Endocrinology, 11th ed.

29
Question: Supplementation
Do transplant recipients on chronic steroids need supplemental doses during periods of acute stress (surgery, infection)? YES or NO
 YES or NO.")
30
Question: Supplementation
Do transplant recipients on chronic steroids need supplemental doses during periods of acute stress (surgery, infection)? DEPENDS Concerns: Impaired wound healing Further immunosuppression Transplantation. 1991;51:
 DEPENDS. Concerns: Impaired wound healing. Further immunosuppression. Transplantation. 1991;51:")
31
Historical Evidence Bromberg et al.
Prospective evaluation of kidney transplant recipients admitted with physiological stress Surgery, sepsis, metabolic abnormalities N=40 Did not receive supplemental steroid doses Remained on admission dose (5 to 10 mg/day) Measurements Serum cortisol levels elevated in 56% Urine cortisol levels elevated in 79% Cosyntropin stimulation tests overestimated adrenal suppression in 63% Transplantation. 1991;51: J Am Coll Surg. 1995;180:
 Measurements. Serum cortisol levels elevated in 56% Urine cortisol levels elevated in 79% Cosyntropin stimulation tests overestimated adrenal suppression in 63% Transplantation. 1991;51: J Am Coll Surg. 1995;180:")
32
Current Evidence Corticosteroids in Septic Shock: Meta-Analysis
15 trials (n = 2022) No recommendations for which populations would benefit Corticosteroid Therapy of Septic Shock (CORTICUS) Efficacy and safety of low-dose hydrocortisone therapy in septic shock Multi-center, double blind, randomized, placebo controlled Inclusion criteria: adult, sepsis within 72 hrs Exclusion criteria: chronic immunosuppression or steroid use No change in 28 day mortality N Engl J Med. 2008;358: BMJ 2004;329:
 No recommendations for which populations would benefit. Corticosteroid Therapy of Septic Shock (CORTICUS) Efficacy and safety of low-dose hydrocortisone therapy in septic shock. Multi-center, double blind, randomized, placebo controlled. Inclusion criteria: adult, sepsis within 72 hrs. Exclusion criteria: chronic immunosuppression or steroid use. No change in 28 day mortality. N Engl J Med. 2008;358: BMJ 2004;329:")
33
Recommendations: Infected Transplant Recipients
Assess the severity of illness and relative risk for acute rejection Discontinue adjunctive agent and minimize other immunosuppression Supplement corticosteroids in the setting of pressor resistant progressive septic shock

34
Question: We performed bowel surgery on this transplant patient, how do we convert their immunosuppression to IV?

35
Question What is the PO to IV conversion for calcineurin inhibitors?
1:1 2:1 3:1 4:1

36
Question What is the PO to IV conversion for calcineurin inhibitors?
1:1 2:1 3:1 4:1

37
Conversion Considerations
Simple answer: 3:1 Tacrolimus.package insert.Astellas.Revised April 2006 Int J Clin Pharmacol Ther. 2004;42:

38
Conversion Considerations
Simple answer: 3:1 Why this does not work: Bioavailability: Tacrolimus : <30% Trough concentrations have good correlation with ACU (r2=0.93) Cyclosporine : erratic, formulation dependent Tacrolimus.package insert.Astellas.Revised April 2006 Int J Clin Pharmacol Ther. 2004;42:
 Cyclosporine : erratic, formulation dependent. Tacrolimus.package insert.Astellas.Revised April Int J Clin Pharmacol Ther. 2004;42:")
39
Conversion Considerations
Simple answer: 3:1 Why this does not work: Bioavailability: Tacrolimus : <30% Trough concentrations have good correlation with ACU (r2=0.93) Cyclosporine : erratic, formulation dependent Race differences: Oral bioavailability in African-Americans is 20 and 50% lower than in Caucasians Tacrolimus.package insert.Astellas.Revised April 2006 Int J Clin Pharmacol Ther. 2004;42:
 Cyclosporine : erratic, formulation dependent. Race differences: Oral bioavailability in African-Americans is 20 and 50% lower than in Caucasians. Tacrolimus.package insert.Astellas.Revised April Int J Clin Pharmacol Ther. 2004;42:")
40
Conversion Considerations
Infusion Continuous versus intermittent q 12 hours Hypertension Renal insufficiency Tubing Must use non-PVC tubing Drawing levels - will contaminate tubing Central lines, port-a-cath Am J Health System Pharm.2008;65:

41
Recommendations: Converting Calcineurin Inhibitors to IV
Use a designated line When in doubt start low Empiric weight based dosing Tacrolimus 0.01 – 0.03 mg/kg/day Cyclosporine 3 – 5 mg/kg/day Use conversion “Soft” maximum doses for initiation Tacrolimus >4 mg in 24 hours Cyclosporine > 50 mg in 24 hours

42
Question: So we have this transplant patient on cyclosporine
Question: So we have this transplant patient on cyclosporine. What level should this patient be at?

43
Appropriate Level Several variables: Center Patient Organ
Time since transplant Rejection history Current clinical situation Concurrent immunosuppression

44
Appropriate Level Several variables: Center Patient Organ
Time since transplant Rejection history Current clinical situation Concurrent immunosuppression Contact the patient’s transplant coordinator

45
Question: So we have this transplant patient on cyclosporine
Question: So we have this transplant patient on cyclosporine. How often should we be getting levels?

46
Measuring Levels Compliance Impending drug interactions Efficacy
Measure of allograft function Toxicity Elevated levels may induce renal artery vasoconstriction Liver insufficiency Increased levels Diarrhea Pediatr Transplant. 2005;9: Am J Transplant. 2005;5:

47
Question: We have to start an azole antifungal agent
Question: We have to start an azole antifungal agent. How should we adjust their medicines and when will we see the effect?

48
Question What is the primary mechanism of fluconazole associated with elevations in the calcineurin inhibitor level? Liver CYP450 inhibition Intestinal P-glycoprotein inhibition Protein binding Intestinal CYP450 inhibition

49
Question What is the primary mechanism of fluconazole associated with elevations in the calcineurin inhibitor level? Liver CYP450 inhibition Intestinal P-glycoprotein inhibition Protein binding Intestinal CYP450 inhibition

50
Azole Antifungal Variable and requires frequent monitoring
Cyclosporine: Romero et al. Double-blind, placebo controlled cross over, oral voriconazole Stable renal transplant recipients (n=53) 2.48 fold increase in CsA trough levels Clin Pharmacol Ther. 2002;71: Eur J Clin Pharmacol. 2008;64:89-91
 2.48 fold increase in CsA trough levels. Clin Pharmacol Ther. 2002;71: Eur J Clin Pharmacol. 2008;64:")
51
Azole Antifungal and Calcineurin Inhibitor
If patient has had stable levels Reduce dose in half Onset of interaction 24 to 72 hours Prolonged Magnitude of interaction for inhibitor Increased with oral administration

52
* Indicates potent inhibitor or inducer
Immunosuppressant Interacting Drugs Mechanism Consequence Clinical Management calcinuerin inhibitors (cyclosporine and tacrolimus) and sirolimus clarithromycin*, erythromycin*, ketoconazole*, itraconazole*, fluconazole, voriconazole*, fluoxetine, fluvoxamine, citalopram, nefazadone*, diltiazem*, verapamil*, delaviridine*, ritonavir*, cimetidine*, grapefruit juice*, amiodarone, saquinavir, nelfinavir, indinavir, amprenavir, chloramphenicol* Inhibit CYP450 3A4 isoenzyme in the liver and intestines Increase the concentration and total AUC of the IS Either prospectively decrease the IS dose or monitor trough concentrations more closely and adjust doses accordingly carbamazepine*, dexamethasone, phenobarbital*, phenytoin*, St. John’s Wort*, rifampin*, rifabutin*, efavirenz*, nevirapine*, nafcillin, clindamycin Induce CYP450 3A4 isoenzyme in the liver and intestines Decrease the concentration and total AUC of the IS Either prospectively increase the IS dose or monitor trough concentrations more closely and adjust doses accordingly calcinuerin inhibitors (cyclosporine and tacrolimus), sirolimus, and mycophenolate mofetil cholestyramine, colestipol, probucol, sevelamer, antacids (magnesium and aluminum containing)**, iron containing products** Bind to IS and prevents absorption Avoid concomitant administration with IS and monitor trough concentrations azathioprine allopurinol Inhibits metabolism by inhibiting xanthine oxidase Increases the concentration and total AUC of azathioprine Avoid use together or prospectively reduce azathioprine dose to 1/3 or 1/4 normal dose and monitor for increased toxicity * Indicates potent inhibitor or inducer ** Only occurs with mycophenolate mofetil
 and sirolimus. clarithromycin*, erythromycin*, ketoconazole*, itraconazole*, fluconazole, voriconazole*, fluoxetine, fluvoxamine, citalopram, nefazadone*, diltiazem*, verapamil*, delaviridine*, ritonavir*, cimetidine*, grapefruit juice*, amiodarone, saquinavir, nelfinavir, indinavir, amprenavir, chloramphenicol* Inhibit CYP450 3A4 isoenzyme in the liver and intestines. Increase the concentration and total AUC of the IS. Either prospectively decrease the IS dose or monitor trough concentrations more closely and adjust doses accordingly. carbamazepine*, dexamethasone, phenobarbital*, phenytoin*, St. John’s Wort*, rifampin*, rifabutin*, efavirenz*, nevirapine*, nafcillin, clindamycin. Induce CYP450 3A4 isoenzyme in the liver and intestines. Decrease the concentration and total AUC of the IS. Either prospectively increase the IS dose or monitor trough concentrations more closely and adjust doses accordingly. calcinuerin inhibitors (cyclosporine and tacrolimus), sirolimus, and mycophenolate mofetil. cholestyramine, colestipol, probucol, sevelamer, antacids (magnesium and aluminum containing)**, iron containing products** Bind to IS and prevents absorption. Avoid concomitant administration with IS and monitor trough concentrations. azathioprine. allopurinol. Inhibits metabolism by inhibiting xanthine oxidase. Increases the concentration and total AUC of azathioprine. Avoid use together or prospectively reduce azathioprine dose to 1/3 or 1/4 normal dose and monitor for increased toxicity. * Indicates potent inhibitor or inducer. ** Only occurs with mycophenolate mofetil.")
53
Question: Can we cath a patient with a kidney transplant who had marginal renal function?

54
Cardiovascular Disease and Renal Transplant Recipients
Annual risk of death from a cardiovascular related event 3.5% to 5% 50 fold higher than the general population Transplantation 2006;15: J Am Soc Nephrol 1998; 9:S16

55
Contrast Induced Nephropathy
Definition: Absolute (Scr≥0.5 mg/dL) or relative (≥25%) increase in after exposure to contrast Occurs within 24 to 48 hours following exposure Peak 3 to 5 days with a return to baseline Etiology Direct toxicity to renal tubular epithelium, oxidative stress, and ischemic injury Catheterization and Cardiovascular interventions.2008;71:62-72
 or relative (≥25%) increase in after exposure to contrast. Occurs within 24 to 48 hours following exposure. Peak 3 to 5 days with a return to baseline. Etiology. Direct toxicity to renal tubular epithelium, oxidative stress, and ischemic injury. Catheterization and Cardiovascular interventions.2008;71:")
56
Clinical Pearls Do not withhold life-saving treatment
Reversible damage from contrast Can be attenuated with adequate hydration Other pharmacological interventions may decrease the length and severity of injury Hydration N-acetylcysteine Sodium bicarbonate

57
Pre-Treatment for All Transplant Recipients

58
Question: What about the generic immunosuppressants?

59
Generic Use in Transplant
Generic Timeline Product Patent Expired Generic Approved Generic Use in Transplant Imuran® (Azathioprine) 1979 1996 No difference in outcomes Neoral® (Cyclosporine) 1995 Increased rejection rates Prograf® (Tacrolimus) April 2008 Pending NDAs Unknown Cellcept® (mycophenolate mofetil) May 2009
 No difference in outcomes. Neoral® (Cyclosporine) Increased rejection rates. Prograf® (Tacrolimus) April Pending NDAs. Unknown. Cellcept® (mycophenolate mofetil) May")
60
The Ongoing Discussion in Transplant Circles
Controversy over the current FDA approval process for generic medication Bioequivalence study – 18 – 36 healthy human subjects 80% equivalent area under the curve 2001 American Society of Transplantation Scientific Forum Specifically addressed cyclosporine generic formulations Am J Transplant.2003;3:

61
Historical Concern Taber et al. Cyclopsorine microemulsion products
Gengraf® (n=88) vs Neoral® (n=100) Retrospective review Acute rejection within 6 months of transplant 39% versus 25%, p=0.04 Second rejection 19% versus 8%, p=0.02 Higher variability in cyclosporine concentrations in patients treated with Gengraf® Transplantation.2005;80:
 vs Neoral® (n=100) Retrospective review. Acute rejection within 6 months of transplant. 39% versus 25%, p=0.04. Second rejection. 19% versus 8%, p=0.02. Higher variability in cyclosporine concentrations in patients treated with Gengraf® Transplantation.2005;80:")
62
New Generics Tacrolimus Mycophenolic Acid
More predictable kinetics, better correlation with AUC Mycophenolic Acid Two formulations currently Unpredictable kinetics

64
MUSC Transplant PharmDs
Nicole A. Weimert, Pharm.D., BCPS Clinical Pharmacy Specialist, Solid Organ Transplant Clinical Assistant Professor of Pharmacy MUSC Department of Pharmacy Services 150 Ashley Ave Charleston, SC (843) office (843) fax Dave Taber, PharmD, BCPS Pharmacy Clinical Specialist - Transplant Clinical Assistant Professor, SCCM MUSC Department of Pharmacy Services PO Box Ashley Avenue - 6th floor RTA Charleston, SC Tel: (843) Fax: (843)
 office (843) fax. Dave Taber, PharmD, BCPS Pharmacy Clinical Specialist - Transplant Clinical Assistant Professor, SCCM MUSC Department of Pharmacy Services PO Box Ashley Avenue - 6th floor RTA Charleston, SC Tel: (843) Fax: (843)")
65
“Oh great! We have a transplant patient on our service” Transplant for the Non-Transplant Clinician
Nicole A. Weimert, PharmD, BCPS Clinical Specialist, Solid Organ Transplantation Assistant Clinical Professor, USC-COP Medical University of South Carolina Department of Pharmacy Services

Similar presentations











 Kingsbrook Jewish Medical Center Clinical Instructor of Pharmacy Practice.>")













