Download presentation
Presentation is loading. Please wait.

1
Eczema, Two Thousand Rashes and Three Creams
A Dermatology Primer for Mid Level Practitioners

2
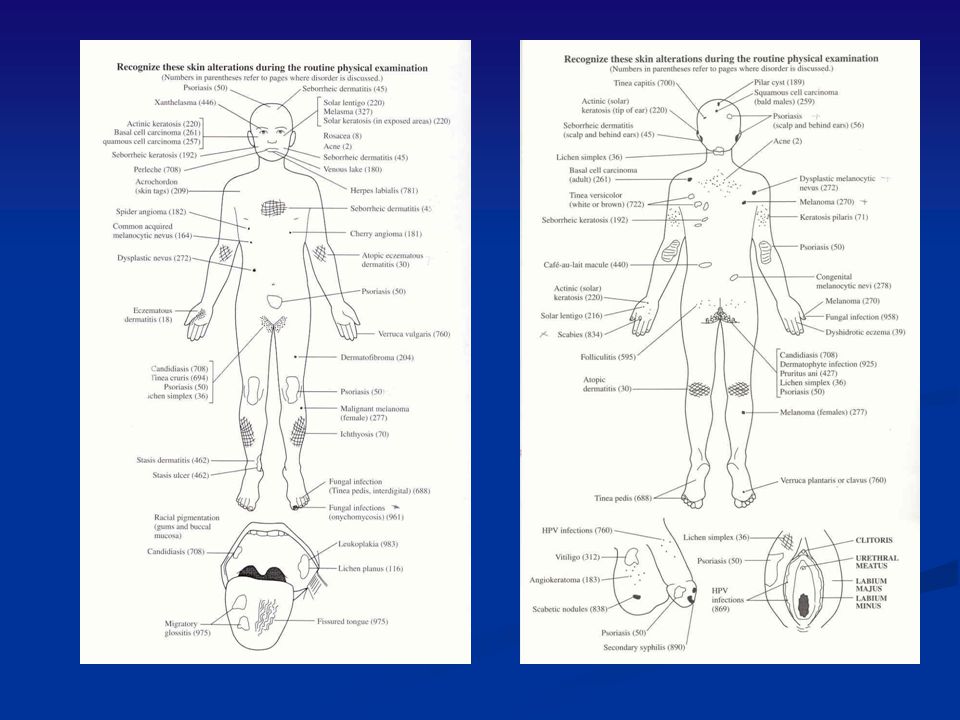
Critical components of the physical exam of the skin should include:
Type Color Shape Arrangement Duration Distribution

3
Adequate history should include:
Skin symptoms Constitutional symptoms Travel/Occupation Systems review Self care

4
Types of lesions Macule Papule-plaque Wheal Nodule Cyst Vesicle-bulla
Ulcer Pustules Hyperkeratosis Exudative: dry/wet Erosion Scar Lichenification

5
Shapes of Lesions The shape of a lesion frequently gives clues to the etiology of the skin lesion. Shapes include lesions that are: round, polygonal, polycyclic, annular, iris, serpiginous, umbilicated,and target. Margination is also important – are the lesions well or ill defined Arrangement – are the lesions grouped or disseminated

6
Distribution of Lesions
A significant number of skin diseases are limited to specific regions of the body Are the lesions isolated, localized, regional, or generalized Are the lesions symmetrical; limited to exposed areas, sites of pressure, or intertriginous areas

8
Eczema - Common Definitions
Any itching rash Any red itching rash Any red itching rash that has scales or is dry The itch that rashes Any rash that cannot otherwise be identified

9
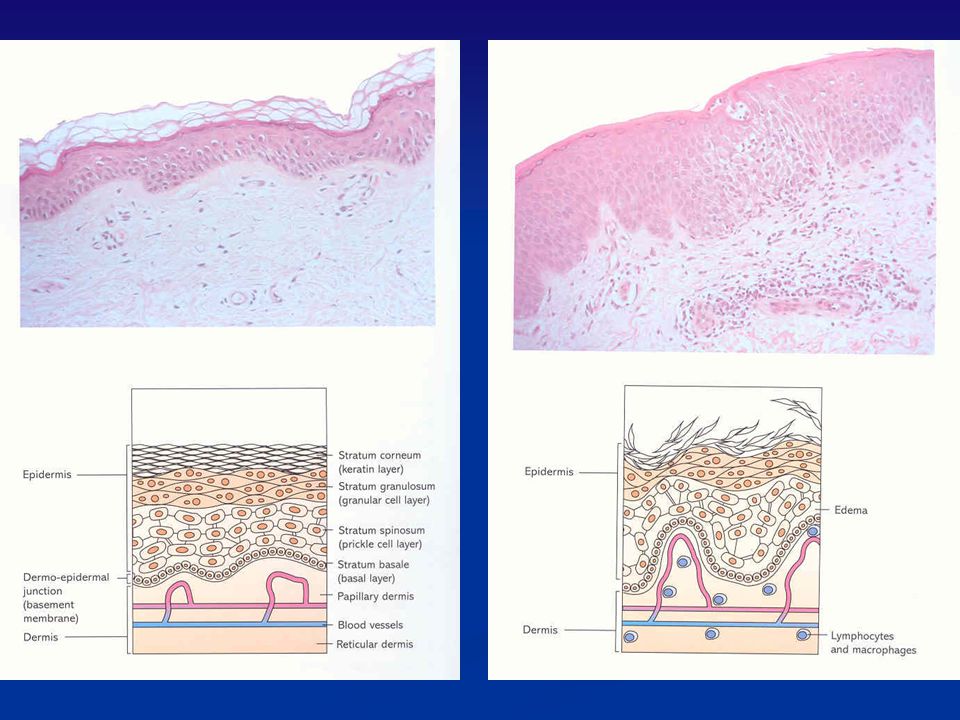
Eczema-Dermatological Definition
An acute, subacute but usually chronic pruritic inflammation of the epidermis and the dermis, often occurring in association with a personal family history of hay fever, asthma, allergic rhinitis or atopic dermatitis. 1 1 Color Atlas and Synopsis of Clinical Dermatology

10
Characteristics of Acute Eczema
Well demarcated plaques of erythema and edema on which are superimposed and closely spaced small vesicles filled with clear fluid with punctate erosions and crusting Distribution may be isolated and localized or general

11
Acute Eczema (Note the erythema, vesicles and swelling)
Term dyshidrotic is a misnomer as sweat glands are not involved Also known as pompholyx

13
Characteristics of Subacute Eczema
Plaques of mild erythema with small dry scales and or superficial desquamation, sometimes associated with small red, pointed or round papules Distribution may be isolated and localized or general

14
Subacute Eczema Note erythema, swelling and desquamation

15
Characteristics of Chronic Eczema
Plaques of lichenification with deepening of the skin lines with satellite, small, firm flat or round top papules, excoriations and pigmentations or mild erythema Distribution – isolated and localized or generalized

16
Chronic Eczema Note lichenification, scaling and fissuring

17
Acute - Subacute - Chronic
Swelling and erythema Punctate erythema, desquamation Lichenification

18
Acute, Subacute or Chronic?
Check for erythema, swelling, desquamation, lichenification

19
Acute, Subacute or Chronic?
Check for erythema, swelling, desquamation, lichenification

20
Classification of Eczema/Dermatitis
Historically Endogenous (occurring from within) dermatitis was given the name “eczema” Exogenous dermatitis (occurring from without) was termed “dermatitis”
 dermatitis was given the name eczema Exogenous dermatitis (occurring from without) was termed dermatitis")
21
Classifications of Eczema
Endogenous Atopic or IgE Seborrheic Discoid or nummular Pompholyx Venous Asteatotic Juvenile plantar Erythoderma Exogenous Allergic Toxic irritant contact Photosensitive

22
Atopic/IgE Eczema (endogenous or exogenous?)
Characteristics: 60% have onset in the first year of life Influenced by genetics and environmental factors More common in males that females Ethnicity may be a factor –less common in Asians; more common in Westerners and higher socioeconomic families Theory is - manifestation of well nourished immune system rarely challenged by infection Rare to have adult onset 2/3 of patients have family history of asthma, hay fever or allergic rhinitis

23
Atopic/IgE Eczema cont.
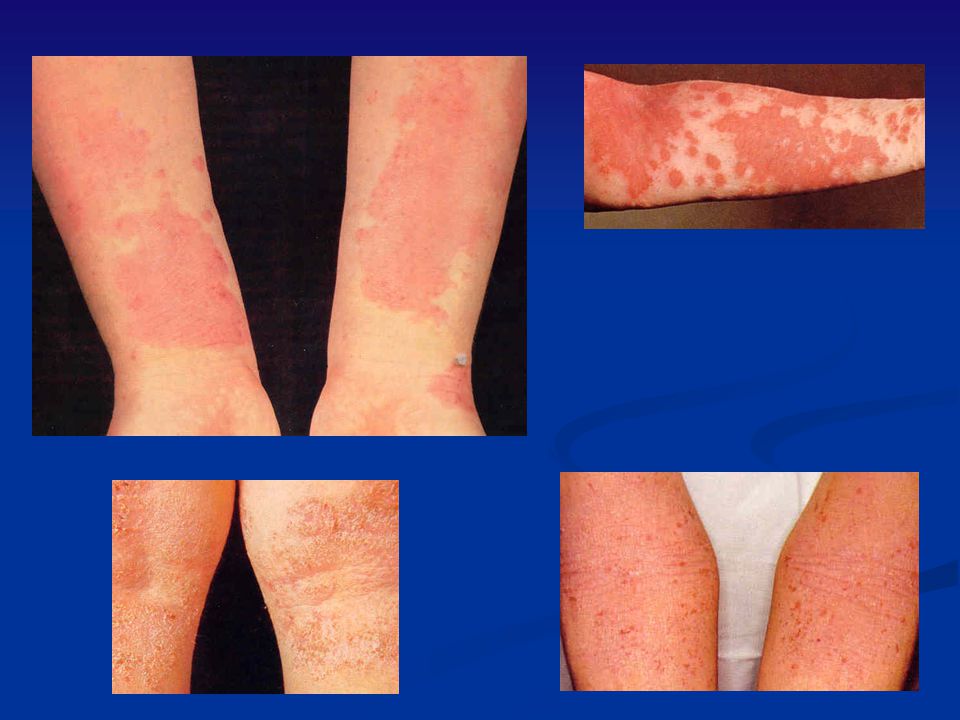
Characteristics: May persist months to years All patients have dry skin Exacerbations caused by allergens, stress, hormones, climate, skin dehydration Physical characteristic may include all phases Distinctive Characteristics: Lesions are usually bilateral Located frequently in skin folds/creases and flexor surfaces

24
Atopic/IgE Eczema Distribution
Note: Bilateral Skin folds and flexor surfaces

25
Atopic/IgE Eczema cont.
Triggers: Irritants Dry skin; bathing without moisturizing Harsh/perfumed soaps, detergents Disinfectants Contact with wool, occupational chemicals/fumes Allergens Dust mites Pet dander (cat more allergenic than dog) Pollens, seasonal and molds Foods- strawberries, carrots
 Pollens, seasonal and molds. Foods- strawberries, carrots.")
26
Atopic/IgE Eczema cont.
Triggers (cont’d): Infections Bacterial Viral Cold and other URI viruses GI viruses Fungal Environmental Extremes in temperature and/or humidity Perspiration Stress
: Infections. Bacterial. Viral. Cold and other URI viruses. GI viruses. Fungal. Environmental. Extremes in temperature and/or humidity. Perspiration. Stress.")
27
Atopic/IgE Eczema cont.
Confused with: Scabies, seborrhea, psoriasis and, contact dermatitis

28
Atopic/IgE Eczema cont.
Treatment: Avoid scratching, clean and cool environment, use of soap substitutes Emollients Topical steroids Topical immunomodulators –tacrolimus Systemic antihistamines Soaks Tar preparations

29
Atopic/IgE Dermatitis

30
Allergic (Contact)Eczema (exogenous or endogenous?)
Characteristic: Delayed, cell mediated hypersensitivity Strong sensitizer results in reaction soon after exposure Weak sensitizer my take months or years to develop reaction Age does not influence capacity for sensitization but more common in adults Black skin is less susceptible Important cause of disability in industry Non seasonal

31
Allergic (Contact) Eczema cont.
Characteristics: usually clears quite rapidly on withdrawal of offending agent may appear as erythematous papules, vesicles or bullous more common where epidermis is thinner Distinctive Characteristics: Initial lesions usually limited to contact area not bilateral lesions with sharp borders or angles are pathognomonic

32
Causes of Allergic/Contact Eczema
Metals- nickel, platinum (10% of women) Detergents Plants and fibers Chemicals and dyes Polyethylene glycol and polysorbate 60 Topical antibiotics and medications Animal keratin
 Detergents. Plants and fibers. Chemicals and dyes. Polyethylene glycol and polysorbate 60. Topical antibiotics and medications. Animal keratin.")
33
Allergic/Contact Eczema cont.
Treatment – remove causative agent, Burow’s soaks 1:40, or saline 1tsp/pt warm water, Aveeno or oatmeal baths, calamine Systemic antihistamines Topical steroids, oral steroid taper Antibiotics for secondary infection Confused with – Atopic eczema, seborrhea, HSV

34
Allergic/ Contact Eczema Distribution

35
Allergic/ Contact Eczema Distribution

36
Note: distribution

37
Note: Linear distribution with satellite lesions

38
What do you think?

39
Bilateral but…..

40
Subacute Allergic Eczema
Note slight swelling and erythema No lichenification Location – what could be the cause?

41
Chronic Allergic Eczema
Note the hyperkeratosis, lichenification and fissuring

42
Toxic / Irritant Eczema (occurring in non allergic skin)
Characteristics: Accounts for 75% of exogenous eczema Age, race and sex are insignificant Results from repeated exposure to toxic or subtoxic agents Severity of skin symptoms vary with the individual and the type of irritant and the length of contact Includes sx of itching, stinging and burning Usually associated with chronic disturbance of the barrier function of the skin

43
Toxic/Irritant Eczema cont.
Common causes: Repeated exposure to alkaline detergents Repeated exposure to organic solvents Corrosive agents Industrial chemicals Chronic self perpetuating habits that irritate the skin

44
Toxic/Irritant Eczema cont.
Treatment: Remove the cause Application of emollients Use of soap substitutes Barrier creams Borrow’s or potassium permanganate soaks twice daily Biopsy/testing- usually not necessary

45
Acute Toxic/Irritant Eczema
Note: distribution, swelling and weeping

46
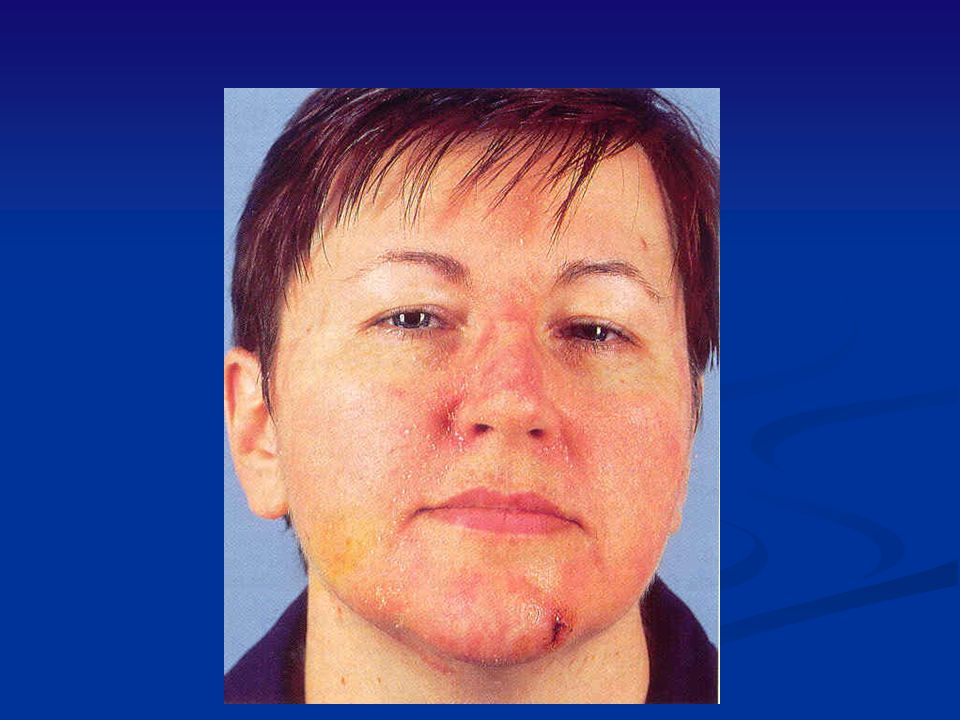
Subacute Toxic/Irritant Eczema
Lip licking often seen in children who have atopic eczema Variant of irritant eczema compare

47
Chronic Toxic/Irritant Eczema
Note:papulosquamous dermatosis with hyperkeratosis, maceration, fissuring and erosions Eruptions tend to be sore rather than itching

48
Acute, subacute, or chronic?
Swelling? Erythema? Desquamation? Lichenification?

49
Comparison of Classifications of the 3 common types of eczema
ACUTE Atopic IgE Toxic/ Irritant Allergic Contact Erythema X Papules NA Vesicles Erosions Crusts Scales Sharp/ confined Spreading peripherally Flexor surfaces, neck, eye lids, d foot Onset rapid Before age 12 Usually as adult Onset slow Concentration L/H H L Incidence Other signs Anyone Sensitized

50
Comparison of Classifications
Chronic Atopic IgE Toxic/Irritant Allergic/Contact scaling X fissues crusts NA papules excoriation lichenification Periorbital pigmentation Infraorbital folds in the eyelids Foillicular papules X more common in the black pop.

51
Pompholyx (from Greek word meaning blister)
Characteristics: Intense itching and burning proceed lesions Blisters and vesicles on hands/ feet Becomes highly exudative Dries up in about 2 wks leaving painful fissuring Acute symptom of a chronic problem Usually no cause but can be due to trichophytin and associated with fungal infection of the feet

52
Pomhpolyx cont. Treatment: Avoidance of soap Emollients
Soaks ( burrows or potassium permanganate) Potent or very potent topical steroids with or with occlusion Antibiotics for infection Systemic steroids Coal tar extracts Biopsy/testing- usually not necessary
 Potent or very potent topical steroids with or with occlusion. Antibiotics for infection. Systemic steroids. Coal tar extracts. Biopsy/testing- usually not necessary.")
53
Pompholyx Where else should you look? What else might this be call?

54
Nummular Eczema Characteristics:
usually -personal or family history of allergy, especially asthma, hay fever, and childhood eczema Distinctive Characteristics - Coin-shaped papulovesicular patches that develop in to scaling and crusting lesions; lesions may be as large as 4-5cm in diameter with distinct margins, initial eruptions on arms and legs; intense itching; tends to be chronic

55
Nummular Eczema cont. Characteristics:
Most severe during winter; may be aggravated by systematic administration of iodine or bromine; secondary bacterial infections are common Treatment: skin hydration, topical corticosteroids, intralesional injection, coal tar ointments, UVB treatment, treat secondary infection

56
Nummular Eczema cont. Confused with – contact dermatitis/eczema, atopic eczema, psoriasis, impetigo, tinea corporis Biopsy/testing – not usually necessary

57
Note: Coin shaped lesions dorsal surface arms bilateral

58
What else should you think about?

59
Seborrehea Characteristics: Positive family history is common
Seen in all age groups equally May occur on presternal area and mid upper back Stress may increase symptoms Pityrosporum ovale may be causative factor Distinctive Characteristics: Red greasy scaling rash consists of patches and plaques with indistinct margins and an underlying red glazed look to the skin Most commonly located in the hairy areas, nasolabial folds, retroauriclar folds Excoriations from scratching are rare

60
Seborrhea cont. Treatment: Scalp –
try OTC preps first (antidandruff, tar or ketoconazole shampoo) Steroid lotions for very short term use 10% Liquor Carbonis Detergens HS and shampoo in AM with Dawn Detergent Skin - try OTC’s first corticosteroids (mild to moderate potency) and/or ketoconazole topically
 Steroid lotions for very short term use. 10% Liquor Carbonis Detergens HS and shampoo in AM with Dawn Detergent. Skin - try OTC’s first. corticosteroids (mild to moderate potency) and/or ketoconazole topically.")
61
Seborrhea cont. Eye lashes- Warm compresses and gentle debridment
with Q tip Sulfacetamide ophthalmic ointment applied topically ** Areas that become exudative may be treated with potassium permanganate or burrow’s soaks Confused with – atopic dermatitis, eczema, psoriasis, discoid lupus, tinea Biopsy/testing – usually none

62
Seborrhea Distribution

63
What else could this be?

66
Asteatotic Eczema (Xerotic Eczema, “Winter Itch”)
Characteristics: Seen mainly in elderly Worse in the winter Precipitated by excessive washing Treatment: Avoid excessive washing and use of soap Emollients Increase humidity in the environment Topical steroids for a short periods of time

67
Localized Neurodermatitis Cont.
Treatment: Stop the scratching Occlusive steroid dressings esp. at night Lubrication Doxepin ointment and/or po 10-20mg Hydroxyzine at night Intralesional steroid injection Stress management and/or medication Treatment is longterm and may be unsatisfactory Confused with – atopic eczema, psorasis, tinea, seborrhea Biopsy / testing – none usually necessary

68
Localized Neurodermatitis (known as Lichen Chronicus Simplex)
Characterisitcs: Origin often small patch of dermatitis or insect bite starting the itch –scratch- itch cycle Condition unrelated to allergies or family history More common in women Nonseasonal aggravated by stress worse at night may be secondary to atopic eczema, contact dermatitis, lichen planus, psoriasis, or insect bite

69
Localized Neurodermatitis (known as Lichen Chronicus Simplex) CONT.
Distinctive Characteristics: Lesions lichenified or excoriated usually limited to a single patch at hairline of nape of neck or on wrists, ankles, ears, or anal area Not bilateral Llichenification of dark skin develops a “follicular pattern”

70
Localized Neurodermatitis Distribution (known as Lichen Chronicus Simplex)
")
71
What should you think about in this man?

72
TREATMENT

73
Stepped Approach to Treatment of Eczema
Conservative Therapy Education (chronicity, prevention, and trigger id) Use of astringents and emollients/moisturizers OTC products (hydrocortisone, Benadryl, Calamine, etc.) Low to mid potency steroid creams High potency steroid creams Immunomodulators - Elidel and Protopic creams Nontraditional agents PO therapy: antiprurutics, steroids, cyclosporine, methotrexate Coal Tar PUVA therapy (phototherapy)
 Use of astringents and emollients/moisturizers. OTC products (hydrocortisone, Benadryl, Calamine, etc.) Low to mid potency steroid creams. High potency steroid creams. Immunomodulators - Elidel and Protopic creams. Nontraditional agents. PO therapy: antiprurutics, steroids, cyclosporine, methotrexate. Coal Tar. PUVA therapy (phototherapy)")
74
Conservative Therapy

75
Education Chronicity of eczema
Association of other conditions: AR, asthma Vast number of sensitizing chemicals used currently in our soaps, shampoos, detergents, foods, etc. Likelihood of finding a trigger low Detailed sensitizers/triggers (see Pocket Guide to Medications used in Dermatology by Scheman and Severson)
")
76
Patient Resources The Eczema Survival Guide – 30 page guide by the NEASE – the single best general patient medical resource on the internet – sponsored by NIH - National Eczema Society – National Eczema Assoc. for Science and Education - online dermatology atlas from Johns Hopkins Univ.

77
Prevention Checklist Moisturize daily
Wear cotton, avoid wool and tight clothes Take lukewarm showers, using mild soap or nonsoap cleansers Pat dry – do not rub Apply moisturizer within 3 min. to “lock in” moisture Avoid extremes of heat/humidity and perspiration Learn triggers and how to avoid them Keep fingernails short Remove carpets and pets from the home

78
Soaps and Cleansers Any product that removes skin oils (sebum), dirt, other undesirable substances Range from very moisturizing to neutral to very drying “If it is dry, wet it; and if it is wet, dry it” – derm mantra Normal skin pH is ; most soaps are basic and therefore can be irritating Rinsing may be an issue if irritating Choose the appropriate cleanser to match your patient’s skin type (most eczema patients will need hydration of the skin and neutral or acidic pH) Again, see Pocket Guide to Medications used in Dermatology for detailed ingredients of skin products
 Again, see Pocket Guide to Medications used in Dermatology for detailed ingredients of skin products.")
79
Soap Free Cleansers Indications:
Cetaphil Aquanil Aveeno Daily Mositurizer Eucerin Gentle Hydrating Cleanser Lobana Body Shampoo Moisturel pHisoderm Indications: For use in those eczema patients who may be sensitive to one or more of the various potential sensitizers in soaps and shampoos. To cleanse, reduce irritation (if sensitive to soaps), and reduce dryness (thereby increase absorption of other topicals).
, and reduce dryness (thereby increase absorption of other topicals).")
80
Emollients/Moisturizers
Aquaphor Balmex Daily AmLactin Cutemol DML Forte Eucerin Original Hydrisinol Lanolor Indication: To soften and soothe rough, dry skin and increase absorbability of topical medications Directions: Apply as necessary or as prescribed; generally after showering/bathing and pat drying; apply liberally to affected areas Neutrogena Norwegian Formula Lac-Hydrin Aveeno Pen-Kera Curel Lubriderm Advanced Therapy Minerin

81
Astringents Astringents – reduce secretions (by causing contraction of tissues) and are antibacterial Best used in eczema where vesicular or draining lesions are present Acetic Acid 5% (white vinegar) – especially useful in Pseudomonas infections Burow’s Solution (Domeboro and others) Potassium Permanganate
 – especially useful in Pseudomonas infections. Burow’s Solution (Domeboro and others) Potassium Permanganate.")
82
Burow’s Solution (aluminum acetate)
Indication: Used as an astringent wet to dry dressing for relief of inflammatory conditions of the skin such as insect bites, poison ivy, allergy, eczema, and athlete’s foot. Directions: One tablet or one pack per pint of water = 1:40 solution Actions: Collagenase enzyme activity may be inhibited by aluminum acetate solution because of the metal ion and low pH.

83
Burow’s Solution As a compress or wet dressing: Saturate a clean, soft, white cloth in the solution. Gently squeeze and apply loosely to affected area. May cover with dry dressing. Saturate the cloth in solution every 15 to 30 minutes and apply to affected area. Repeat as often as necessary As a soak: Soak affected area in solution for 15 to 30 minutes. Discard solution after each use. Repeat 3 times a day

84
Burow’s Solution Precautions:
Discontinue use if intolerance, irritation, or extension of inflammatory condition being treated occurs. If symptoms persist >7 days, discontinue use and consult physician Do not use plastic or any other impervious material to prevent evaporation Avoid contact with the eyes

85
OTC Therapy

86
OTC Meds Antiinflammatory topicals Hydrocortisone creams, 0.5% to 1%
Antipruritics and others Benadryl (diphenhydramine 25-50mg q6h prn) Calamine Lotion (zinc oxide and ferric oxide used as a mild astringent) Caladryl Lotion (both of above) Burow/s solution
 Calamine Lotion (zinc oxide and ferric oxide used as a mild astringent) Caladryl Lotion (both of above) Burow/s solution.")
87
Prescription Therapy of Eczema

88
Properties of the Ideal Drug (prescription or otc)
(Acronym IDEA) Inexpensive Dosage – once daily or bid or less Effective Adverse effects absent
 Inexpensive. Dosage – once daily or bid or less. Effective. Adverse effects absent.")
89
Steroid Creams

90
Basic Rules of Dermal Absorption
The larger the surface area the formulation is applied to, the greater the absorption Formulations or dressings that increase the hydration of the skin generally improve absorption The greater the amount of rubbing in of the formulation, the greater the absorption The more active inflammation or open vesicles or ulcers present, the greater the absorption The longer the formulation remains in contact with the skin, the greater will be the absorption

91
Steroid Classifications

92
Topical Vehicles Creams: Less greasy and most acceptable to patient
Applies more easily Penetrates skin well Works well in intertriginous and hairy areas Can be drying Have a cooling effect Easy to wash off Lotions: more water content and less viscous than creams Ointments: Petrolatum based Alleviates dryness by prevention of evaporation Removes scales Enables medication to penetrates skin well Water repellant Remains on the skin Occlusive and protective Soothing and lubricating

93
Prescription Topical Steroids Low and Medium Potency
Do consider use in: Allergic/Contact Dermatitis Seborrheic Dermatitis Intertrigo of axillary, crural or inframammary regions Atopic Eczema Neurodermatitis Otic eczema Do not use: Large body areas because of expense, difficulty with application, and question of internal absorption

94
Prescription Topical Steroids High Potency and Fluorinated
Do consider use: With or without occlusive dressing in palmar or plantar atopic dermatitis Localized neurodermatitis Do not use: Face Intertriginous areas ** prolonged use in any area may cause thinning of the skin, telangiectasia, striae

95
Immunomodulators (Topical immunomodulators-TIM’s)
")
96
Elidel Elidel (pimecrolimus) 1% cream Indications:
Short term and repeated courses for mild to moderate eczema in nonimmunocompromised patients greater that 2 years of age in whom the use of alternative conventional treatment is inadvisable or those with are none responsive to conventional treatment. Can be used anywhere on the skin Precautions: Do not use in treatment of infected atopic dermatitis, including eczema herpeticum Patients who develop lymphadenopathy should have a complete evaluation to R/O lymphoma Avoid sun light exposure as sun exposure and use of pimecrolimus shortens time of skin lesion to skin tumor formation in animals Do not use occlusive dressings

97
Elidel (cont’d) Adverse Effects (often resolve after a few days of therapy): Warmth or burning where applied Headache Cold-like symptoms (st, cough, rn) Fever Viral skin infection Dosage: Apply BID Discontinue when symptoms resolved Further evaluation needed if symptoms persist > 6 weeks MOA: Calcineurin inhibitor Cost: 30 grams: $63; 60 grams $117
 Fever. Viral skin infection. Dosage: Apply BID. Discontinue when symptoms resolved. Further evaluation needed if symptoms persist > 6 weeks. MOA: Calcineurin inhibitor. Cost: 30 grams: $63; 60 grams $117.")
98
Protopic Protopic (tacrolimus) adults 0.03% & 0.1% ointment
Indications: Protopic ointment 0.1% for adults only Protopic ointment 0.03% for children age 2 and older Short term and repeated courses of moderate to severe eczema in whom the use of alternative conventional treatment is inadvisable or those who are not responsive to conventional treatment Can be used anywhere on the skin Precautions: Do not use in treatment of infected atopic dermatitis, including eczema herpeticum Patients who develop lymphadenopathy should have a complete evaluation to R/O lymphoma Avoid sunlight, tanning salons, phototherapy (PUVA), as sunlight shortens time of skin lesion to skin tumor formation in animals Do not use occlusive dressings
, as sunlight shortens time of skin lesion to skin tumor formation in animals. Do not use occlusive dressings.")
99
Protopic (cont’d) Adverse reactions ( often resolve after few days of application): Skin stinging and burning (dependent on degree of eczema) Increased skin infections Dosage: Apply BID Discontinue 1 week after symptoms resolved Further evaluation needed if symptoms persist > 6 weeks MOA: Calcineurin inhibitor Cost: 30 grams: $62; 60 grams $130

100
Potential problem with both TIM’s (Elidel and Protopic)
Feb. 15th 2005: the Pediatric Advisory Committee of the FDA met and recommended that a “black box warning” be added to both Elidel and Protopic due to “potential cancer risk” This is due to animal studies where animals swallowed large amounts of both drugs over a long period of time, achieved significant blood levels of the drugs, and developed lymphomas. March 10, 2005: The FDA issued a Public Health Advisory warning the public about potential carcinogenic safety issues involving both TIM’s. The American Academy of Dermatology, the Nat’l. Eczema Assn. for Science and Education (NEASE), and the Inflammatory Skin Disease Institute (ISDI) all have issued statements declaring the FDA action premature and all feel that the drugs are safe when used appropriately There are already websites dedicated to class action litigation against both manufacturers Bottom Line: I would not adivse using in any pediatric patients, or in any patient that can be controlled with less expensive and efficacious therapy.
, and the Inflammatory Skin Disease Institute (ISDI) all have issued statements declaring the FDA action premature and all feel that the drugs are safe when used appropriately. There are already websites dedicated to class action litigation against both manufacturers. Bottom Line: I would not adivse using in any pediatric patients, or in any patient that can be controlled with less expensive and efficacious therapy.")
101
Nontraditional Agents
Problem: these are not deemed safe or effective by the FDA Herbal remedies Licorice as topical gel Guava leaves (as tea) Chinese herbal teas St. John’s wort (as lotion or tea) Probiotics – thought to help relieve inflammation Homeopathic – arsenicum alba and calcara carbonica Hypnosis Acupuncture Gamma linoleic acid oils Evening primrose oil Borage oil
 Chinese herbal teas. St. John’s wort (as lotion or tea) Probiotics – thought to help relieve inflammation. Homeopathic – arsenicum alba and calcara carbonica. Hypnosis. Acupuncture. Gamma linoleic acid oils. Evening primrose oil. Borage oil.")
102
PO Prescription Drug Therapy
Antipruritics Hydroxyzine 10-25mg q6h prn itching Doxepin 10-25mg q12-24h prn itching (off label) also can be compounded as a cream) Oral Steroids May give in tapering short courses for selected episodes of acute and/or severe eczema Effective, inexpensive, qd dosing, few side effects in most people with short term use Cyclosporine – reserve for specialty use Methotrexate – reserve for specialty use
 also can be compounded as a cream) Oral Steroids. May give in tapering short courses for selected episodes of acute and/or severe eczema. Effective, inexpensive, qd dosing, few side effects in most people with short term use. Cyclosporine – reserve for specialty use. Methotrexate – reserve for specialty use.")
103
Coal Tar Preparations Tegrin cream and lotion Medotar ointment
PsoriGel gel Polytar and Tegrin soaps Tegrin, T/Gel, and other shampoos Indication: to relieve and control itching, and flaking skin associated with psoriasis and seborrhea as well as eczema Directions: Depending on product 1-4 times daily

104
Coal Tar Preparations (cont’d)
Contraindications: Hypersensitivity Precautions: Do not use on broken skin, genital or rectal area except on the advise of your health care provider. Photosensitivity x 24hr after application May stain light colored hair Warning: High concentrations of some chemicals in coal tar may cause cancer. Concentrations of 0.5% to 5% appear to be safe.

105
PUVA Therapy Indications: Psoriasis, eczema, pruritic rashes of other causes Consists of PO psoralen (photosensitizing agent) followed by UVA phototherapy Must avoid sunlight for 24h after po psoralen Sessions are 3d/wk, may be from sessions, increasing in duration Side effects are redness, burning, occasional nausea Litigation very high in some states
 followed by UVA phototherapy. Must avoid sunlight for 24h after po psoralen. Sessions are 3d/wk, may be from sessions, increasing in duration. Side effects are redness, burning, occasional nausea. Litigation very high in some states.")
106
Summary of Treatment Conservative Therapy
Education (chronicity, prevention, and trigger id) Use of astringents and emollients/moisturizers OTC products (hydrocortisone, Benadryl, Calamine, etc.) Low to mid potency steroid creams High potency steroid creams Immunomodulators - Elidel and Protopic creams Nontraditional agents PO therapy: antiprurutics, steroids, cyclosporine, methotrexate Coal Tar PUVA therapy (phototherapy)
 Use of astringents and emollients/moisturizers. OTC products (hydrocortisone, Benadryl, Calamine, etc.) Low to mid potency steroid creams. High potency steroid creams. Immunomodulators - Elidel and Protopic creams. Nontraditional agents. PO therapy: antiprurutics, steroids, cyclosporine, methotrexate. Coal Tar. PUVA therapy (phototherapy)")
107
Midlevel Provider’s Role in theTreatment of Eczema
Identification Treatment Education

108
Identify Acute-Chronic; Allergic,Atopic, Toxic/Irritant

117
Extra Credit!!!!!

118
The End

Similar presentations

















 Prevent insensible water.>")









