Download presentation
Presentation is loading. Please wait.

1
An Overview in Mass Casualty Incident (MCI) Operations and Triage
MASCAL An Overview in Mass Casualty Incident (MCI) Operations and Triage
 Operations and Triage.")
2
Purpose To familiarize personnel with: the triage process
the organization and conduct of MASCAL Operations Purpose

3
MASS-CASUALTY SITUATION: used to describe a situation in which the number of casualties exceeds the hospital's capabilities to provide medical care. Maybe one patient maybe 20…question is have we exceeded our ability to provide medical care MASCAL

5
Possible Scenarios Accident War Terrorism Epidemic Toxin
Environmental Extremes Possible Scenarios

6
Situational Factors Numbers of Casualties Location of Casualties Time
of day to medical facility (Distance) Transportation Vehicles Lines of Communication Medical Resources Personnel Facilities Distance Situational Factors
 Transportation. Vehicles. Lines of Communication. Medical Resources. Personnel. Facilities. Distance. Situational Factors.")
7
Hospital Disaster Plan Considerations
Alert Process Activation Levels Notification Procedures Emergency Privileging Process Operations Triage Areas Marking Techniques Standing Orders Layout/Patient Flow at Medical Facility Supplies Backup Transportation Organization of Health Care Providers Echelons of Providers Ancillary Personnel Litter Bearers Drivers Traffic controllers Security Chaplains Red Cross Housekeeping Runners/Messengers Patient Administrators Communications Command and Control Medical Resources Hospital Disaster Plan Considerations

8
Conduct of MASCAL Initial Response
Notification/Alert First Response On-Site Activities Safety Security Traffic Management Communications Personnel Management Triage Medical Care Medical Facility Preparation Transportation Conduct of MASCAL Initial Response

9
Notification (Example)
MCI (Mass Casualty Incident) reporting form located on 121st website. The IC (Incident Commander, the Hospital Commander) is notified and initiates the MASCAL plan. The Deputy Commander for Administration (DCA) activates the EOC (Emergency Operations Center (S3) ). There is a 24 hour on-call NCO for this center. Cell # Units/departments alert personnel via own department policies (alert rosters). Notification (Example)
 reporting form located on 121st website. The IC (Incident Commander, the Hospital Commander) is notified and initiates the MASCAL plan. The Deputy Commander for Administration (DCA) activates the EOC (Emergency Operations Center (S3) ). There is a 24 hour on-call NCO for this center. Cell # Units/departments alert personnel via own department policies (alert rosters). Notification (Example)")
10
Incident Commander (Example)
Is the Hospital Commander Initiates and terminates the MASCAL Plan. Designates the Level of Response to the MASCAL Notifies higher headquarters and keeps higher headquarters informed of MASCAL status. Prioritizes utilization of all assets. Determines patient holding and evacuation criteria. Incident Commander (Example)
")
11
Deputy Commander for Administration (DCA) (Example)
Coordinates administrative staff support to manpower pool operations Activates the USAMEDDAC-Korea EOC Acting IC in the absence of the Commander Observes MASCAL response Deputy Commander for Administration (DCA) (Example)
 (Example)")
12
Deputy Commander for Clinical Services (DCCS) (Example)
Designates surgeons for triage and other duties. Reviews MASCAL triage decisions with Chief Nurse Assists training of EMT personnel in triage. Assigns physicians to duty positions. Deputy Commander for Clinical Services (DCCS) (Example)
 (Example)")
13
Deputy Commander for Nursing (DCN) (Example)
Controls nurse corps workforce. Observes MASCAL response; initiates on-the-spot correction of the patient care process not foreseen in planning and rehearsal. Monitors patient flow and assigns nurses to appropriate sections as required. Deputy Commander for Nursing (DCN) (Example)
 (Example)")
14
Command Sergeant Major (CSM) (Example)
In conjunction with the Chief Nurse, and the DCCS, determines treatment areas and patient flow Designates NCO to act as MASCAL site manager Command Sergeant Major (CSM) (Example)
 (Example)")
15
Chief Ward Master (Example)
Reviews MASCAL procedures for adjustments Briefs hospital staff on MASCAL procedures Chief Ward Master (Example)
")
16
Manpower Pool NCOIC (non-clinical)
Directs all personnel reporting to the Manpower Pool. Reports directly to the Command Sergeant Major (CSM). Organizes personnel into litter teams. As needed, assigns personnel to act as: Runners Vehicle and personnel guides Security teams Manpower Pool NCOIC (non-clinical)
. Organizes personnel into litter teams. As needed, assigns personnel to act as: Runners. Vehicle and personnel guides. Security teams. Manpower Pool NCOIC (non-clinical)")
17
Hospital Non-Clinical Staff
Personnel Officer (S1): Manages Personnel/Manpower pool Intelligence Officer (S2): Identifies possible Nuclear, Biological, Radiological, and Chemical (CBRN) threats and briefs hospital staff Plans and Operations Officer (S3): Serves in the Emergency Operations Center (EOC) as required by the Incident Commander (IC) Logistics Officer (S4): Anticipates supply requirements and notifies command of critical supply state Communications Officer (S6): Establishes and Monitors Communications Hospital Non-Clinical Staff
: Manages Personnel/Manpower pool. Intelligence Officer (S2): Identifies possible Nuclear, Biological, Radiological, and Chemical (CBRN) threats and briefs hospital staff. Plans and Operations Officer (S3): Serves in the Emergency Operations Center (EOC) as required by the Incident Commander (IC) Logistics Officer (S4): Anticipates supply requirements and notifies command of critical supply state. Communications Officer (S6): Establishes and Monitors Communications. Hospital Non-Clinical Staff.")
18
Patient Administrative Division (PAD)
Establishes the Patient Identification process outside the Emergency Department. Processes casualties for admission; collects patients' funds and valuables at the Triage Point. Discharges those current in-patients selected by ward doctors to make additional beds available; transfers patients as required. Provides bed and patient status reports to the EOC every thirty minutes. Provides updated patient rosters to the command Provide staffing to the Emergency Operations Center (as required or as per Standard Operating Procedure) Patient Administrative Division (PAD)
 Patient Administrative Division (PAD)")
19
Provides augmentation personnel to the Emergency Department as required.
Department of Surgery

20
Department of Medicine
Receives and treats casualties in the Acute Care Clinic (ACC) requiring MINIMAL treatment; obtains personnel support for the ACC from the Mass Casualty Manpower Center, should the workload indicate. Provides augmentation personnel to the Emergency Department as required. Department of Medicine
 requiring MINIMAL treatment; obtains personnel support for the ACC from the Mass Casualty Manpower Center, should the workload indicate. Provides augmentation personnel to the Emergency Department as required. Department of Medicine.")
21
Lab Services and Pathology
Provides emergency laboratory services for the treatment of casualties, as requested. Expands emergency blood bank services, if required. Implements emergency procedures for handling remains. Provide one staff pathologist to the Emergency Department, if required. Lab Services and Pathology

22
Department of Pharmacy
As required delivers drugs and supplies to the Emergency Department. As required issues required drugs and supplies to inpatient wards. Provide staffing to Emergency Operations Center (EOC) as required. Department of Pharmacy
 as required. Department of Pharmacy.")
23
Department of Radiology
Positions one mobile X-ray unit in the Emergency Department immediately upon announcement of a MASCAL. Determines, with the Chief of Emergency Medicine Service, the requirement for additional mobile X-ray units in the Emergency Department to support mass casualty operations. Provides staff radiologist to the Emergency Department. Implements procedures to provide wet readings, if required. Department of Radiology

24
Supervises the reception and treatment of casualties.
Uses augmenting personnel provided by other departments, services and divisions and activates and manages the expanded Emergency Department. Provide staffing to EOC as required. Emergency Department

26
Emergency Department (ED) Considerations after Notification
Alert the on-call team Analyze incoming reports Rapid brief of team Organize available personnel Triage Treatment teams Position personnel Check communications Check readiness of ancillary staff EKG, X-Ray, Lab, Blood Bank, etc. Check emergency equipment and supplies Check readiness of OR/surgeons Review SOP's Safety, safety, safety INCLUDING BLOOD AND BODY FLUID PRECAUTIONS Emergency Department (ED) Considerations after Notification
 Considerations after Notification.")
27
DO THE MOST FOR THE MOST Triage

28
Principles of Triage Rapid assessment of every patient Safety
Experienced Triage Officer Triage "Captains" do not give medical care Speed, with Thoroughness Impassionate Use simple criteria, without need for equipment Return the Most to Duty Principles of Triage

29
Problems Humbling Second-Guessing Errors Imprecise Process
Scoring Systems not any better than Experience, Knowledge, Instinct Triage is at multiple levels-- everyone needs training Problems

30
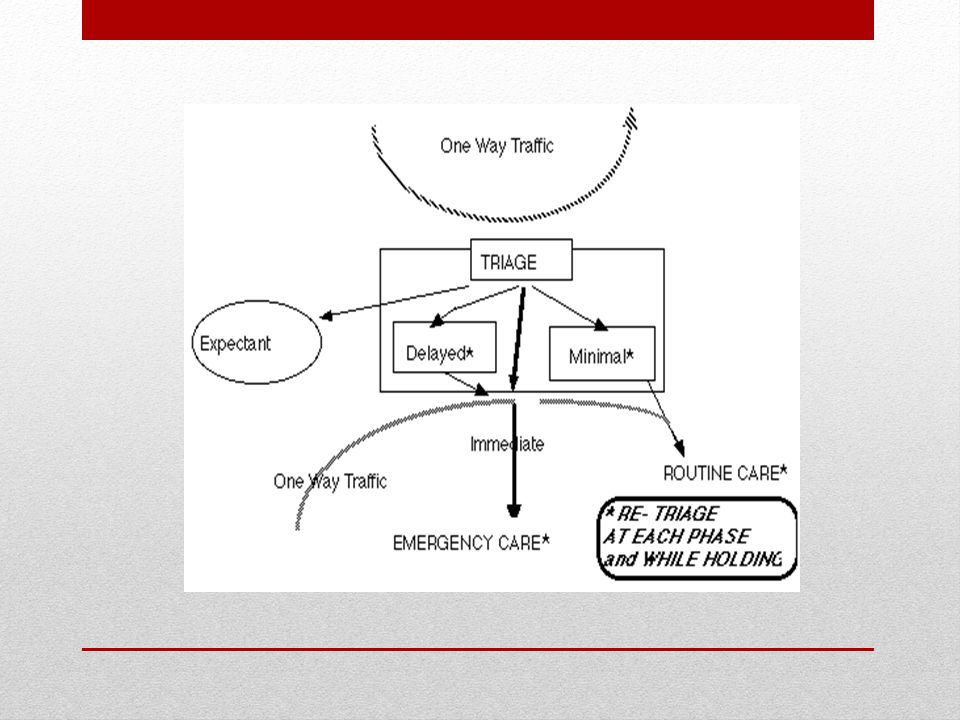
I-immediate: This group includes those soldiers requiring life -saving surgery.
Procedure should not be time consuming Casualties should have high chance of survival D-delayed: those wounded who are badly in need of time consuming surgery but whose general condition permits delay in intervention without unduly endangering life. Will require sustaining treatment IDME or DIME

31
M-minimal or “walking wounded”: These casualties have minor injuries and can usually care for themselves with self-aid or “buddy aid”. These casualties should still be employed for mission requirements (litter bearers runners, scene security). E-expectant: those whose wounds are so extensive that even if they were the sole casualty and had the benefit of optimal medical resource application, their survival would be unlikely IDME or DIME
. E-expectant: those whose wounds are so extensive that even if they were the sole casualty and had the benefit of optimal medical resource application, their survival would be unlikely. IDME or DIME.")
32
Examples Immediate: Delayed: Respiratory obstruction
Unstable casualties with chest or abdominal injuries Emergency amputation Delayed: Large muscle wounds Fractures of major bones Intra-abdominal and or thoracic wounds Burns < 50 % Total body surface area ( TBSA) Examples
 Examples.")
33
Examples Minimal: Expectant: Minor lacerations and or abrasion
Minor fractures of small bones Minor burns Expectant: Unresponsive patients with penetrating head wounds High spinal cord injuries Mutilating explosive wounds Partial and full thickness burns > 60% TBSA Profound shock Exhibiting agonal respirations Examples

34
What is the Category?

35
RPG to R Knee

37
Triage Officer Should be experienced Leader
Not involved in patient care "Chance favors the prepared mind." Louis Pasteur Triage Officer

38
Remember Triage is: Continuous (for each victim)
Repeated (for groups of victims at each site) MASCAL Site Treatment Areas Entry Exit/Evacuation Remember
 MASCAL Site. Treatment Areas. Entry. Exit/Evacuation. Remember.")
39
Organization of the Staging/Triage Area
Primary Rescuers Triage Officer (Senior Medical Officer on scene) Communications Liaison Traffic Control Personnel Control Security Officer Site Manager Organization of the Staging/Triage Area
 Communications Liaison. Traffic Control. Personnel Control. Security Officer. Site Manager. Organization of the Staging/Triage Area.")
43
Arrival of Patients Check your pulse Exhibit calm demeanor
Control the flow of communication Control the flow of people Assess number of casualties Arrival of Patients

44
Preparation and Training
Develop Triage System Analyze patient Flow Analyze communication flow Train Staff in triage monitoring treatment Reporting/communication/documentation Analyze/Train pre-hospital team Talk thru Walk Thru Drill, Drill, Drill Feedback/After Action Discussions Study Trauma Medical Threat Intelligence Endemic Diseases Enemy Weapons Preparation and Training

45
Preparation and Training
Clinical Knowledge Trauma assessment and treatment Triage Skills MASCAL Process Organization Command, Control, Communications Logistics Exercises Partial Complete Mental/Spiritual Preparedness Preparation and Training

46
Debriefing and After Action Review
To analyze the good and the bad Emotional venting & support Make immediate reports Make corrections quickly Debriefing and After Action Review

47
"To improve is to change; to be perfect is to change often."
--Winston Churchill

48
Questions?

Similar presentations
























 program helps train people to be better prepared to respond to emergency.>")