Download presentation
Presentation is loading. Please wait.

1
Tools in the Battle Against Smoking and Tobacco
3-C CON, AHMEDABAD, FEBRUARY 2011 Chaim Lotan, MD Akshardham Temple, Gandhinagar, Ahmedabad Heart Institute, Hadassah Hospital, Jerusalem, ISRAEL

2
Smoking and coronary artery disease
History Epidemiology CV Effects Importance of Cessation

4
Cigarette Smoking as a Risk Factor for Cardiovascular Disease
was recognized in the results of the Framingham Heart Study in 1960

5
Smoking kills more people each year than
alcohol cocaine crack heroin homicide suicide car accidents fires AIDS C O M B I N ED!!!

6
New Concepts of Management to Prevent Hazardous Consequences
Smoking Cessation: New Concepts of Management to Prevent Hazardous Consequences

7
Smoking and coronary artery disease
History Epidemiology CV Effects Importance of Cessation

8
Global Cigarette Consumption
WHO World Health Report .Tobacco Atlas

9
Section 2: The Hazards of Smoking

10
8 smokers die every minute
Facts & Numbers 1.25 billion smokers Worldwide 30 million smokers added every year 84% of smokers live in developing countries Africa & Middle East (17% of World’s population) accounts for 7% of World’s total cigarette consumption 8 smokers die every minute One-third of the world's adult population are smokers (57% of these are men, 43% are women) and each year, tobacco causes 3.5 million deaths a year, or about 10,000 deaths each day. It is predicted that in 20 years this yearly death rate from tobacco use will be more than 10 million people. Here are some worldwide alarming statistics stated by the World Heart Foundation: 1.25 billion smokers Worldwide 30 million new smokers are added every year 84% of smokers live in developing countries. Africa & Middle East, representing 17% of World’s population, accounts for 7% of World’s total cigarette consumption. 8 smokers die every minute. The picture on the right is taken from the 1996 Guinness Book of Records. It is for Stefan Sigmond, who is a 29 years old man, from Cluj in Transylvania. Stefan set a record in Bucharest on January 31st, 1996, when he smoked 800 filter-tipped western cigarettes in less than 6 minutes through a special wheel-like device, breaking his 1995 record of 750. In 1995 he ate 29 boiled eggs in 4 minutes and – separately – jumped into a lake from a 135 feet (41 meters)-high platform. He will not, however, appear in the Guinness Book of Records which now discourages gluttony and fool hardiness. AP; R 2 Feb Voute J, World Heart Foundation
 accounts for 7% of World’s total cigarette consumption. 8 smokers die every minute. One-third of the world s adult population are smokers (57% of these are men, 43% are women) and each year, tobacco causes 3.5 million deaths a year, or about 10,000 deaths each day. It is predicted that in 20 years this yearly death rate from tobacco use will be more than 10 million people. Here are some worldwide alarming statistics stated by the World Heart Foundation: 1.25 billion smokers Worldwide. 30 million new smokers are added every year. 84% of smokers live in developing countries. Africa & Middle East, representing 17% of World’s population, accounts for 7% of World’s total cigarette consumption. 8 smokers die every minute. The picture on the right is taken from the 1996 Guinness Book of Records. It is for Stefan Sigmond, who is a 29 years old man, from Cluj in Transylvania. Stefan set a record in Bucharest on January 31st, 1996, when he smoked 800 filter-tipped western cigarettes in less than 6 minutes through a special wheel-like device, breaking his 1995 record of 750. In 1995 he ate 29 boiled eggs in 4 minutes and – separately – jumped into a lake from a 135 feet (41 meters)-high platform. He will not, however, appear in the Guinness Book of Records which now discourages gluttony and fool hardiness. AP; R 2 Feb Voute J, World Heart Foundation.")
11
Tobacco – a major health problem now and for the future
A startling fact to set the scene. Tobacco is a major public health issue globally and specifically within developing countries WHO estimates that by 2030 over 80% of tobacco related deaths will be in the developing world

12
One out of two lifelong adult smokers will die from a smoking related disease.
CDC. Projected smoking-related deaths among youth – United States. MMWR 1996;45(44):
:")
13
Gender-specific Smoking Prevalence Across the World
1.25 billion smokers worldwide1 Sweden 17% 18% Iceland 25% 20% Canada 22% 17% Russian Federation 60% 16% Belarus 53% 7% France 30% 21% Germany 37% 28% US 24% 19% Portugal 33% 10% China 67% 2% Spain 39% 25% Italy 33% 17% Iran 22% 2% Mexico 13% 5% Egypt 45% 12% India 47% 17% Philippines 41% 8% Key Points Worldwide, there are marked difference in smoking prevalence between men and women Smoking prevalence is much lower in women (vs men) in South Africa, the Philippines, China, Iran, and Portugal Smoking prevalence is only slightly lower in women (vs men) in the US, Canada, Australia, and Iceland Overall, the prevalence of smoking in men is declining Smoking prevalence in women is declining is some countries (US, UK, Australia, and Canada) However, smoking prevalence in women is either remaining constant or increasing in several Southern, Central, and Eastern European countries Reference 1. Mackay J, Eriksen M, Shafey O. The Tobacco Atlas. Second Ed. American Cancer Society Myriad Editions Limited. Atlanta, Georgia, Also available online at: Brazil 22% 14% Kenya 21% 1% Men Women Australia 19% 16% South Africa 23% 8% Chile 48% 37% Mackay J, Eriksen M. The Tobacco Atlas. Second Ed. American Cancer Society, 2006.
 in South Africa, the Philippines, China, Iran, and Portugal. Smoking prevalence is only slightly lower in women (vs men) in the US, Canada, Australia, and Iceland. Overall, the prevalence of smoking in men is declining. Smoking prevalence in women is declining is some countries (US, UK, Australia, and Canada) However, smoking prevalence in women is either remaining constant or increasing in several Southern, Central, and Eastern European countries. Reference. 1. Mackay J, Eriksen M, Shafey O. The Tobacco Atlas. Second Ed. American Cancer Society Myriad Editions Limited. Atlanta, Georgia, Also available online at: Brazil. 22% 14% Kenya. 21% 1% Men. Women. Australia. 19% 16% South Africa. 23% 8% Chile. 48% 37% Mackay J, Eriksen M. The Tobacco Atlas. Second Ed. American Cancer Society,")
14
4 year-old addict to smoking in Indonesia

15
Smoking and coronary artery disease
History Epidemiology CV Effects Importance of Cessation

16
Smoking: Leading Preventable Cause of Disease and Death1
Cancer Lung (#1) Leukemia (AML, ALL, CLL)2-4 Oral cavity/pharynx Laryngeal Esophageal Stomach Pancreatic Kidney Bladder Cervical Other Adverse surgical outcomes/wound healing Hip fractures Low-bone density Cataract Peptic ulcer disease in Helicobacter pylori-positive patients Reproductive Low-birth weight Pregnancy complications Reduced fertility SIDS Cardiovascular Ischemic heart disease (#2) Stroke – vascular dementia5 Peripheral vascular disease6 Abdominal aortic aneurysm Respiratory COPD (#3) Pneumonia Poor asthma control Key Points Smoking has been causally linked to a host of cardiovascular, respiratory, reproductive, and other conditions, as well as many types of cancer These diseases affect smokers of all ages, but … Increases in a smoker’s age correlate with increased frequency of smoking-related diseases Background In 2004, the US Surgeon General published a report on the health effects of active smoking1, focusing specifically on the evidence for a causal relationship between smoking and disease and death. According to the research summarised in the report, many serious conditions are caused by smoking, including cardiovascular, respiratory, reproductive, and other conditions, as well as cancer affecting diverse areas and organs of the body. In addition to the widely known consequences of lung cancer and respiratory disease, smoking has been causally linked to such diverse morbidities as low-bone density, nuclear cataract, bladder cancer, and reduced fertility. Other studies have linked smoking to vascular dementia5 and peripheral arterial disease.7 These conditions can affect young and middle-aged smokers and, in general, as a smoker’s age increases, the frequency of smoking-caused diseases rises. References Surgeon General’s Report. The Health Consequences of Smoking; 2004. Sandler DP, et al. J Natl Cancer Inst. 1993;85: Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5: Miligi L, et al. Am J Ind Med. 1999;36:60-69. Roman GC. Cerebrovasc Dis. 2005;20: Willigendael EM, et al. J Vasc Surg. 2004;40: AML = acute myeloid leukemia; ALL = acute lymphocytic leukemia; CLL = chronic lymphocytic leukemia; COPD = chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome. Surgeon General’s Report. The Health Consequences of Smoking; 2004. Sandler DP, et al. J Natl Cancer Inst. 1993;85: Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5: Miligi L, et al. Am J Ind Med. 1999;36:60-69. Roman GC. Cerebrovasc Dis. 2005;20: Willigendael EM, et al. J Vasc Surg. 2004;40:
 Leukemia (AML, ALL, CLL)2-4. Oral cavity/pharynx. Laryngeal. Esophageal. Stomach. Pancreatic. Kidney. Bladder. Cervical. Other. Adverse surgical outcomes/wound healing. Hip fractures. Low-bone density. Cataract. Peptic ulcer disease in Helicobacter pylori-positive patients. Reproductive. Low-birth weight. Pregnancy complications. Reduced fertility. SIDS. Cardiovascular. Ischemic heart disease (#2) Stroke – vascular dementia5. Peripheral vascular disease6. Abdominal aortic aneurysm. Respiratory. COPD (#3) Pneumonia. Poor asthma control. Key Points. Smoking has been causally linked to a host of cardiovascular, respiratory, reproductive, and other conditions, as well as many types of cancer. These diseases affect smokers of all ages, but … Increases in a smoker’s age correlate with increased frequency of smoking-related diseases. Background. In 2004, the US Surgeon General published a report on the health effects of active smoking1, focusing specifically on the evidence for a causal relationship between smoking and disease and death. According to the research summarised in the report, many serious conditions are caused by smoking, including cardiovascular, respiratory, reproductive, and other conditions, as well as cancer affecting diverse areas and organs of the body. In addition to the widely known consequences of lung cancer and respiratory disease, smoking has been causally linked to such diverse morbidities as low-bone density, nuclear cataract, bladder cancer, and reduced fertility. Other studies have linked smoking to vascular dementia5 and peripheral arterial disease.7 These conditions can affect young and middle-aged smokers and, in general, as a smoker’s age increases, the frequency of smoking-caused diseases rises. References. Surgeon General’s Report. The Health Consequences of Smoking; Sandler DP, et al. J Natl Cancer Inst. 1993;85: Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5: Miligi L, et al. Am J Ind Med. 1999;36: Roman GC. Cerebrovasc Dis. 2005;20: Willigendael EM, et al. J Vasc Surg. 2004;40: AML = acute myeloid leukemia; ALL = acute lymphocytic leukemia; CLL = chronic lymphocytic leukemia; COPD = chronic obstructive pulmonary disease; SIDS = sudden infant death syndrome. Surgeon General’s Report. The Health Consequences of Smoking; Sandler DP, et al. J Natl Cancer Inst. 1993;85: Crane MM, et al. Cancer Epidemiol Biomarkers Prev. 1996;5: Miligi L, et al. Am J Ind Med. 1999;36: Roman GC. Cerebrovasc Dis. 2005;20: Willigendael EM, et al. J Vasc Surg. 2004;40:")
17
Published 2004 The INTERHEART Study
Finding: Nine potentially modifiable risk factors are strongly associated with AMI worldwide

18
INTERHEART: Smoking and MI
Odds of myocardial infarction 2 4 8 16 OR (99% CI) > #cigarettes smoked per day
 >40 #cigarettes smoked per day.")
19
Risk of AMI associated with Risk Factors in the Overall Population
Controls % Cases % Odds ratio PAR(99%)CI ApoB/ApoA1(5vs1) 20.0 33.5 3.87 ± 0.5 541. ± 4.5 Current smoking 26.76 45.15 2.95 ± 0.2 C+Former smoking 48.12 65.19 2.27 ± 0.4 36.4 ± 2.6 Diabetes 7.52 18.45 3.08 ± 0.3 12.3 ± 0.8 Hypertension 21.91 39.02 2.48 ± 0.2 23.4 ± 1.7 Abd obesity (3vs1) 33.32 46.31 2.24 ± 0.2 33.7 ± 3.6 All psychosocial - 2.51 ± 0.4 28.8 ± 6.8 Veg&fruit daily 42.36 35.79 0.70 ± 0.1 12.9 ± 3.7 Exercise 19.28 14.27 0.72 ± 0.1 25.5 ± 5.4 Alcohol intake 24.45 24.01 0.79 ± 0.1 13.9 ± 4.6 COMBINED (90-185) 90.4 ± 2.3
CI. ApoB/ApoA1(5vs1) ± ± 4.5. Current smoking ± 0.2. C+Former smoking ± ± 2.6. Diabetes ± ± 0.8. Hypertension ± ± 1.7. Abd obesity (3vs1) ± ± 3.6. All psychosocial ± ± 6.8. Veg&fruit daily ± ± 3.7. Exercise ± ± 5.4. Alcohol intake ± ± 4.6. COMBINED (90-185) 90.4 ± 2.3.")
20
Cardiovascular Risk Factors
8422 Men Age Followed for 72,011 person-years Smoking > 1 ppd Weight > 129% ideal vs < 112% Cholesterol > 268 vs < 219 Systolic BP > 150 vs < 130 Diastolic BP > 94 vs < 80 Relative Risk of Major Coronary Events There are also interactions between risk factors. The Pooling Project Research Group. J Chron Dis 1978;31:

21
WHO top ten causes of death3
Smoking Is Related To 5 of the Top 10 Leading Causes of Death Worldwide1 1 in 10 adult deaths are smoking-related2 500,000,000 people alive today will die from smoking-related causes2 WHO top ten causes of death3 Smoking has been found to be causally related to 5 of the top 10 leading causes of death worldwide. These 5– Ischemic Heart Disease, Cerebrovascular disease, COPD, Lung Cancer, Stomach Cancer – are highlighted in orange in the graph above. Note – the graph displays overall numbers of deaths, which includes but is not limited to those that are directly attributable to smoking. References US Department of Health and Human Services. The Health Consequences of Smoking. A Report of the Surgeon General. Atlanta, Ga: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004. The World Bank Curbing the epidemic: governments and the economics of tobacco control. Washington, D.C. World Health Organization. World Health Report: 2003: Shaping the Future. Causes Related to Smoking 1. Surgeon General’s Report, World Bank, World Health Organization, 2003.

22
How does smoking induce ACS ?
Platelet Viscosity function Endothelial function Coagulation Collagen (PAI-1) Macrophages Inflammation (hs-CRP, cytokine, chemokine) MMPs Smooth LDL-C muscle cells HDL-C TG
 Macrophages. Inflammation. (hs-CRP, cytokine, chemokine) MMPs. Smooth. LDL-C. muscle cells. HDL-C. TG.")
23
LUNGS

24
Role of AMI due to tobacco in India
N=300 AMI, 300 Controls Pais P, Fay MP, Yusuf S Indian Heart J 2001; 53:731-5

26
Tobacco associated mortality in Mumbai (Bombay) India
Tobacco associated mortality in Mumbai (Bombay) India. Results of the Bombay Cohort Study Gupta PC, Pednekar MS, Parkin DM, Sankaranarayanan R Background Little is known about the excess mortality from forms of tobacco use other than cigarette smoking that are widely prevalent in India, such as bidi smoking and the various forms of smokeless tobacco use. We report on absolute and relative risks of mortality among various kinds of ever tobacco users vs never-users in the city of Mumbai, India. (n=99570) Results The adjusted relative risk was 1.37 (95% CI 1.23–1.53) for (men) cigarette smokers and 1.64 (95% CI 1.47–1.81) for bidi smokers, with a significant dose–response relationship for number of bidis or cigarettes smoked. Women were essentially smokeless tobacco users; the adjusted relative risk was 1.25 (95% CI 1.15–1.35). Conclusions Bidi is no less hazardous than cigarette smoking, and smokeless tobacco use may also result in significantly increased mortality. Intl J Epidemiol 2005;43(6):
 India. Results of the Bombay Cohort Study. Gupta PC, Pednekar MS, Parkin DM, Sankaranarayanan R. Background Little is known about the excess mortality from forms of tobacco use other than cigarette smoking that are widely prevalent in India, such as bidi smoking and the various forms of smokeless tobacco use. We report on absolute and relative risks of mortality among various kinds of ever tobacco users vs never-users in the city of Mumbai, India. (n=99570) Results The adjusted relative risk was 1.37 (95% CI 1.23–1.53) for (men) cigarette smokers and 1.64 (95% CI 1.47–1.81) for bidi smokers, with a significant dose–response relationship for number of bidis or cigarettes smoked. Women were essentially smokeless tobacco users; the adjusted relative risk was 1.25 (95% CI 1.15–1.35). Conclusions Bidi is no less hazardous than cigarette smoking, and smokeless tobacco use may also result in significantly increased mortality. Intl J Epidemiol 2005;43(6):")
27
Smokeless tobacco and health in India and South Asia
Prakash C. GUPTA, Cecily S. RAY Abstract: South Asia is a major producer and net exporter of tobacco. Over one-third of tobacco consumed regionally is smokeless. Traditional forms like betel quid, tobacco with lime and tobacco tooth powder are commonly used and the use of new products is increasing, not only among men but also among children, teenagers, women of reproductive age, medical and dental students and in the South Asian diaspora. Smokeless tobacco users studied prospectively in India had age-adjusted relative risks for premature mortality of 1.2–1.96 (men) and 1.3 (women). Current male chewers of betel quid with tobacco in case-control studies in India had relative risks of oral cancer varying between 1.8–5.8 and relative risks for oesophageal cancer of 2.1–3.2. Oral submucous fibrosis is increasing due to the use of processed areca nut products, many containing tobacco. Pregnant women in India who used smokeless tobacco have a threefold increased risk of stillbirth and a two- to threefold increased risk of having a low birthweight infant. In recent years, several states in India have banned the sale, manufacture and storage of gutka, a smokeless tobacco product containing areca nut. In May 2003 in India, the Tobacco Products Bill 2001 was enacted to regulate the promotion and sale of all tobacco products. In two large-scale educational interventions in India, sizable proportions of tobacco users quit during 5–10 years of follow-up and incidence rates of oral leukoplakia measured in one study fell in the intervention cohort. Tobacco education must be imparted through schools, existing government health programmes and hospital outreach programmes. Respirology 2003;8(4):419-31
 and 1.3 (women). Current male chewers of betel quid with tobacco in case-control studies in India had relative risks of oral cancer varying between 1.8–5.8 and relative risks for oesophageal cancer of 2.1–3.2. Oral submucous fibrosis is increasing due to the use of processed areca nut products, many containing tobacco. Pregnant women in India who used smokeless tobacco have a threefold increased risk of stillbirth and a two- to threefold increased risk of having a low birthweight infant. In recent years, several states in India have banned the sale, manufacture and storage of gutka, a smokeless tobacco product containing areca nut. In May 2003 in India, the Tobacco Products Bill 2001 was enacted to regulate the promotion and sale of all tobacco products. In two large-scale educational interventions in India, sizable proportions of tobacco users quit during 5–10 years of follow-up and incidence rates of oral leukoplakia measured in one study fell in the intervention cohort. Tobacco education must be imparted through schools, existing government health programmes and hospital outreach programmes. Respirology 2003;8(4):")
28
Tobacco consumption is a major source of mortality and morbidity in India.
Studies have shown contradictory results regarding smokeless tobacco use as a cardiovascular risk factor, but many show conclusive connection. 2003 Study of adults males in a rural village in Haryana, northern India (chosen randomly)
")
29
Prevalence of tobacco use in study population (N=443):
Non-user of tobacco % Smokeless tobacco user (exclusive) 21% Smoker of tobacco (exclusive) 33% Both smoker and smokeless tobacco user 19.4% Exclusive ST User N=93 (21%) Non User of tobacco N=118 (26.6%) P value Mean body weight (kg) 51.8 ±10.4 53.2 ±12.5 0.386 Family history of HTN 5.4% (n=5) 6.77% (n=8) 0.779 Regular exercise 12.9% (n=12) 11.8% (n=14) 0.835 Mean systolic BP (mmHg) 139.2 ±17.4 135.7 ±18.8 0.16 Mean diastolic BP (mmHg) 86.8 ±11.5 82.6 ±11.5 0.01 Systolic HTN prevalence 43% (n=40) 36.4% (n=43) 0.39 Diastolic HTN prevalence 40.9% (n=38) 22.9% (n=27) 0.0018 Conclusion: Smokeless tobacco consumption is associated in this population with increased prevalence of high blood pressure, which is an indicator of increased disposition to major adverse cardiac events. Pandey A etal. Tobacco Induced Diseases 2009; 5:15
 21% Smoker of tobacco (exclusive) 33% Both smoker and smokeless tobacco user 19.4% Exclusive ST User N=93 (21%) Non User of tobacco N=118 (26.6%) P value. Mean body weight (kg) 51.8 ± ± Family history of HTN. 5.4% (n=5) 6.77% (n=8) Regular exercise. 12.9% (n=12) 11.8% (n=14) Mean systolic BP (mmHg) ± ± Mean diastolic BP (mmHg) 86.8 ± ± Systolic HTN prevalence. 43% (n=40) 36.4% (n=43) Diastolic HTN prevalence. 40.9% (n=38) 22.9% (n=27) Conclusion: Smokeless tobacco consumption is associated in this population with increased prevalence of high blood pressure, which is an indicator of increased disposition to major adverse cardiac events. Pandey A etal. Tobacco Induced Diseases 2009; 5:15.")
30
smokeless tobacco With smoke-free laws, smokeless tobacco (ST) products are being marketed as smoking substitutes: snuff, chewing tobacco, spitless pouched moist snuff, compressed tobacco lozenges. A recent US study found no reduction in smoking rates among people using ST as replacement, although a previous (2006) Swedish study showed an overall country reduction in smoking with increased overall ST consumption.
 products are being marketed as smoking substitutes: snuff, chewing tobacco, spitless pouched moist snuff, compressed tobacco lozenges. A recent US study found no reduction in smoking rates among people using ST as replacement, although a previous (2006) Swedish study showed an overall country reduction in smoking with increased overall ST consumption.")
31
Global Common Smokeless Tobacco Products
North America Chewing tobacco: loose leaf, plug, twist, iq’mik Snuff (spit tobacco): moist, dry Snus (drier moist snuff) Oral compressed tobacco lozenges South America Chimo, tobacco with NaHCO3, brown sugar, vanilla Sweden Snus (finely ground moist tobacco) Britain Gutka (betal quid with tobacco, betel nut and slaked lime), snuff Central Asia Gul (tobacco powder and molasses), nass or naswar, niswar, pan masala or betel quid, zarda East/SE Asia Gutka, pan masala or betel quid South Asia Snuff (creamy), gul, gutka, khaini, mawa, mishri, misheri, qiwam or kima, red tooth powder, snus, snuff Middle East Nass or naswar, niswar, shammah, zard Sudan Toombak (fermented ground powdered tobacco with NaHCO3
: moist, dry Snus (drier moist snuff) Oral compressed tobacco lozenges. South America. Chimo, tobacco with NaHCO3, brown sugar, vanilla. Sweden. Snus (finely ground moist tobacco) Britain. Gutka (betal quid with tobacco, betel nut and slaked lime), snuff. Central Asia. Gul (tobacco powder and molasses), nass or naswar, niswar, pan masala or betel quid, zarda. East/SE Asia. Gutka, pan masala or betel quid. South Asia. Snuff (creamy), gul, gutka, khaini, mawa, mishri, misheri, qiwam or kima, red tooth powder, snus, snuff. Middle East. Nass or naswar, niswar, shammah, zard. Sudan. Toombak (fermented ground powdered tobacco with NaHCO3.")
32
Chemical Composition of ST Products
Similar to cigarettes, nicotine is the principal alkaloid Amount of total and free nicotine varies substantially - generally, concentration similar in oral snuff and cigarette tobacco, somewhat lower in chewing tobacco Minor alkaloids: nornicotine, anatabine, anabasine Carcinogens: Combustion-derived Benzo[a]pyrene and other polycyclics lower than in cigarette smoking Carcinogens: Nitrosamines - highest known nonoccupational exposure Nitrite, nitrate, formate, chloride, sulfate, phosphate

33
Impact of Smokeless Tobacco Products on Cardiovascular Disease: Implications for Policy, Prevention and Treatment: A Policy Statement From The American Heart Association 2010 Long-term use of smokeless tobacco products increases the odds of fatal heart attack or fatal stroke (according to analysis of several studies). The AHA advises against smokeless tobacco products for smoking cessation - they are not a “safe” alternative to smoking, and carry the risk of addiction and return to smoking.
. The AHA advises against smokeless tobacco products for smoking cessation - they are not a safe alternative to smoking, and carry the risk of addiction and return to smoking.")
34
Second-Hand Smoke (Environmental Tobacco Smoke “ETS” – Passive Smoking)
Secondhand smoke is a mixture of the smoke given off by the burning end of a cigarette, pipe or cigar and the smoke exhaled from the lungs of smokers. It is involuntarily inhaled by nonsmokers, lingers in the air hours after cigarettes have been extinguished and can cause or exacerbate a wide range of adverse health effects, including Cardiovascular cancer, respiratory infections, and asthma. California Environmental Protection Agency. Identification of Environmental Tobacco Smoke as a Toxic Air Contaminant. Executive Summary. June 2005.

35
The Effects of Second-Hand Smoke
Short-term effects of second-hand smoke: Coughing Headache Eye irritation Sore throat Sneezing and runny nose Feeling sick Breathing problems (and possibly an asthma attack) Irregular heartbeat (a particular problem for people with heart disease) Long-term effects of second-hand smoke: Worsening of chest problems and allergies like asthma, hay fever, bronchitis and emphysema Increased risk of heart disease Increased risk of lung cancer Pregnant women exposed to second hand smoke can pass on the harmful gases and chemicals onto their babies.
 Irregular heartbeat (a particular problem for people with heart disease) Long-term effects of second-hand smoke: Worsening of chest problems and allergies like asthma, hay fever, bronchitis and emphysema. Increased risk of heart disease. Increased risk of lung cancer. Pregnant women exposed to second hand smoke can pass on the harmful gases and chemicals onto their babies.")
36
Coronary heart disease
The health consequences of smoking and second hand smoke evolve over a lifetime. Pregnancy Infant health Child Health and Smoking Physical Growth Behavior and cognitive development Respiratory infections More hospitalization Fetal growth Birth weight Abortions Premature Birth Fetal Death SIDS Adulthood Adolescence Chronic bronchitis Emphysema Lung cancer by 20%–30% Coronary heart disease Stroke COPD Small airway dysfunction Cough Wheezing Phlegm production other respiratory symptoms News release, June 27, 2006; US Department of Health & Human Services. Available at: Mackay J, et al. The Tobacco Atlas. World Health Organization, 2006. Teo KK, et al. Lancet. 2006;368: Fagerström K. Drugs. 2002;62:1-9. Blizzard L, et al. Arch Pediatr Adolesc Med. 2004;158: Leung GM, et al. Arch Pediatr Adolesc Med. 2004;158:

37
Passive Smoking and CV Disability
Have a clear relationship to CV disability & mortality ~ 37,000 to 40,000 people die from cardiovascular disease caused by other people’s smoke every year. Of these, 35,000 non-smokers die from coronary heart disease. Non-smoking adults exposed to secondhand or environmental tobacco smoke (ETS) have an increased risk of lung cancer and heart disease. Young children are especially vulnerable to health hazards of ETS. They are at an increased risk of respiratory illnesses as asthma, bronchitis, pneumonia, as well as sudden infant death syndrome (SIDS). Passive (= Secondhand = Environmental Smoke) has a clear relationship to CV disability & mortality. ~ 37,000 to 40,000 people die from cardiovascular disease caused by other people’s smoke every year. Of these, 35,000 non-smokers die from CHD. Secondhand smoke contains >4000 chemical compounds, >60 of which are known or suspected to be human carcinogens. American Heart Association 2007
 have an increased risk of lung cancer and heart disease. Young children are especially vulnerable to health hazards of ETS. They are at an increased risk of respiratory illnesses as asthma, bronchitis, pneumonia, as well as sudden infant death syndrome (SIDS). Passive (= Secondhand = Environmental Smoke) has a clear relationship to CV disability & mortality. ~ 37,000 to 40,000 people die from cardiovascular disease caused by other people’s smoke every year. Of these, 35,000 non-smokers die from CHD. Secondhand smoke contains >4000 chemical compounds, >60 of which are known or suspected to be human carcinogens. American Heart Association")
38
Importance of Not Smoking During Pregnancy
Rate of Infants with Low-Birth Weight* in Taiwanese Infants by Smoking Status of the Mother (N=9499) OR 1.7 (95% CI: 1.0–2.8) † 4.8 5.8 8.2 2 4 6 8 10 Rate of Infants With Low Birth Weight (%) Never Smoked Quitting Smoking‡ Continued Smoking OR 1.1 (95% CI: 0.9–1.4) Key Points Data were analysed from the Pregnancy Risk Assessment Monitoring System in Taiwan Rates of low birth weight infants by mothers’ smoking status were assessed The “Continued Smoking” population had a significantly higher (OR 1.7) rate of low birth weight infants than the “Never Smoked” population However, the “Quitting Smoking” population (defined as quitting before or by the time of the 1st prenatal visit in the 1st trimester) did not have significantly different birth weight offspring than “Never Smoked” mothers (OR 1.1). Quitting smoking before or during the first trimester may help to decrease the odds of low birth weight infants Background Using data from the Pregnancy Risk Assessment Monitoring System in Taipei City, Taiwan, Wen and colleagues studied the effects of smoking in 9499 women on the health of their newborns. Two-thirds of the women who smoked quit during the first trimester of pregnancy, and only 2.2% of mothers smoked throughout pregnancy. Smoking throughout pregnancy resulted in significantly reduced mean birth weight and a significant increase in the rate of infants with low-birth weight (P<0.05). However, for mothers who quit smoking early in the first trimester, mean birth weights were normal and the rate of infants with low-birth weight was reduced—although it remained significantly greater compared with the rate in mothers who never smoked. Reference 1. Wen CP, Cheng TY, Lin CL, et al. The health benefits of smoking cessation for adult smokers and for pregnant women in Taiwan. Tob Control. 2005;14(Suppl 1):i56–i61. * Low birth weight defined as <2500 g † ORs of having low birth weight infants, adjusted for mothers’ age, education level, parity, and alcohol consumption level, as well as the sex of the infants ‡ Before or during first trimester. Abbreviations: CI, confidence interval; OR, odds ratio Wen CP, et al. Tob Control. 2005;14(Suppl 1):i56-i61.
 OR 1.7 (95% CI: 1.0–2.8) † Rate of Infants With Low Birth Weight (%) Never. Smoked. Quitting Smoking‡ Continued Smoking. OR 1.1 (95% CI: 0.9–1.4) Key Points. Data were analysed from the Pregnancy Risk Assessment Monitoring System in Taiwan. Rates of low birth weight infants by mothers’ smoking status were assessed. The Continued Smoking population had a significantly higher (OR 1.7) rate of low birth weight infants than the Never Smoked population. However, the Quitting Smoking population (defined as quitting before or by the time of the 1st prenatal visit in the 1st trimester) did not have significantly different birth weight offspring than Never Smoked mothers (OR 1.1). Quitting smoking before or during the first trimester may help to decrease the odds of low birth weight infants. Background. Using data from the Pregnancy Risk Assessment Monitoring System in Taipei City, Taiwan, Wen and colleagues studied the effects of smoking in 9499 women on the health of their newborns. Two-thirds of the women who smoked quit during the first trimester of pregnancy, and only 2.2% of mothers smoked throughout pregnancy. Smoking throughout pregnancy resulted in significantly reduced mean birth weight and a significant increase in the rate of infants with low-birth weight (P<0.05). However, for mothers who quit smoking early in the first trimester, mean birth weights were normal and the rate of infants with low-birth weight was reduced—although it remained significantly greater compared with the rate in mothers who never smoked. Reference. 1. Wen CP, Cheng TY, Lin CL, et al. The health benefits of smoking cessation for adult smokers and for pregnant women in Taiwan. Tob Control. 2005;14(Suppl 1):i56–i61. * Low birth weight defined as <2500 g. † ORs of having low birth weight infants, adjusted for mothers’ age, education level, parity, and alcohol consumption level, as well as the sex of the infants. ‡ Before or during first trimester. Abbreviations: CI, confidence interval; OR, odds ratio. Wen CP, et al. Tob Control. 2005;14(Suppl 1):i56-i61.")
39
Second hand Smoke

40
Smoking and coronary artery disease
History Epidemiology CV Effects Importance of Cessation

41
Why Quit? Potential Health Benefits of Quitting Smoking
CHD risk is similar to never smokers 15 years Lung cancer risk is 30%–50% that of continuing smokers 10 years Stroke risk returns to the level of people who have never smoked at 5–15 years post-cessation 5 years Cardiovascular Heart Disease (CHD): excess risk is reduced by 50% among ex-smokers 1 year 3 months Lung function may start to improve with decreased cough, sinus congestion, fatigue, and shortness of breath Key Points The US Surgeon General Report and the American Cancer Society indicate that the health benefits of quitting smoking can start as early as 2 weeks and are sustained After quitting smoking Within 2 weeks to 3 months, lung function can improve and over time, can reach the levels of never smokers After 1 year, risk of cardiovascular heart disease (CHD) can decrease by 50% and continues to decline thereafter Between 5-15 years, risk of stroke can become comparable to never smokers After 10 years, lung cancer risk is reduced to 30%-50% of continuing smokers Moreover, the risk can be reduced for cancers of the larynx, oral cavity, esophagus, pancreas, urinary bladder, and of developing ulcers of the stomach or duodenum After 15 years, CHD risk can return to level of never smokers Background When gauging the health benefits from smoking cessation one is encouraged to assess both the short-term and long-term improvements. Within 2 weeks to 3 months lung function may begin to improve and there may be notable decreases in coughing, sinus congestion, fatigue, and shortness of breath. Around the year mark, coronary heart disease risk, the leading cause of death in the United States, improves with smoking cessation to a point where excess risk is reduced by 50% and continues to decline thereafter. Within the 5–15 year range, the risk of stroke for smoking cessators returns to the level of a person who has never smoked. Other potential long-term benefits include: the risk of lung cancer—the most common cause of cancer death in the United States—declines steadily after smoking cessation; and by 10 years after cessation, the risk of lung cancer is 30%-50% that of continuing smokers. And beyond this, smoking cessation may also reduce the risk of cancers of the larynx, oral cavity, esophagus, pancreas, urinary bladder, and of developing ulcers of the stomach or duodenum. Other long-term benefits include the rate of decline in lung function among former smokers returns to that of never smokers, reducing the risk of COPD. And the risk of coronary heart disease, after 15 years of abstinence, becomes similar to that of a person who has never smoked. Clearly, a patient has health benefits to gain if they successfully quit and remain quit. References US Department of Health & Human Services. The Health Benefits of Smoking Cessation: A Report of the Surgeon General. Centers for Disease Control and Prevention (CDC), Office on Smoking and Health Available at: Accessed July 2006. American Cancer Society. Guide to Quitting Smoking. Available at: Cessation USDHHS. The Health Benefits of Smoking Cessation: A Report of the Surgeon General, Available at: American Cancer Society. Guide to Quitting Smoking. Available at:
: excess risk is reduced by 50% among ex-smokers. 1 year. 3 months. Lung function may start to improve with decreased cough, sinus congestion, fatigue, and shortness of breath. Key Points. The US Surgeon General Report and the American Cancer Society indicate that the health benefits of quitting smoking can start as early as 2 weeks and are sustained. After quitting smoking. Within 2 weeks to 3 months, lung function can improve and over time, can reach the levels of never smokers. After 1 year, risk of cardiovascular heart disease (CHD) can decrease by 50% and continues to decline thereafter. Between 5-15 years, risk of stroke can become comparable to never smokers. After 10 years, lung cancer risk is reduced to 30%-50% of continuing smokers. Moreover, the risk can be reduced for cancers of the larynx, oral cavity, esophagus, pancreas, urinary bladder, and of developing ulcers of the stomach or duodenum. After 15 years, CHD risk can return to level of never smokers. Background. When gauging the health benefits from smoking cessation one is encouraged to assess both the short-term and long-term improvements. Within 2 weeks to 3 months lung function may begin to improve and there may be notable decreases in coughing, sinus congestion, fatigue, and shortness of breath. Around the year mark, coronary heart disease risk, the leading cause of death in the United States, improves with smoking cessation to a point where excess risk is reduced by 50% and continues to decline thereafter. Within the 5–15 year range, the risk of stroke for smoking cessators returns to the level of a person who has never smoked. Other potential long-term benefits include: the risk of lung cancer—the most common cause of cancer death in the United States—declines steadily after smoking cessation; and by 10 years after cessation, the risk of lung cancer is 30%-50% that of continuing smokers. And beyond this, smoking cessation may also reduce the risk of cancers of the larynx, oral cavity, esophagus, pancreas, urinary bladder, and of developing ulcers of the stomach or duodenum. Other long-term benefits include the rate of decline in lung function among former smokers returns to that of never smokers, reducing the risk of COPD. And the risk of coronary heart disease, after 15 years of abstinence, becomes similar to that of a person who has never smoked. Clearly, a patient has health benefits to gain if they successfully quit and remain quit. References. US Department of Health & Human Services. The Health Benefits of Smoking Cessation: A Report of the Surgeon General. Centers for Disease Control and Prevention (CDC), Office on Smoking and Health Available at: Accessed July American Cancer Society. Guide to Quitting Smoking. Available at: Cessation. USDHHS. The Health Benefits of Smoking Cessation: A Report of the Surgeon General, Available at: American Cancer Society. Guide to Quitting Smoking. Available at:")
42
Quitting at Any Age May Increase Life Expectancy Age Stopped Smoking: 45–54 Years Old
Results From a Study of Male Physician Smokers in the UK Nonsmokers Age Stopped: 45–54 Cigarette Smokers Percentage Survival from Age 50 Key Points This prospective study investigated the impact of smoking and of quitting smoking on the overall mortality of 34,439 male doctors in the United Kingdom from 1951 to 2001 Survival curves from age 45 years revealed that, compared to lifelong smokers: Nonsmokers have about a 10 year longer life expectancy Smokers who stop by age 50, have a 6 year longer life expectancy The sooner smokers quit, the more likely their life expectancy would return to that of non-smokers Although even quitting smoking later in life can provide benefits in life expectancy Background This prospective study by Doll and colleagues, used periodically mailed questionnaires to investigate the impact of smoking and of quitting smoking, on the overall mortality of 34,439 male doctors in the United Kingdom from 1951 to Survival curves for percentage survival from age 35 years for male physicians born in 1900–1930 revealed a 10-year shift in overall survival for those who continued smoking cigarettes vs lifelong nonsmokers. This means that, on average, participants who never smoked lived 10 years longer than those who were current smokers. By age 70 years, 81% of lifelong nonsmokers were alive vs 59% of continuing cigarette smokers. A mortality rate of approximately 75% was reached at age 80 years for smokers, but was not reached until age 90 years for nonsmokers. Reference 1. Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519–1527. Age (Years) Even quitting smoking later in life can lead to longer life expectancy Doll R, et al. BMJ. 2004;328:
 Even quitting smoking later in life can lead to longer life expectancy. Doll R, et al. BMJ. 2004;328:")
44
Smoking bans in public places and workplaces are significantly associated with a reduction in AMI incidence, particularly if enforced over several years.

45
Countries Banning Smoking in Public Places
Nigeria Norway 2004 Paraguay Peru Philippines (partial) Poland (partial) Portugal 2007 Puerto Rico Singapore Serbia Slovenia South Africa 2001 Spain Sweden (partial) Syria 2009 Thailand and more! Albania 2007 Andorra (partial) Argentina-Buenos Aires 2006 Armenia (partial) Australia Austria (partial) Bahrain 2008 Bosnia-Herzegv.2007 Brazil 2009 Bulgaria (partial) Canada Chile (partial) China (partial) Colombia 2009 Croatia Cyprus 2009 Czech Rep.(partial) Denmark 2007 Estonia (partial) Finland 2007 France 2008 Germany (contested) Greece 1010 Guatemala Hong Kong 2007 Hungary (partial) Iceland India (partial) Indonesia (partial) Ireland 2004 Israel Kazakhstan Kenya 2007 Latvia 2010 Lithuania (partial) Luxemburg (partial) Macedonia 2010 Malta Malaysia Mexico 2008 Monaco (partial) Montenegro Morocco Mozambique 2007 Namibia 2010 Netherlands New Zealand 2004 Source: Wikipedia
 Poland (partial) Portugal Puerto Rico. Singapore. Serbia. Slovenia. South Africa Spain Sweden (partial) Syria Thailand 2008 and more! Albania Andorra (partial) Argentina-Buenos Aires Armenia (partial) Australia Austria (partial) Bahrain Bosnia-Herzegv Brazil Bulgaria (partial) Canada. Chile (partial) China (partial) Colombia Croatia Cyprus Czech Rep.(partial) Denmark Estonia (partial) Finland France Germany (contested) Greece Guatemala. Hong Kong Hungary (partial) Iceland. India (partial) Indonesia (partial) Ireland Israel. Kazakhstan Kenya Latvia Lithuania (partial) Luxemburg (partial) Macedonia Malta. Malaysia. Mexico Monaco (partial) Montenegro. Morocco. Mozambique Namibia Netherlands. New Zealand Source: Wikipedia.")
46
Beneficial Effects of Smoking Ban for Employees
10 20 30 40 Before ban After Ban Symptoms among 67 barmen before and after ban dyspnea morning cough cough sputum eye irritation nose irritation throat irritation Number of barmen with symptoms Source: Eisner M et coll., JAMA 1998, 280,

47
Smoking and coronary artery disease
History Epidemiology CV Effects Importance of Cessation Nicotine addiction

48
Nicotine Addictive or Just a Bad Habit??????

49
WHAT IS ADDICTION? ”Compulsive drug use, without medical purpose, in the face of negative consequences” Alan I. Leshner, Ph.D. Former Director, National Institute on Drug Abuse National Institutes of Health Many people believe that addiction is a result of weakness in character and an inability to change one’s behavior. But is it really that simple? Research contradicts this position. Nicotine addiction is a form of chronic brain disease resulting from an alteration in brain chemistry (Leshner, 1997, 1999). Dr. Alan Leshner, the former director of the National Institute on Drug Abuse, simply defines drug addiction as “compulsive use, without medical purpose, in the face of negative consequences” (Leshner, 1997). But how does human behavior fit into this equation? Leshner Al. (1997, April). Drug abuse and addiction are biomedical problems. Hosp Pract (special report):2–4. Leshner AI. (1999). Science-based views of drug addiction and its treatment. JAMA 282:1314–1316.
. Dr. Alan Leshner, the former director of the National Institute on Drug Abuse, simply defines drug addiction as compulsive use, without medical purpose, in the face of negative consequences (Leshner, 1997). But how does human behavior fit into this equation Leshner Al. (1997, April). Drug abuse and addiction are biomedical problems. Hosp Pract (special report):2–4. Leshner AI. (1999). Science-based views of drug addiction and its treatment. JAMA 282:1314–1316.")
51
NICOTINE PHARMACODYNAMICS
Nicotine binds to receptors in the brain and other sites in the body. Central nervous system Cardiovascular system Exocrine glands Nicotine pharmacodynamics refers to the effects that nicotine has on the body. Nicotine is a potent agent that affects numerous organ systems, including the cardiovascular, endocrine, musculoskeletal, and neurologic systems, as shown in this diagram. Following absorption, nicotine binds to receptors in the brain and other sites in the body, inducing a variety of predominantly stimulant and, to a lesser extent, sedative effects (Taylor, 2006). Taylor P. (2006). Agents acting at the neuromuscular junction and autonomic ganglia. In Brunton LL, Lazo JS, Parker KL (eds.), Goodman and Gilman's The Pharmacological Basis of Therapeutics, 11th ed. New York: McGraw-Hill. Gastrointestinal system Adrenal medulla Other: Neuromuscular junction Sensory receptors Other organs Peripheral nervous system Nicotine has predominantly stimulant effects.
. Taylor P. (2006). Agents acting at the neuromuscular junction and autonomic ganglia. In Brunton LL, Lazo JS, Parker KL (eds.), Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th ed. New York: McGraw-Hill. Gastrointestinal system. Adrenal medulla. Other: Neuromuscular junction. Sensory receptors. Other organs. Peripheral nervous system. Nicotine has predominantly stimulant effects.")
52
Mechanism of Action of Nicotine in the Central Nervous System
b2 4b2 nicotinic acetylcholine receptor (nAChR) Key Points Nicotine stimulates dopamine release in areas of the brain (eg, α4β2 nicotinic acetylcholine receptors in ventral tegmental area) This stimulation is believed to cause dopamine release in the nucleus accumbens Activation of nucleus accumbens neurons may be related to the reward and satisfaction effect associated with smoking Background After inhalation, nicotine preferentially binds to nicotinic acetylcholine receptors (nAChRs) located in the mesolimbic-dopamine system of the brain within a matter of seconds. Nicotine specifically activates 4β2 nicotinic receptors in the Ventral Tegmental Area (VTA) causing an immediate dopamine release at the Nucleus Accumbens (nAcc).1 The dopamine release is believed to be a key component of the reward circuitry associated with cigarette smoking.1 Reference 1. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S Nicotine binds preferentially to nAChRs in the central nervous system; one key area is the α4β2 nicotinic receptor in the VTA After nicotine binds to the α4β2 nAChR in the VTA, dopamine is released in the nAcc which is believed to be linked to reward
 Key Points. Nicotine stimulates dopamine release in areas of the brain (eg, α4β2 nicotinic acetylcholine receptors in ventral tegmental area) This stimulation is believed to cause dopamine release in the nucleus accumbens. Activation of nucleus accumbens neurons may be related to the reward and satisfaction effect associated with smoking. Background. After inhalation, nicotine preferentially binds to nicotinic acetylcholine receptors (nAChRs) located in the mesolimbic-dopamine system of the brain within a matter of seconds. Nicotine specifically activates 4β2 nicotinic receptors in the Ventral Tegmental Area (VTA) causing an immediate dopamine release at the Nucleus Accumbens (nAcc).1 The dopamine release is believed to be a key component of the reward circuitry associated with cigarette smoking.1. Reference. 1. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S Nicotine binds preferentially to nAChRs in the central nervous system; one key area is the α4β2 nicotinic receptor in the VTA. After nicotine binds to the α4β2 nAChR in the VTA, dopamine is released in the nAcc which is believed to be linked to reward.")
53
The Cycle of Nicotine Addiction
Nicotine binding causes an increase in release of dopamine1,2 Dopamine gives feelings of pleasure and calmness1 competitive binding of nicotine to nicotinic acetylcholine receptors causes prolonged activation, desensitization, and upregulation2 Dopamine Nicotine Key Points For most people, smoking is a nicotine addiction Nicotine addiction is a cycle, as described in the slide It begins with nicotine binding to receptors in the brain This causes a release of dopamine, which in turn results in feelings of pleasure and calmness A lack of nicotine (eg, during smoking abstinence) leads to dopamine decrease Craving is increased to replenish dopamine levels Background The binding of nicotine to its relevant receptors results in the release of multiple neurotransmitters, most critically dopamine. The release of dopamine in the nucleus accumbens neurons is thought to play a critical role in the addictive nature of nicotine. This release of dopamine requires binding of nicotine to 42 receptors.1,2 Absorption of cigarette smoke from the lungs is rapid and complete, producing with each inhalation a high concentration of arterial nicotine that reaches the brain within 10 to 16 seconds. Nicotine has a terminal half-life in blood of 2 hours. Smokers therefore experience a pattern of repetitive and transient high blood nicotine concentrations from each cigarette. Nicotine’s activation of acetylcholinergic receptors induces the release of dopamine in the nucleus accumbens. This is similar to the effect produced by other drugs of misuse, such as amphetamines and cocaine. The symptoms of nicotine withdrawal are a major barrier to smoking cessation for most people. Smokers start to experience impairment of mood and performance within hours of their last cigarette. These effects are completely alleviated by smoking a cigarette. Withdrawal symptoms include irritability, restlessness, feeling miserable, impaired concentration, and increased appetite, as well as craving for cigarettes. Cravings, sometimes intense, can persist for many months. References Jarvis MJ. Why people smoke. BMJ. 2004;328: Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S121-S125. Jarvis MJ. BMJ. 2004; 328: Picciotto MR, et al. Nicotine and Tob Res. 1999:Suppl 2:S121-S125.
 leads to dopamine decrease. Craving is increased to replenish dopamine levels. Background. The binding of nicotine to its relevant receptors results in the release of multiple neurotransmitters, most critically dopamine. The release of dopamine in the nucleus accumbens neurons is thought to play a critical role in the addictive nature of nicotine. This release of dopamine requires binding of nicotine to 42 receptors.1,2. Absorption of cigarette smoke from the lungs is rapid and complete, producing with each inhalation a high concentration of arterial nicotine that reaches the brain within 10 to 16 seconds. Nicotine has a terminal half-life in blood of 2 hours. Smokers therefore experience a pattern of repetitive and transient high blood nicotine concentrations from each cigarette. Nicotine’s activation of acetylcholinergic receptors induces the release of dopamine in the nucleus accumbens. This is similar to the effect produced by other drugs of misuse, such as amphetamines and cocaine. The symptoms of nicotine withdrawal are a major barrier to smoking cessation for most people. Smokers start to experience impairment of mood and performance within hours of their last cigarette. These effects are completely alleviated by smoking a cigarette. Withdrawal symptoms include irritability, restlessness, feeling miserable, impaired concentration, and increased appetite, as well as craving for cigarettes. Cravings, sometimes intense, can persist for many months. References. Jarvis MJ. Why people smoke. BMJ. 2004;328: Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S121-S125. Jarvis MJ. BMJ. 2004; 328: Picciotto MR, et al. Nicotine and Tob Res. 1999:Suppl 2:S121-S125.")
54
The Cycle of Nicotine Addiction ( continued)
As nicotine levels decrease, receptors revert to an open state causing hyperexcitability leading to cravings1,2 The dopamine decrease between cigarettes leads to withdrawal symptoms of irritability and stress1 The smoker craves nicotine to release more dopamine to restore pleasure and calmness1 Dopamine Nicotine Key Points For most people, smoking is a nicotine addiction Nicotine addiction is a cycle, as described in the slide It begins with nicotine binding to receptors in the brain This causes a release of dopamine, which in turn results in feelings of pleasure and calmness A lack of nicotine (eg, during smoking abstinence) leads to dopamine decrease Craving is increased to replenish dopamine levels Background The binding of nicotine to its relevant receptors results in the release of multiple neurotransmitters, most critically dopamine. The release of dopamine in the nucleus accumbens neurons is thought to play a critical role in the addictive nature of nicotine. This release of dopamine requires binding of nicotine to 42 receptors.1,2 Absorption of cigarette smoke from the lungs is rapid and complete, producing with each inhalation a high concentration of arterial nicotine that reaches the brain within 10 to 16 seconds. Nicotine has a terminal half-life in blood of 2 hours. Smokers therefore experience a pattern of repetitive and transient high blood nicotine concentrations from each cigarette. Nicotine’s activation of acetylcholinergic receptors induces the release of dopamine in the nucleus accumbens. This is similar to the effect produced by other drugs of misuse, such as amphetamines and cocaine. The symptoms of nicotine withdrawal are a major barrier to smoking cessation for most people. Smokers start to experience impairment of mood and performance within hours of their last cigarette. These effects are completely alleviated by smoking a cigarette. Withdrawal symptoms include irritability, restlessness, feeling miserable, impaired concentration, and increased appetite, as well as craving for cigarettes. Cravings, sometimes intense, can persist for many months. References Jarvis MJ. Why people smoke. BMJ. 2004;328: Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S121-S125. Jarvis MJ. BMJ. 2004; 328: Picciotto MR, et al. Nicotine and Tob Res. 1999:Suppl 2:S121-S125.
 leads to dopamine decrease. Craving is increased to replenish dopamine levels. Background. The binding of nicotine to its relevant receptors results in the release of multiple neurotransmitters, most critically dopamine. The release of dopamine in the nucleus accumbens neurons is thought to play a critical role in the addictive nature of nicotine. This release of dopamine requires binding of nicotine to 42 receptors.1,2. Absorption of cigarette smoke from the lungs is rapid and complete, producing with each inhalation a high concentration of arterial nicotine that reaches the brain within 10 to 16 seconds. Nicotine has a terminal half-life in blood of 2 hours. Smokers therefore experience a pattern of repetitive and transient high blood nicotine concentrations from each cigarette. Nicotine’s activation of acetylcholinergic receptors induces the release of dopamine in the nucleus accumbens. This is similar to the effect produced by other drugs of misuse, such as amphetamines and cocaine. The symptoms of nicotine withdrawal are a major barrier to smoking cessation for most people. Smokers start to experience impairment of mood and performance within hours of their last cigarette. These effects are completely alleviated by smoking a cigarette. Withdrawal symptoms include irritability, restlessness, feeling miserable, impaired concentration, and increased appetite, as well as craving for cigarettes. Cravings, sometimes intense, can persist for many months. References. Jarvis MJ. Why people smoke. BMJ. 2004;328: Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S121-S125. Jarvis MJ. BMJ. 2004; 328: Picciotto MR, et al. Nicotine and Tob Res. 1999:Suppl 2:S121-S125.")
55
Withdrawal Syndrome: A Combination of Physical and Psychological Conditions, Making Smoking Hard to Treat Decreased heart rate Irritability, frustration, or anger Insomnia/sleep disturbance Anxiety (may increase or decrease with quitting) Increased appetite or weight gain Key Points According to the Diagnostic and Statistical Manual of Mental Disorders, IV-TR, during periods of abstinence, smokers can undergo nicotine withdrawal syndrome Nicotine withdrawal syndrome: Can occur rapidly after a smoker attempts to quit Is characterised by a combination of physical and psychological conditions The typical duration of most of these symptoms is <4 weeks Increased appetite is an exception, often lasting >10 weeks Background Recognizing that nicotine withdrawal results in clinically significant impairment in a person’s ability to function, the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) classifies these symptoms as a distinct condition: nicotine withdrawal syndrome. The symptoms of nicotine withdrawal syndrome can develop rapidly after a smoker tries to quit, and characteristics include the psychological symptoms of dysphoric or depressed mood; anxiety; irritability, frustration, or anger; and restlessness or impatience and the physical symptoms of insomnia, increased appetite/weight gain, and difficulty concentrating. Although present in those who use other nicotine-containing products, the manifestations of nicotine withdrawal syndrome are more intense in individuals who smoke compared with those who use other forms of tobacco. The rapidity of onset and intensity of withdrawal syndrome in smokers may suggest a greater dependence on tobacco.1 The typical duration of most of these symptoms is <4 weeks. Increased appetite is an exception, often lasting for >10 weeks. Although anxiety is listed as a classic symptom of nicotine withdrawal in the DSM, additional information is available about the relationship between anxiety and smoking. Some evidence suggests that while smokers increase their smoking when stressed, smoking does not help relieve the stress. As smokers stop smoking, levels of stress and anxiety actually decrease.2 References 1. Diagnostic and Statistical Manual of Mental Disorders, IV-TR. Washington, DC: APA; 2006: Available at Accessed November 7, 2006. 2. West R, Shiffman S. Fast Facts: Smoking Cessation. 1st ed. Oxford, United Kingdom. Health Press Limited Restlessness or impatience Dysphoric or depressed mood Difficulty concentrating DSM-IV-TR. APA; 2006: Available at:
 Increased appetite or weight gain. Key Points. According to the Diagnostic and Statistical Manual of Mental Disorders, IV-TR, during periods of abstinence, smokers can undergo nicotine withdrawal syndrome. Nicotine withdrawal syndrome: Can occur rapidly after a smoker attempts to quit. Is characterised by a combination of physical and psychological conditions. The typical duration of most of these symptoms is <4 weeks. Increased appetite is an exception, often lasting >10 weeks. Background. Recognizing that nicotine withdrawal results in clinically significant impairment in a person’s ability to function, the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) classifies these symptoms as a distinct condition: nicotine withdrawal syndrome. The symptoms of nicotine withdrawal syndrome can develop rapidly after a smoker tries to quit, and characteristics include the psychological symptoms of dysphoric or depressed mood; anxiety; irritability, frustration, or anger; and restlessness or impatience and the physical symptoms of insomnia, increased appetite/weight gain, and difficulty concentrating. Although present in those who use other nicotine-containing products, the manifestations of nicotine withdrawal syndrome are more intense in individuals who smoke compared with those who use other forms of tobacco. The rapidity of onset and intensity of withdrawal syndrome in smokers may suggest a greater dependence on tobacco.1. The typical duration of most of these symptoms is <4 weeks. Increased appetite is an exception, often lasting for >10 weeks. Although anxiety is listed as a classic symptom of nicotine withdrawal in the DSM, additional information is available about the relationship between anxiety and smoking. Some evidence suggests that while smokers increase their smoking when stressed, smoking does not help relieve the stress. As smokers stop smoking, levels of stress and anxiety actually decrease.2. References. 1. Diagnostic and Statistical Manual of Mental Disorders, IV-TR. Washington, DC: APA; 2006: Available at Accessed November 7, West R, Shiffman S. Fast Facts: Smoking Cessation. 1st ed. Oxford, United Kingdom. Health Press Limited Restlessness or impatience. Dysphoric or depressed mood. Difficulty concentrating. DSM-IV-TR. APA; 2006: Available at:")
56
50% are likely to relapse in the first month
The greatest risk of relapse is during the first three months after quitting. 37% have their first lapse between 8:00pm and midnight 50% are likely to relapse in the first month 67% are likely to relapse in the first three months DSM-IV-TR. APA; 2006: Available at:

57
“Nine out of ten ex-smokers who have a cigarette after quitting later return to smoking” (Brandon, 1990)
")
58
Many Health Organizations Emphasise the Important Role Physicians Can Play in Helping Their Patients Quit Smoking World Health Organization1 Health Professionals Against Smoking2 The American Academy of Family Physicians3 American Medical Association2 National Institute for Health and Clinical Excellence4 Key Points Leading health organizations from around the world emphasise the physician’s role in helping their patients to quit smoking Background: WHO: “Health workers function as exemplars and educators for their patients, and consequently should set an example by abstaining from tobacco.” Health Professional Against Smoking: “The detrimental effects of smoking constitute one of the most urgent health problems in Europe. Individual doctors have a clear duty and responsibility toward their patients in this respect. Campaigns to inform the public of the damage to health caused by smoking will not be convincing if doctors—as individuals and as a profession—are seen as smokers.” AAFP: “The American Academy of Family Physicians strongly encourages all of its members and staff to personally avoid tobacco use. The AAFP urges its members to: save lives by working toward elimination of all tobacco use; document use of tobacco products in patient charts; work cooperatively with other health professionals to provide cessation counselling and other treatments; discourage tobacco use in all public and workplace settings; and, list tobacco as a cause on death certificates when appropriate.” AMA: “Tobacco dependence is a chronic illness, much like diabetes or high blood pressure, and it requires that doctors take the same long-term treatment approach to help patients succeed.” NICE: “A body of level 1+ evidence directly applicable to UK health care settings supports the efficacy of physician advice as a brief intervention for smoking cessation.” References 1. World Health Organization. Mayo report on addressing the worldwide tobacco epidemic through effective, evidence-based treatment. Report of an expert meeting, March 1999, Rochester (Minnesota) USA. Available at: Accessed July 2006. 2. The American Academy of Family Physicians. Tobacco use, prevention and cessation. Available at: Accessed July 2006. 3. American Cancer Society. Tobacco control strategy planning, companion guide #2: Engaging doctors in tobacco control. Available at: Accessed July 2006. 4. National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in primary care. Available at: Accessed August 2006. World Health Organization. Mayo report on addressing the worldwide tobacco epidemic through effective, evidence-based treatment. Report of an expert meeting, March 1999, Rochester (Minnesota) USA. Available at: Accessed July 2006. American Cancer Society. Tobacco control strategy planning, companion guide #2: Engaging doctors in tobacco control. Available at: The American Academy of Family Physicians. Tobacco use, prevention and cessation. Available at: National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in primary care and other settings. Available at:
 USA. Available at: Accessed July The American Academy of Family Physicians. Tobacco use, prevention and cessation. Available at: Accessed July American Cancer Society. Tobacco control strategy planning, companion guide #2: Engaging doctors in tobacco control. Available at: Accessed July National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in primary care. Available at: o= Accessed August World Health Organization. Mayo report on addressing the worldwide tobacco epidemic through effective, evidence-based treatment. Report of an expert meeting, March 1999, Rochester (Minnesota) USA. Available at: Accessed July American Cancer Society. Tobacco control strategy planning, companion guide #2: Engaging doctors in tobacco control. Available at: The American Academy of Family Physicians. Tobacco use, prevention and cessation. Available at: National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in primary care and other settings. Available at: o=")
59
READINESS to make a quit attempt
US PHS Guideline – Treating Tobacco Use and Dependence: 2008 Update Tobacco Dependence Support – The “5 A’s” ASK about tobacco USE ADVISE tobacco users to QUIT As a final review, the 5 A’s are as follows: Ask about tobacco use. Advise tobacco users to quit. Assess readiness to make a quit attempt. Assist with the quit attempt. Arrange follow-up care. Each of these is a key component of comprehensive tobacco cessation counseling interventions. ASSESS READINESS to make a quit attempt ASSIST with the QUIT ATTEMPT ARRANGE FOLLOW-UP care

60
Reference Rigotti NA. Treatment of tobacco use and dependence. N Engl J Med. 2002;346:

61
All decrease cravings, withdrawal
US PHS Guideline – Treating Tobacco Use and Dependence: 2008 Update First-line Pharmacotherapies for Tobacco Dependence1 Nicotine replacement therapy (NRT) Patch Gum Inhaler Nasal spray Sublingual tablets/lozenges Bupropion SR Champix (Varenicline) Key Points Based upon systematic review and meta-analyses, these are the first-line therapies recommended by the US PHS Guideline – Treating Tobacco Use and Dependence: 2008 Update Nicotine replacement therapy comes in 5 forms 1 slow-acting sustained form (patch) 4 faster-acting acute forms (gum, inhaler, nasal spray, sublingual tablet/lozenge) Bupropion SR (sustained-release) is an antidepressant with an indication for smoking cessation Varenicline is an α4β2 nicotinic receptor partial agonist that was specifically designed for smoking cessation References 1. Fiore MC, et al. Clinical Practice Guideline. Treating Tobacco Use and Dependence: 2008 Update. US Department of Health and Human Services. Public Health Service. Rockville, MD All decrease cravings, withdrawal 20-25% quit rates at 1 year Fiore MC, et al. Clinical Practice Guideline. Treating Tobacco Use and Dependence: 2008 Update. USDHHS. PHS. Rockville, MD
 Patch. Gum. Inhaler. Nasal spray. Sublingual tablets/lozenges. Bupropion SR. Champix (Varenicline) Key Points. Based upon systematic review and meta-analyses, these are the first-line therapies recommended by the US PHS Guideline – Treating Tobacco Use and Dependence: 2008 Update. Nicotine replacement therapy comes in 5 forms. 1 slow-acting sustained form (patch) 4 faster-acting acute forms (gum, inhaler, nasal spray, sublingual tablet/lozenge) Bupropion SR (sustained-release) is an antidepressant with an indication for smoking cessation. Varenicline is an α4β2 nicotinic receptor partial agonist that was specifically designed for smoking cessation. References. 1. Fiore MC, et al. Clinical Practice Guideline. Treating Tobacco Use and Dependence: 2008 Update. US Department of Health and Human Services. Public Health Service. Rockville, MD All decrease cravings, withdrawal % quit rates at 1 year. Fiore MC, et al. Clinical Practice Guideline. Treating Tobacco Use and Dependence: 2008 Update. USDHHS. PHS. Rockville, MD")
62
21 References Benowitz NL, Porchet H, Sheiner L, et al. Nicotine absorption and cardiovascular effects with smokeless tobacco use: comparison with cigarettes and nicotine gum. Clin Pharmacol Ther. 1988; 44:23-28. Schneider NG, Lunell E, Olmstead RE, et al. Clinical pharmacokinetics of nasal nicotine delivery. A review and comparison to other nicotine systems. Clin Pharmacokinet. 1996; 31: Benowitz NL. Nicotine replacement therapy: what has been accomplished – can we do better? Drugs. 1993;45:

63
(varenicline) A Selective 42 Nicotinic Acetylcholine Receptor Partial Agonist
 A Selective 42 Nicotinic Acetylcholine Receptor Partial Agonist")
64
Champix (varenicline): A Highly Selective 42 Receptor Partial Agonist
Nicotine Varenicline Binding of nicotine at the 42 nicotinic receptor in the Ventral Tegmental Area (VTA) is believed to cause large amounts of dopamine to be released at the Nucleus Accumbens (nAcc) Ref1/Coe/ 1/1/2/5-8 Ref2/Picciotto/ S123/2/3/1-16 The initial view of the mesolimbic system identifies the Ventral Tegmental Area (VT) where the 42 receptors predominate, as well as the Nucleus Accumbens (nAcc). The release of dopamine at the nAcc from the axons of the dopamine cells of the VTA is believed to produce a reward response. When nicotine binds at the 42 nicotinic receptor in the Ventral Tegmental Area (VTA), it is believed to cause release of dopamine at the Nucleus Accumbens (nAcc). Chantix was deliberately designed for the 42 receptor, as an 42 nicotinic receptor partial agonist (with dual agonist and antagonist properties) and physically prevents nicotine from binding and releases intrinsically less dopamine at the nAcc. Binding of nicotine at the 42 nicotinic receptor in the Ventral Tegmental Area (VTA) is believed to cause release of dopamine at the Nucleus Accumbens (nAcc) Varenicline is an 42 nicotinic receptor partial agonist, a compound with dual agonist and antagonist activities. This is believed to result in both a lesser amount of dopamine release from the VTA at the nAcc as well as the prevention of nicotine binding at the 42 receptors 1. Coe JW et al. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco Prague, Czech Republic. 2. Picciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S References Coe JW, Brooks PR, Wirtz MC, et al. Varenicline (CP-526, 555): A novel, potent, and selective nicotinic receptor partial agonist for the treatment of smoking cessation: Rationale, discovery, and mode of action. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco, March 20–23, 2005, Prague, Czech Republic. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S
 is believed to cause large amounts of dopamine to be released at the Nucleus Accumbens (nAcc) Ref1/Coe/ 1/1/2/5-8. Ref2/Picciotto/ S123/2/3/1-16. The initial view of the mesolimbic system identifies the Ventral Tegmental Area (VT) where the 42 receptors predominate, as well as the Nucleus Accumbens (nAcc). The release of dopamine at the nAcc from the axons of the dopamine cells of the VTA is believed to produce a reward response. When nicotine binds at the 42 nicotinic receptor in the Ventral Tegmental Area (VTA), it is believed to cause release of dopamine at the Nucleus Accumbens (nAcc). Chantix was deliberately designed for the 42 receptor, as an 42 nicotinic receptor partial agonist (with dual agonist and antagonist properties) and physically prevents nicotine from binding and releases intrinsically less dopamine at the nAcc. Binding of nicotine at the 42 nicotinic receptor in the Ventral Tegmental Area (VTA) is believed to cause release of dopamine at the Nucleus Accumbens (nAcc) Varenicline is an 42 nicotinic receptor partial agonist, a compound with dual agonist and antagonist activities. This is believed to result in both a lesser amount of dopamine release from the VTA at the nAcc as well as the prevention of nicotine binding at the 42 receptors. 1. Coe JW et al. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco Prague, Czech Republic. 2. Picciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S References. Coe JW, Brooks PR, Wirtz MC, et al. Varenicline (CP-526, 555): A novel, potent, and selective nicotinic receptor partial agonist for the treatment of smoking cessation: Rationale, discovery, and mode of action. Presented at the 11th Annual Meeting and 7th European Conference of the Society for Research on Nicotine and Tobacco, March 20–23, 2005, Prague, Czech Republic. Picciotto MR, Zoli M, Changeux J. Use of knock-out mice to determine the molecular basis for the actions of nicotine. Nicotine Tob Res. 1999; Suppl 2:S")
65
Continuous Abstinence
Champix (varenicline) Efficacy Measurements: CO-Confirmed 4-Wk Continuous Abstinence Rates Wks 9–12 Ref1/Gonzalez/ 51/1/2/1-10 Ref1/Gonzalez/ 51/Fig 2 100 44.0 43.9 29.8 29.5 17.6 17.7 20 40 60 n=352 n=329 n=344 n=342 n=341 P < 0.001 P < 0.001 Ref2/Jorenby/ 59/1/2/10-16 Ref2/Jorenby/ 60/Fig 2 P < 0.001 P < 0.001 Continuous Abstinence Rate (%) P < 0.001 P = 0.001 Analyses of smoking cessation rates for the All Subjects population showed that varenicline was significantly more efficacious than placebo in all measures of abstinence, both at the end of the 12-week treatment period and during the non-pharmacologic treatment follow-up through Week 24 and Week 52. The 9-12 week Continuous Abstinence Rate is defined as the percentage of randomized subjects who abstained from smoking (not even a puff) from Week 9 through 12 of the study as confirmed by both subject self-report and by end-expiratory CO measurement of ≤10 parts per million at each clinic visit. The primary endpoint, which was abstinence from even a single puff of a cigarette (patient reported and CO-confirmed at study visits) during weeks 9, 10, 11, and 12, was nearly identical in the two studies. This Continuous Abstinence Rate was 44% in the varenicline groups. Each of the comparisons were statistically significant. Varenicline also showed significantly greater response rates vs.bupropion SR in these analyses. The studies above correspond to Study 4 and Study 5 in the Chantix full prescribing information. The most frequently reported adverse events (>10%) with Chantix were nausea, headache, insomnia, and abnormal dreams. Nausea was reported by approximately 30% of patients treated with Chantix 1 mg bid, with approximately a 3% discontinuation rate during 12 weeks of treatment. Nausea was generally described as mild or moderate and often transient. For some subjects, it was persistent over several months. Gonzales et al. Jorenby et al. Varenicline Bupropion SR Placebo The 9-12 week Continuous Abstinence Rate is defined as the percentage of subjects who abstained from smoking (not even a puff) from Week 9 through 12 of the study as confirmed by both subject self-report and by end-expiratory carbon monoxide (CO) measurement Chantix PI/ 13/1/¶1 Chantix PI/ 9/1/¶5 1. Gonzalez D et al. JAMA. 2006;296: Jorenby DE et al. JAMA. 2006;296:56-63. References Gonzalez D, Rennard SI, Billing CB, et al. Varenicline, an 42 Nicotinic Acetylcholine Receptor Partial Agonist, vs Sustained-Release Bupropion and Placebo for Smoking Cessation. JAMA. 2006;296:47-55. Jorenby DE, Hays JT, Rigotti MD, et al. Efficacy of Varenicline, an 42 Nicotinic Acetylcholine Receptor Partial Agonist, vs Placebo or Sustained-Release Bupropion for Smoking Cessation. JAMA. 2006;296:56-63. Chantix Prescribing Information. Pfizer Inc, New York, NY. (May 2006)
 Efficacy Measurements: CO-Confirmed 4-Wk Continuous Abstinence Rates Wks 9–12. Ref1/Gonzalez/ 51/1/2/1-10. Ref1/Gonzalez/ 51/Fig n=352. n=329. n=344. n=342. n=341. P < P < Ref2/Jorenby/ 59/1/2/ Ref2/Jorenby/ 60/Fig 2. P < P < Continuous Abstinence. Rate (%) P < P = Analyses of smoking cessation rates for the All Subjects population showed that varenicline was significantly more efficacious than placebo in all measures of abstinence, both at the end of the 12-week treatment period and during the non-pharmacologic treatment follow-up through Week 24 and Week 52. The 9-12 week Continuous Abstinence Rate is defined as the percentage of randomized subjects who abstained from smoking (not even a puff) from Week 9 through 12 of the study as confirmed by both subject self-report and by end-expiratory CO measurement of ≤10 parts per million at each clinic visit. The primary endpoint, which was abstinence from even a single puff of a cigarette (patient reported and CO-confirmed at study visits) during weeks 9, 10, 11, and 12, was nearly identical in the two studies. This Continuous Abstinence Rate was 44% in the varenicline groups. Each of the comparisons were statistically significant. Varenicline also showed significantly greater response rates vs.bupropion SR in these analyses. The studies above correspond to Study 4 and Study 5 in the Chantix full prescribing information. The most frequently reported adverse events (>10%) with Chantix were nausea, headache, insomnia, and abnormal dreams. Nausea was reported by approximately 30% of patients treated with Chantix 1 mg bid, with approximately a 3% discontinuation rate during 12 weeks of treatment. Nausea was generally described as mild or moderate and often transient. For some subjects, it was persistent over several months. Gonzales et al. Jorenby et al. Varenicline. Bupropion SR. Placebo. The 9-12 week Continuous Abstinence Rate is defined as the percentage of subjects who abstained from smoking (not even a puff) from Week 9 through 12 of the study as confirmed by both subject self-report and by end-expiratory carbon monoxide (CO) measurement. Chantix PI/ 13/1/¶1. Chantix PI/ 9/1/¶5. 1. Gonzalez D et al. JAMA. 2006;296: Jorenby DE et al. JAMA. 2006;296: References. Gonzalez D, Rennard SI, Billing CB, et al. Varenicline, an 42 Nicotinic Acetylcholine Receptor Partial Agonist, vs Sustained-Release Bupropion and Placebo for Smoking Cessation. JAMA. 2006;296: Jorenby DE, Hays JT, Rigotti MD, et al. Efficacy of Varenicline, an 42 Nicotinic Acetylcholine Receptor Partial Agonist, vs Placebo or Sustained-Release Bupropion for Smoking Cessation. JAMA. 2006;296: Chantix Prescribing Information. Pfizer Inc, New York, NY. (May 2006)")
66
Smoking is Cool….again

68
Prevention of smoking

69
THANK YOU!

Similar presentations
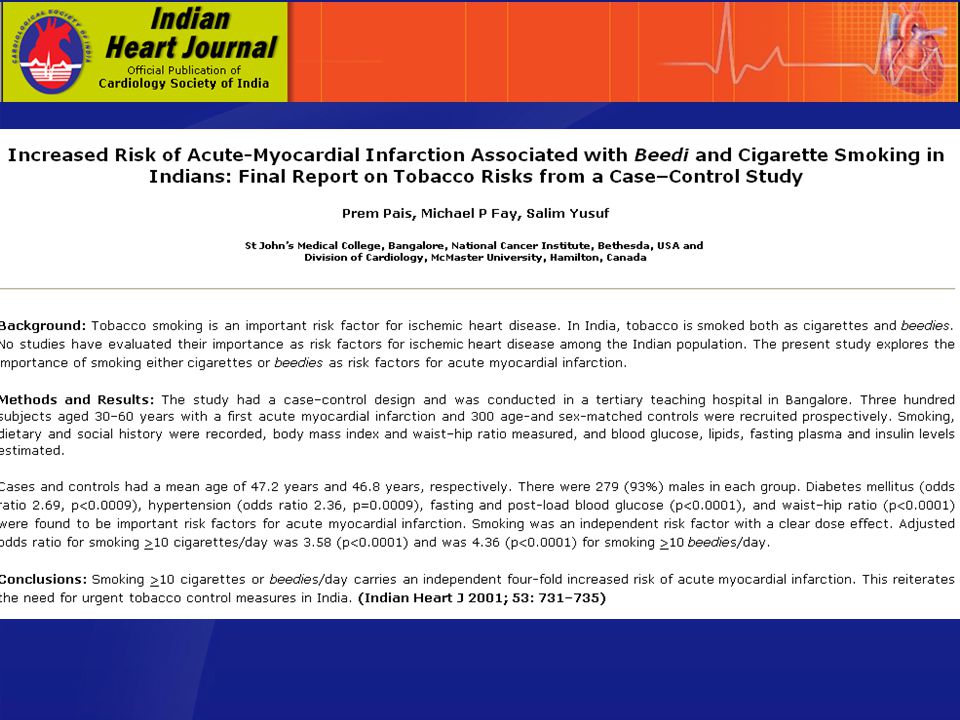
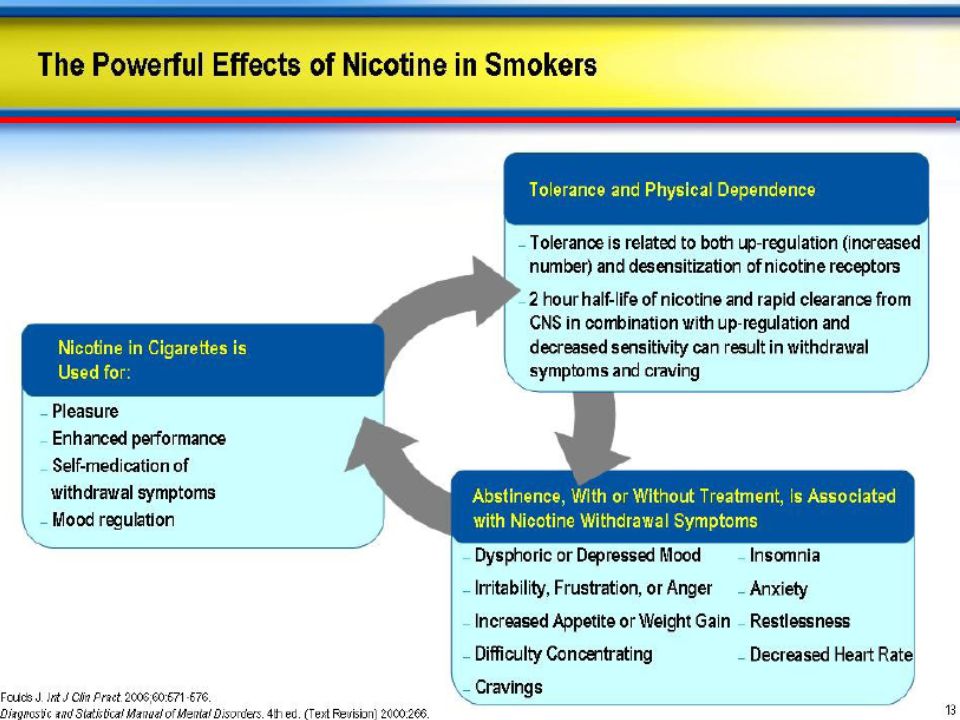


















 1920’s beginning of heavy marketing World War II Marlboro Man 1964 Smoking linked to cancer 1971 advertisements.>")

