Download presentation
Presentation is loading. Please wait.

1
Safe Prescribing Week 3 – Amino glycosides + electrolytes
Dr Ian Coombes, Senior Clinical Lecturer University of Queensland Schools of Medicine and Pharmacy Safe Medication Practice Unit, Queensland Health The University of Queensland

2
Objectives Principles of once daily Aminoglycoside dosing and avoiding toxicity Key messages about analgesia use This week we’re going to follow Mr AD, the man we first met in the medication history session (last week). I’m sure by now you’ll be familiar with some of the issues involved in prescribing. We’ll go over a few of these as a refresher before we discuss the pros and cons of using prescribing guidelines and where else you can source drug information. We will review the orders that you wrote up for Mr AD and discuss some strategies for ensuring that what you order is what is administered. We’ll demonstrate how to change doses of a drug that your patient is already on, as well as how to start a new medication. Our patient from last week will develop a pneumonia, which you will treat today. You will learn how to prescribe medications that require therapeutic drug monitoring and variable dosing, such as aminoglycosides (e.g. gentamicin). Aminoglycosides are one of the classes of drugs that interns and junior doctors classically report having problems with. As always, don’t be afraid to ask questions as we go along.
. I’m sure by now you’ll be familiar with some of the issues involved in prescribing. We’ll go over a few of these as a refresher before we discuss the pros and cons of using prescribing guidelines and where else you can source drug information. We will review the orders that you wrote up for Mr AD and discuss some strategies for ensuring that what you order is what is administered. We’ll demonstrate how to change doses of a drug that your patient is already on, as well as how to start a new medication. Our patient from last week will develop a pneumonia, which you will treat today. You will learn how to prescribe medications that require therapeutic drug monitoring and variable dosing, such as aminoglycosides (e.g. gentamicin). Aminoglycosides are one of the classes of drugs that interns and junior doctors classically report having problems with. As always, don’t be afraid to ask questions as we go along.")
3
Gentamicin Revision Gram negative bactericidal agent
Excellent anti-pseudomonal cover Once daily dosing benefits vs tds or bd: high peak level – excellent distribution post antibiotic effect (>24-36 hours) reduced monitoring and administration reduced nephro and ototoxicity easier monitoring (10-12 hours post dose) This slide gives a quick overview on gentamicin and some important key elements to consider. The next two slides are deliberately put AFTER the prescribing so that students can learn from their errors once already made (shock factor) Bactericidal efficacy is determined by the peak concentration and AUC of drug exposure, not by the time that the concentration exceeds the minimum inhibitory concentration. Nephrotoxicity and renal accumulation is reduced with higher doses administered less frequently. Not all forms of ototoxicity are reduced by this method.
 reduced monitoring and administration. reduced nephro and ototoxicity. easier monitoring (10-12 hours post dose) This slide gives a quick overview on gentamicin and some important key elements to consider. The next two slides are deliberately put AFTER the prescribing so that students can learn from their errors once already made (shock factor) Bactericidal efficacy is determined by the peak concentration and AUC of drug exposure, not by the time that the concentration exceeds the minimum inhibitory concentration. Nephrotoxicity and renal accumulation is reduced with higher doses administered less frequently. Not all forms of ototoxicity are reduced by this method.")
4
Severe risks of nephrotoxicity and ototoxicity
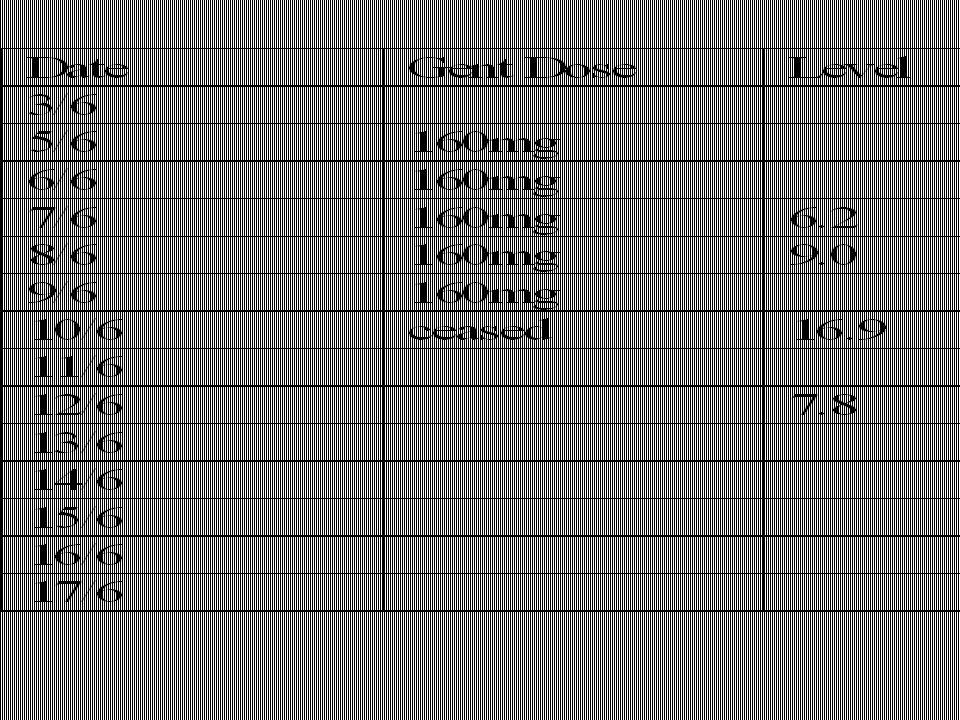
Mrs HR 78 years, wt 57kg Admitted to outlying hospital acute exacerbation COPD Baseline Cr 80mol/L Charted gentamicin 160mg daily for 5/7 CrCl = 45ml/min

7
21/6 Gent level still 1.4!!!! 23/6 complaining of dizziness, unsteady feeling, vestibular symptoms, vomiting 1/7 Cr 0.21 recovering

8
Aminoglycoside dosing and Monitoring
Case continued… Day 3: Mr AD (67yrs) has now developed sever hospital acquired pneumonia Ward round decisions start gentamicin once a day dose as per levels each night at 20:00 recall patient weighs 70 kg creatinine has improved (now 140 micro mole/l) start Co-Amoxiclav 1.2g IV q8h The scenario continues with our patient, who now has pneumonia. Participants should be asked to prescribe the patient Timentin® (Ticarcillin Sodium/Potassium Clavulanate) and gentamicin. NOTE: in this scenario, the patient has a penicillin allergy. Participants should not be alerted to this. If any student appears to want to ask about the penicillin allergy, politely ask them to write up both antibiotics as they see fit. If a student asks the facilitator individually, answer quietly rather than informing the group. Anecdotally, a large percentage of the group will not realise that they are prescribing a drug that will cause a serious life-threatening condition. The ‘shock-factor’ of this rings home the importance of checking for ADRs and allergies. To add realism to the situation, placing a time pressure and having the ‘consultant’ MO telling them to hurry up demonstrates how easy it is just to do what you’re told when under pressure – and yet how disastrous the consequences can be. Participants should initiate the gentamicin dose and then write up the second dose based on the level taken on day four (12 hours post dose). Participants should use either hospital dosing guidelines (if in use in your hospital) or alternatively, handouts from the antibiotic guidelines on gentamicin dosing. Once all the discussion is done, propose the scenario as an opportunity to practise graded assertiveness. Facilitator to pose as threatening consultant and ask how the students would approach the situation once they identified an issue. Remember PACE – probe, alert, challenge, emergency.
 has now developed sever hospital acquired pneumonia. Ward round decisions. start gentamicin once a day. dose as per levels each night at 20:00. recall patient weighs 70 kg. creatinine has improved (now 140 micro mole/l) start Co-Amoxiclav 1.2g IV q8h. The scenario continues with our patient, who now has pneumonia. Participants should be asked to prescribe the patient Timentin® (Ticarcillin Sodium/Potassium Clavulanate) and gentamicin. NOTE: in this scenario, the patient has a penicillin allergy. Participants should not be alerted to this. If any student appears to want to ask about the penicillin allergy, politely ask them to write up both antibiotics as they see fit. If a student asks the facilitator individually, answer quietly rather than informing the group. Anecdotally, a large percentage of the group will not realise that they are prescribing a drug that will cause a serious life-threatening condition. The ‘shock-factor’ of this rings home the importance of checking for ADRs and allergies. To add realism to the situation, placing a time pressure and having the ‘consultant’ MO telling them to hurry up demonstrates how easy it is just to do what you’re told when under pressure – and yet how disastrous the consequences can be. Participants should initiate the gentamicin dose and then write up the second dose based on the level taken on day four (12 hours post dose). Participants should use either hospital dosing guidelines (if in use in your hospital) or alternatively, handouts from the antibiotic guidelines on gentamicin dosing. Once all the discussion is done, propose the scenario as an opportunity to practise graded assertiveness. Facilitator to pose as threatening consultant and ask how the students would approach the situation once they identified an issue. Remember PACE – probe, alert, challenge, emergency.")
10
Creatinine Clearance CrCl ≈ 42 mL/min (140-67 X 70) / (0.814 x 140)
Do NOT use eGFR provided by AusLab (calculated using standard 70 kg patient can lead to over-dosing) Recall Cockcroft-Gault Formula: CrCl (mL/min) = [140-age (years)] * ideal weight (kg) [0.814 * serum creatinine (micromol/L)] {♀ * 0.85 } If patient 70 kg, 67 y.o. with serum creat~140micromol/L: CrCl ≈ 42 mL/min ( X 70) / (0.814 x 140) eGFR still not approved yet for DOSING (just a general guide to alert you of reduced renal function) Cockroft Gault is approved for dosing Available on AMH, TGs, local guides (eg PAH has it on poster and prescribing guidelines)
 Recall Cockcroft-Gault Formula: CrCl (mL/min) = [140-age (years)] * ideal weight (kg) [0.814 * serum creatinine (micromol/L)] {♀ * 0.85 } If patient 70 kg, 67 y.o. with serum creat~140micromol/L: CrCl ≈ 42 mL/min ( X 70) / (0.814 x 140) eGFR still not approved yet for DOSING (just a general guide to alert you of reduced renal function) Cockroft Gault is approved for dosing. Available on AMH, TGs, local guides (eg PAH has it on poster and prescribing guidelines)")
11
Ideal Body Weight male = 50kg + (0.9 * [ height (cm) – 152])
female = 45.5kg + (0.9 * [ height (cm) – 152]) or ideal weight = BMI 25 BMI = weight (kg) / [height (m)]2 ideal weight = 25 * [height (m)]2 height (cm) – 100 = weight (kg) The last method is the simplest and reasonably accurate for patients between 160cm – 190cm 160cm = 60kg = BMI approx 23.4 190cm = 90kg = BMI approx 24.9
![Ideal Body Weight male = 50kg + (0.9 * [ height (cm) – 152])](http://slideplayer.com/slide/3452603/12/images/11/Ideal+Body+Weight+male+%3D+50kg+%2B+%280.9+%2A+%5B+height+%28cm%29+%E2%80%93+152%5D%29.jpg "female = 45.5kg + (0.9 * [ height (cm) – 152]) or. ideal weight = BMI 25. BMI = weight (kg) / [height (m)]2. ideal weight = 25 * [height (m)]2. height (cm) – 100 = weight (kg) The last method is the simplest and reasonably accurate for patients between 160cm – 190cm. 160cm = 60kg = BMI approx cm = 90kg = BMI approx")
12
Calculating first dose gent

13
Gentamicin Dose Adjustment
Day 4: gentamicin level = 2.5 (taken 08:00, 12 hrs post dose) The initial dose given in emergency department was 280mg (4mg/kg x approx 70kg) Prescribe new gentamicin dose based on level Get students to use the guides/AMH/TG to help them
 The initial dose given in emergency department was 280mg (4mg/kg x approx 70kg) Prescribe new gentamicin dose based on level. Get students to use the guides/AMH/TG to help them.")
14
2.5

15
Adjusting doses of gentamicin

16
Gentamicin Dose Adjustment
Level at 12 hours = 2.5 (ideal = < 2) New Dose = Level Wanted (mg/L) x Dose Given (mg) Level Achieved (mg/L) In this case: (1.5/2.5) x 280 = 168 mg round down to 160 (nearest multiple of 40 mg) amps = 40 mg/mL Using AusLab, pressing Shift-Insert on the gentamicin level screen will show the blood level curve and dosing guidelines. To creatinine clearance, use the Cockroft-Gault formula (listed previously). Round your dosing and always round down. Ampoules come as 40mg/mL (2mL) and nurses will thank you for prescribing doses in quantities that are easy to measure out. Some patients require high doses (4-5mg/kg) to ensure adequate penetration to the site where it is needed. If they are poor at excreting the drug, they may need 48 hour dosing. If the dose you calculate for a patient (based on their gentamicin levels and renal function) is lower than 4mg/kg, it may be worth speaking to your consultant or registrar about whether the interval (rather than the dose) should be adjusted.
 New Dose = Level Wanted (mg/L) x Dose Given (mg) Level Achieved (mg/L) In this case: (1.5/2.5) x 280 = 168 mg. round down to 160 (nearest multiple of 40 mg) amps = 40 mg/mL. Using AusLab, pressing Shift-Insert on the gentamicin level screen will show the blood level curve and dosing guidelines. To creatinine clearance, use the Cockroft-Gault formula (listed previously). Round your dosing and always round down. Ampoules come as 40mg/mL (2mL) and nurses will thank you for prescribing doses in quantities that are easy to measure out. Some patients require high doses (4-5mg/kg) to ensure adequate penetration to the site where it is needed. If they are poor at excreting the drug, they may need 48 hour dosing. If the dose you calculate for a patient (based on their gentamicin levels and renal function) is lower than 4mg/kg, it may be worth speaking to your consultant or registrar about whether the interval (rather than the dose) should be adjusted.")
17
When NOT to take levels Do not take levels if: Stat dose Or
Patient has Normal renal function and is only receiving 1 or 2 doses ie prophylactic

18
Variable Dose Medication
Drug Level and Time Taken Variable dose medications are things such as gentamicin or prednisolone reducing doses, where the dose changes from day to day. Gentamicin dosing is a common ward call scenario that you will need to be familiar with. This is an example of how to write up gentamicin. Warfarin has its own separate place on the medication chart (we will cover this in a future session). Important things to note: Timing of dose (to fit in with blood levels). Different hospitals have different administration times, depending on blood collectors’ morning rounds. Check actual time dose was administered to accurately use dosing curve. Dose Time and Actual Time Given
. Important things to note: Timing of dose (to fit in with blood levels). Different hospitals have different administration times, depending on blood collectors’ morning rounds. Check actual time dose was administered to accurately use dosing curve. Dose Time and Actual Time Given.")
19
Use in moderate to sever renal function
Where ever possible withhold other nephrotoxic drugs and ensure no other altenative Ie unavoidable use of gentamicin: Requires extended dose intervals 36, 48 or 96 hours Effectively daily levels wait til < 1.0mmol/l then dose again

20
Gentamicin FAQs Patient returns from OT, septic, at 4 p.m.? dose now
get level 8 a.m. (difficult to get bloods during night) if level < 0.5, clearance satisfactory Patient in ED at 4 a.m. with severe pneumonia? give standard dose now; dose again at 8 p.m. Level low but adequate dose? (patient ok clinically) dose 4-5mg/kg has long post antibiotic effect don’t increase If in doubt, CHECK! Registrar; clinicial pharmacists; ID team If you are dosing at the recommended 4-5mg/kg and the patient’s levels come back below the therapeutic range, there is NO NEED to increase the dose. They are still getting the peak, they are just clearing the gentamicin faster.
 if level < 0.5, clearance satisfactory. Patient in ED at 4 a.m. with severe pneumonia give standard dose now; dose again at 8 p.m. Level low but adequate dose (patient ok clinically) dose 4-5mg/kg has long post antibiotic effect. don’t increase. If in doubt, CHECK! Registrar; clinicial pharmacists; ID team. If you are dosing at the recommended 4-5mg/kg and the patient’s levels come back below the therapeutic range, there is NO NEED to increase the dose. They are still getting the peak, they are just clearing the gentamicin faster.")
21
Gentamicin Ordering key messages
If elderly (renal impaired) is there an alternative safer drug? Do not write as a regular medication – prescribe dose for regular dosing after levels available Dose according to gentamicin level Use aminoglycoside dosing guides - these notes safe prescribing Try to prescribe in multiples of 40mg (ampoule contains 80mg/2mL = 40mg/mL) Where possible, dose at a time that allows level to be taken on next day’s blood round Some important considerations for dosing gentamicin: write in the variable dose section Try and use multiples of 40mg (80mg/2mL = 40mg/mL ampoules) use gentamicin guidelines (AMH, AUSLAB (once get levels back), therapeutic guidelines or hospital guidelines) (Note: Some hospitals have therapeutic drug monitoring services that will advise you on doses, monitoring and interpretation of results. You should check with your hospital if such a service exits.)
 is there an alternative safer drug Do not write as a regular medication – prescribe dose for regular dosing after levels available. Dose according to gentamicin level. Use aminoglycoside dosing guides. - these notes safe prescribing. Try to prescribe in multiples of 40mg (ampoule contains 80mg/2mL = 40mg/mL) Where possible, dose at a time that allows level to be taken on next day’s blood round. Some important considerations for dosing gentamicin: write in the variable dose section. Try and use multiples of 40mg (80mg/2mL = 40mg/mL ampoules) use gentamicin guidelines (AMH, AUSLAB (once get levels back), therapeutic guidelines or hospital guidelines) (Note: Some hospitals have therapeutic drug monitoring services that will advise you on doses, monitoring and interpretation of results. You should check with your hospital if such a service exits.)")
22
Questions?

23
Introduction to Prescribing Analgesia and Pain Relief
Presented by: [insert presenter name here] Disclaimer The materials presented in this publication are distributed by Queensland Health as an information source only. Queensland Health makes no statements, representations, or warranties about the accuracy or completeness of, and you should not rely on, any information contained in this publication. Despite our best efforts, Queensland Health makes no warranties that the information in this publication is free of infection by computer viruses or other contamination. Queensland Health disclaims all responsibility and liability (including without limitation, liability in negligence) for all expenses, losses, damages and costs you might incur as a result of the information being inaccurate or incomplete in any way, and for any reason. Copyright Queensland Health supports and encourages the dissemination and exchange of information. However, copyright protects this material. Queensland Health asserts the right to be recognised as author of this material and the right to have its material unaltered. Use of material published by Queensland Health should be in accord with the Copyright Act 1968. Endorsement This kit has been endorsed by the Safe Medication Practice Unit (SMPU) Board, Queensland Health Medication Safety Implementation Group (QHMSIG). Program Development: This program was originally developed by Ian Coombes as a component of his PhD studies and has been adapted by team members of the Safe Medication Practice Unit with permission. Editor This guide has been edited by Ian Coombes and Charles Mitchell, Key Contributors Ian Coombes, Charles Mitchell, Danielle Stowasser, Judith Coombes, Catherine Lucas and Jeremy Brammer. Safe Medication Practice Unit 23
 for all expenses, losses, damages and costs you might incur as a result of the information being inaccurate or incomplete in any way, and for any reason. Copyright. Queensland Health supports and encourages the dissemination and exchange of information. However, copyright protects this material. Queensland Health asserts the right to be recognised as author of this material and the right to have its material unaltered. Use of material published by Queensland Health should be in accord with the Copyright Act Endorsement. This kit has been endorsed by the Safe Medication Practice Unit (SMPU) Board, Queensland Health Medication Safety Implementation Group (QHMSIG). Program Development: This program was originally developed by Ian Coombes as a component of his PhD studies and has been adapted by team members of the Safe Medication Practice Unit with permission. Editor. This guide has been edited by Ian Coombes and Charles Mitchell, Key Contributors. Ian Coombes, Charles Mitchell, Danielle Stowasser, Judith Coombes, Catherine Lucas and Jeremy Brammer. Safe Medication Practice Unit. 23.")
24
You have been asked to write up a patient’s analgesia…
What patient factors do you need to consider? Prompt students to answer - What is the relevance to them as junior prescribers? You have the knowledge and want to show importance of recalling that knowledge in clinical situation Safe Medication Practice Unit 24

25
Goal to individualise analgesic therapy
Patient Assessment Goal to individualise analgesic therapy Assess patient characteristics: indication for analgesia age, sex, weight culture vital signs allergies/ADRs opioid tolerance respiratory status renal/hepatic function other medical co-morbidities mental state other Rx availability of oral/rectal routes In adults, age rather than weight is a better predictor of opioid requirements (although there is large inter-patient variation) Need to evaluate current analgesia (if applicable) - what patient was prescribed and what they are actually taking. Look for other sources of analgesia e.g. PCA, site perfusion devices etc. Titrate analgesia to patients needs – wide variability in patient response to pain (“emotional” experience) respiratory status (sleep apnoea, chronic lung disease) other Rx (e.g. antidepressants; analgesics; benzos) Safe Medication Practice Unit 25
 Need to evaluate current analgesia (if applicable) - what patient was prescribed and what they are actually taking. Look for other sources of analgesia e.g. PCA, site perfusion devices etc. Titrate analgesia to patients needs – wide variability in patient response to pain ( emotional experience) respiratory status (sleep apnoea, chronic lung disease) other Rx (e.g. antidepressants; analgesics; benzos) Safe Medication Practice Unit. 25.")
26
WHO Analgesic Ladder (ideally fro chronic pain)
Level 1: Non opioid/adjuvant (paracetamol; NSAIDs; amitriptyline; local anaesthetics) Level 2: Weak opioid + non-opioid Level 3: Strong opioid +/- non-opioid/adjuvant NOT ACCEPTED- Use Multimodal Analgesia Now not accepted –use multimodal analgesia Different pharmacological groups of analgesics: Non-opioid simple analgesics e.g. paracetamol NSAIDs muscle relaxants antispasmodics Weak opioids e.g. codeine Strong opioids e.g. morphine One opioid is not superior over others, but some opioids are better in some patients Safe Medication Practice Unit 26
 Level 2: Weak opioid + non-opioid. Level 3: Strong opioid +/- non-opioid/adjuvant NOT ACCEPTED- Use Multimodal Analgesia. Now not accepted –use multimodal analgesia. Different pharmacological groups of analgesics: Non-opioid simple analgesics e.g. paracetamol. NSAIDs. muscle relaxants. antispasmodics. Weak opioids e.g. codeine. Strong opioids e.g. morphine. One opioid is not superior over others, but some opioids are better in some patients. Safe Medication Practice Unit. 26.")
27
Inflammatory e.g. rheumatoid arthritis
DRUGS PAIN TYPE Nociceptive e.g. fracture Neuropathic eg neuralgia Inflammatory e.g. rheumatoid arthritis Paracetamol Effective when taken regularly at max. dose Less effective Effective, but not anti-inflammatory Opioids Effective May be effective (agent + dose) (depends on dose) NSAIDs Not effective TCAs, parenteral, local anaesthetics antiepileptic Rarely used (clonidine may be effective as adjunct) Rarely used (may be effective as adjunct) Adapted from Table 3-1, Australian Medicines Handbook Adapted from Table 3-1, Australian Medicines Handbook Different pharmacological groups of analgesics effective for different types of pain. Again, must take people through this in question and answer format. Safe Medication Practice Unit 27
 (depends on dose) NSAIDs. Not effective. TCAs, parenteral, local anaesthetics antiepileptic. Rarely used (clonidine may be effective as adjunct) Rarely used (may be effective as adjunct) Adapted from Table 3-1, Australian Medicines Handbook. Adapted from Table 3-1, Australian Medicines Handbook. Different pharmacological groups of analgesics effective for different types of pain. Again, must take people through this in question and answer format. Safe Medication Practice Unit. 27.")
28
NSAIDs- Adverse Effects
Side effects Cautions hypersensitivity/allergy GI (GORD/PUD) platelet inhibition sodium retention, oedema renal toxicity hepatic toxicity Platelet inhibition, but remember – COX-2 inhibitors INCREASE the risk of thrombotic events! GI bleeding/ulceration – risk NOT reduced by use of enteric coated or rectal dosage forms. Use a proton pump inhibitor to minimise risk of GORD/PUD Safe Medication Practice Unit 28
 platelet inhibition. sodium retention, oedema. renal toxicity. hepatic toxicity. Platelet inhibition, but remember – COX-2 inhibitors INCREASE the risk of thrombotic events! GI bleeding/ulceration – risk NOT reduced by use of enteric coated or rectal dosage forms. Use a proton pump inhibitor to minimise risk of GORD/PUD. Safe Medication Practice Unit. 28.")
29
NSAIDs- Adverse Effects
Side effects Cautions hypersensitivity/allergy asthma GI (GORD/PUD) GI bleeding/ulceration platelet inhibition coagulation disorders warfarin therapy sodium retention, oedema hypertension cardiac failure ACEI/ARA/diuretics renal toxicity renal impairment gentamicin therapy hepatic toxicity hepatic impairment Platelet inhibition, but remember – COX-2 inhibitors INCREASE the risk of thrombotic events! GI bleeding/ulceration – risk NOT reduced by use of enteric coated or rectal dosage forms. Use a proton pump inhibitor to minimise risk of GORD/PUD Safe Medication Practice Unit 29
 GI bleeding/ulceration. platelet inhibition. coagulation disorders. warfarin therapy. sodium retention, oedema. hypertension. cardiac failure. ACEI/ARA/diuretics. renal toxicity. renal impairment. gentamicin therapy. hepatic toxicity. hepatic impairment. Platelet inhibition, but remember – COX-2 inhibitors INCREASE the risk of thrombotic events! GI bleeding/ulceration – risk NOT reduced by use of enteric coated or rectal dosage forms. Use a proton pump inhibitor to minimise risk of GORD/PUD. Safe Medication Practice Unit. 29.")
30
NSAIDs – Caution! Major cause of ADEs and hospital admissions
use lowest effective dose for shortest possible time use paracetamol as alternative or to reduce NSAID dose COX-2 inhibitors similar adverse effects to non-selective increase risk of thrombotic events (stroke; MI)! little difference in efficacy between NSAIDs avoid aspirin < 18 yrs in viral illness (Reye’s syndrome) elderly - increased risk of adverse effects Continue only if effective. Avoid if possible! Little difference in efficacy between NSAIDs (choice depends on individual response and tolerance) children - no aspirin < 2 y.o. and avoid < 18 y.o. in viral illness (Reye’s syndrome) elderly - increased risk of adverse effects (esp. in heart failure, GI ulceration; renal impairment) Safe Medication Practice Unit 30
! little difference in efficacy between NSAIDs. avoid aspirin < 18 yrs in viral illness (Reye’s syndrome) elderly - increased risk of adverse effects. Continue only if effective. Avoid if possible! Little difference in efficacy between NSAIDs. (choice depends on individual response and tolerance) children - no aspirin < 2 y.o. and avoid < 18 y.o. in viral illness (Reye’s syndrome) elderly - increased risk of adverse effects (esp. in heart failure, GI ulceration; renal impairment) Safe Medication Practice Unit. 30.")
31
Potential Adverse Effects of Opioids?
Prompt the group. Safe Medication Practice Unit 31

32
Opioids – Adverse Effects
respiratory depression sedation nausea and vomiting confusion hypotension; bradycardia pruritus constipation / ∆ gut motility urinary retention Respiratory depression – major association with morbidity and mortality! ↑ airway resistance ↓ respiratory drive Avoid in acute/severe asthma Need to titrate opioid and give appropriate regular doses to avoid respiratory depression, which can occur at lower doses in patients with no pain. Respiratory centre receives nociceptive input, which counterbalances the respiratory depressant potential of the opioid. Absence of pain input leaves respiratory depressant effect of opioids unopposed e.g. need to reduce dose of regular opioid once patient has had a successful nerve block. Monitoring needs to continue for 24 hrs after epidural or intrathecal administration (chance of delayed respiratory depression). Sedation you will discuss this in a later slide can interfere with mobilisation and breathing.- Sedation always precedes respiratory depression, so it is important to monitor for excessive sedation. Nausea and vomiting Will discuss in later slides are caused by central mechanisms – stimulation of chemoreceptor trigger zone in medulla. Some patients develop tolerance to nausea and vomiting. Pain itself can cause nausea. Pruritis (itch), management on a later slide particularly with parenteral administration – not an allergy, rather, due to direct histamine release. Mainly occurs with morphine, particularly via the epidural route. Constipation Management on a later slide. occurs by central and peripheral mechanisms because of decreased intestinal motility and decreased GIT secretions. Tolerance develops slowly, if at all. All opioids at equianalgesic doses cause constipation. Urinary retention - caused by increased smooth muscle tone in urinary tract. Some pain is opioid insensitive, in that the dose of opioid required has intolerable side effects. Usually involves nerve compression and nerve destruction/neuropathic pain. Safe Medication Practice Unit 32 12
. Sedation you will discuss this in a later slide. can interfere with mobilisation and breathing.- Sedation always precedes respiratory depression, so it is important to monitor for excessive sedation. Nausea and vomiting Will discuss in later slides. are caused by central mechanisms – stimulation of chemoreceptor trigger zone in medulla. Some patients develop tolerance to nausea and vomiting. Pain itself can cause nausea. Pruritis (itch), management on a later slide particularly with parenteral administration – not an allergy, rather, due to direct histamine release. Mainly occurs with morphine, particularly via the epidural route. Constipation Management on a later slide. occurs by central and peripheral mechanisms because of decreased intestinal motility and decreased GIT secretions. Tolerance develops slowly, if at all. All opioids at equianalgesic doses cause constipation. Urinary retention - caused by increased smooth muscle tone in urinary tract. Some pain is opioid insensitive, in that the dose of opioid required has intolerable side effects. Usually involves nerve compression and nerve destruction/neuropathic pain. Safe Medication Practice Unit")
33
Opioids – Precautions hypotension, shock concomitant CNS depression
impaired respiration /↓ respiratory reserve elderly hepatic impairment renal impairment epilepsy/recognised seizure risk biliary colic or surgery phaeochromocytoma hypotension, shock —reduced blood volume increases hypotensive risk. impaired respiration/↓ respiratory reserve – respiratory depression. elderly; infants ≤ 12 months hypoxia; hypercapnia; cor pulmonale acute/severe asthma; COPD avoid opiates during acute asthma attack — opioids depress respiration and cough reflex and dry secretions elderly (increased risk of cognitive impairment and falls) - ↓ dose phaeochromocytoma - pressor response 2o to histamine release (no histamine release with fentanyl) hepatic impairment - severe hepatic disease may precipitate coma (↓ dose) renal impairment - active/toxic metabolites accumulate (↓ dose/use fentanyl or oxycodone) epilepsy/recognised seizure risk - increased risk of seizure head injury; metabolic disorders; EtOH/drug withdrawal; CNS infections; CNS depressants (eg. hypnotics) (CNS depression) biliary colic or surgery (spasm of sphincter of Oddi) Safe Medication Practice Unit 33 12
 - ↓ dose. phaeochromocytoma - pressor response 2o to histamine release (no histamine release with fentanyl) hepatic impairment - severe hepatic disease may precipitate coma (↓ dose) renal impairment - active/toxic metabolites accumulate (↓ dose/use fentanyl or oxycodone) epilepsy/recognised seizure risk - increased risk of seizure. head injury; metabolic disorders; EtOH/drug withdrawal; CNS infections; CNS depressants (eg. hypnotics) (CNS depression) biliary colic or surgery (spasm of sphincter of Oddi) Safe Medication Practice Unit")
34
Regular vs PRN Analgesia
regular analgesia is better in setting of continuous pain PRN only if pain intermittent and unpredictable in most settings, pain is predictable problems with using only PRN analgesia dose prescribed by Dr/administered by nurse patients don’t ask for medication inadequate or infrequent dosing → unrelieved pain keeping up with pain is easier than catching up with pain prn dose = 1/6 →1/12 total regular daily dose In acute pain setting, regular is preferred over just PRN. PRN prescribing is for when pain is possible but not predictable. In most post-op settings, pain is predictable. Regular analgesia should be given and then PRN analgesics can be used to manage breakthrough pain. A vicious cycle can occur if doctors don’t initially prescribing enough or adjust doses to individual patient needs: nurses give lower dose (if range prescribed) and less frequently, because PRN is translated as “when requested by patient”. patients don’t ask for medication because they don’t want to bother busy staff, so try to hold out. patients not regularly assessed for pain delays in administering analgesia promote anxiety in the patient and emotion is a part of the pain experience. Unfounded fears of giving too much/overdose or causing addiction. Evaluate PRN analgesic use and assess whether regular analgesia should be increased. Safe Medication Practice Unit 34 5
 and less frequently, because PRN is translated as when requested by patient . patients don’t ask for medication because they don’t want to bother busy staff, so try to hold out. patients not regularly assessed for pain. delays in administering analgesia promote anxiety in the patient and emotion is a part of the pain experience. Unfounded fears of giving too much/overdose or causing addiction. Evaluate PRN analgesic use and assess whether regular analgesia should be increased. Safe Medication Practice Unit")
35
Key Messages individualise analgesic therapy
choose analgesics judiciously use multimodal analgesia regular pain monitoring is critical to outcomes regularly review and revise analgesic doses adjust regular dose according to breakthrough usage anticipate and manage analgesic-associated adverse events avoid NSAIDs – major cause of morbidity/mortality! avoid tramadol, dextropropoxyphene, pethidine

36
Electrolyte Objectives
Fluid requirements Common error traps Electrolyte requirements Key messages for safe electrolyte prescribing The session will cover the following: fluid requirements for a “standard” patient monitoring of electrolyte levels The range of common IV fluids available to order common error traps in the ordering of fluids and electrolytes daily electrolyte requirements an opportunity to ask any questions around the material covered We encourage you to ask questions whenever you are not sure about something and we’ll do our best to provide you with a solution.

37
Maintenance Fluid for “Standard” Patient
70 kg euvolaemic no electrolyte derangements not septic normal cardiac and renal function no additional ongoing fluid losses Daily requirements are: ~ 2 mmol/kg sodium ~ 1 mmol/kg potassium, Hence, a 70kg patient will need in 24 hours: ~ 140 mmol NaCl ~ 70 mmol KCl 3L of 3.3% glucose and 0.3% NaCl will give 150 mmol of Na+; and adding 20 mmol of KCl to each bag will provide 60 mmol of K+ a day. Of course, modifications are necessary for patients who a fluid depleted or who have electrolyte derangements.

38
(Normal Saline) +/- 20/40 mmol KCl/l
Sodium Glucose Potassium Daily Requirement 2 mmol/kg >100G 1 mmol/kg 0.9% NaCl 1L (Normal Saline) +/- 20/40 mmol KCl/l 150 mmol 0, 20 or 40 mmol 4% glucose & 0.18% NaCl 1L 30 mmol 40G 3.3% glucose & 0.3% NaCl +/- 20/40 mmol KCl 1L 50 mmol 33G This chart compares three different fluids and demonstrates that for your ‘standard’ patient, three bags of 3 and 1/3 with 20 mmol KCl will provide the daily requirements of fluid, sodium, potassium and glucose.
 +/- 20/40 mmol KCl/l. 150 mmol. 0, 20 or 40 mmol. 4% glucose & 0.18% NaCl 1L. 30 mmol. 40G. 3.3% glucose & 0.3% NaCl +/- 20/40 mmol KCl 1L. 50 mmol. 33G. This chart compares three different fluids and demonstrates that for your ‘standard’ patient, three bags of 3 and 1/3 with 20 mmol KCl will provide the daily requirements of fluid, sodium, potassium and glucose.")
39
Risks of Having IV Line Infection Immobility Thrombophlebitis
Time and effort to re-site every 48 hours Immobility Thrombophlebitis Direct costs of consumables Overdosing of fluids and electrolytes What are the risks of having a line? Infection – change every 48 hours – time and effort to resite Immobility Thrombophlebitis Cost – consumables – PAH reported a 25% decrease in IV fluid use when changed to new IV fluid form where fluids had to be prescribed DAILY and only one bag was given per order Overdosing of fluids and electrolytes

40
Key Messages IV Fluid Ordering
Supply orally if possible Assess current fluid status wet / dry / ‘just right’? how do you tell? Review fluid balance chart Assess ongoing requirements and losses Reassess fluid status at least daily Before prescribing any fluids to a patient, you need to assess the patient’s fluid status using the various rough guides that we’ve discussed previously. You need to know if a patient is over-hydrated, under-hydrated or appropriately hydrated. This will guide you to how much fluid the patient needs (and will hopefully prevent you from making the patient worse). Think about whether IV fluids are the only way to rehydrate the patient. Is the oral route suitable? If the patient has already received fluids and you’ve been asked to review and write up additional fluids, you will need to look at what they have already received. Don’t assume that what they have been given is what they need. Look at ongoing fluid requirements and losses – for example drain sites, vomiting, diarrhoea, high fevers etc. QH policy only allows for no more than 24 hours of fluids to be written up. This is to ensure that the patient’s fluid status is reviewed at least daily. This is a bare minimum and if a patient has abnormal electrolytes or a significant fluid imbalance, it may be necessary to review more frequently (clinically +/- serum electrolytes), making adjustments as necessary.
. Think about whether IV fluids are the only way to rehydrate the patient. Is the oral route suitable If the patient has already received fluids and you’ve been asked to review and write up additional fluids, you will need to look at what they have already received. Don’t assume that what they have been given is what they need. Look at ongoing fluid requirements and losses – for example drain sites, vomiting, diarrhoea, high fevers etc. QH policy only allows for no more than 24 hours of fluids to be written up. This is to ensure that the patient’s fluid status is reviewed at least daily. This is a bare minimum and if a patient has abnormal electrolytes or a significant fluid imbalance, it may be necessary to review more frequently (clinically +/- serum electrolytes), making adjustments as necessary.")
41
Potassium What is normal? Where do you lose it from?
How much do you need? How can you replace it? Routes of administration? How fast can you replace it? Quantities? What goes wrong?

42
Potassium Normal serum K+ = 3.8-4.9 mmol/L
Daily requirement = 1 mmol/kg Dietary K+ < 25 mmol (1gram)/day leads to hypokalaemia Is magnesium low (< 0.5 mmol/L)? (makes it difficult to correct potassium) Normal range of serum K+: mmol/L (< 3.6 mmol/L considered hypokalaemia). ( for plasma) (Ref: AMH 2007) Apart from the usual 1 mmol/kg/d requirement and ongoing excess losses, you need to replace depleted potassium.
/day leads to hypokalaemia. Is magnesium low (< 0.5 mmol/L) (makes it difficult to correct potassium) Normal range of serum K+: mmol/L (< 3.6 mmol/L considered hypokalaemia). ( for plasma) (Ref: AMH 2007) Apart from the usual 1 mmol/kg/d requirement and ongoing excess losses, you need to replace depleted potassium.")
43
Causes of Hypokalaemia
Potential sites for K+ loss urine; faeces; drain sites; vomitus Intracellular shifts insulin β adrenoceptor agonists caffeine hyperthyroidism correction of acidosis Increased external losses Drugs that promote renal K+ excretion loop diuretics (eg frusemide) aldosterone; thiazides; penicillins Losses of potassium in the stool of mmol/L, however, when stools are normal and low in fluid, this is only about 10 mmol/day. Intracellular shifts Insulin and ß-adrenoceptor agonists both cause potassium to be taken up into the cells via Na+/K+ ATPase. Drugs such as ß2 sympathomimetics (e.g. salbutamol) cause intracellular shifts. A single initial dose of salbutamol can cause a drop of mmol/L drop in serum potassium and a second dose within the hour can reduce it by 1 mmol/L. Caffeine can cause a release of sympathetic amines and a few cups of coffee can drop the potassium by 0.4 mmol/L. Na+/K+ ATPase synthesis is stimulated by thyroid hormone, thus patients with hyperthyroidism may be prone to hypokalaemia. Acidosis results in K+ being exchanged for H+ as the H+ moves in to cells, thus increasing serum K+. The reverse occurs as acidosis is corrected; e.g. in recovery of diabetic keto-acidosis. Increased external losses aldosterone thiazide and loop diuretics (block chloride associated sodium resorption, increasing sodium to collecting ducts, where resorption causes potassium secretion) penicillin (and derivatives) in large doses can promote renal excretion by increasing sodium delivery to distal nephron
 aldosterone; thiazides; penicillins. Losses of potassium in the stool of mmol/L, however, when stools are normal and low in fluid, this is only about 10 mmol/day. Intracellular shifts. Insulin and ß-adrenoceptor agonists both cause potassium to be taken up into the cells via Na+/K+ ATPase. Drugs such as ß2 sympathomimetics (e.g. salbutamol) cause intracellular shifts. A single initial dose of salbutamol can cause a drop of mmol/L drop in serum potassium and a second dose within the hour can reduce it by 1 mmol/L. Caffeine can cause a release of sympathetic amines and a few cups of coffee can drop the potassium by 0.4 mmol/L. Na+/K+ ATPase synthesis is stimulated by thyroid hormone, thus patients with hyperthyroidism may be prone to hypokalaemia. Acidosis results in K+ being exchanged for H+ as the H+ moves in to cells, thus increasing serum K+. The reverse occurs as acidosis is corrected; e.g. in recovery of diabetic keto-acidosis. Increased external losses. aldosterone. thiazide and loop diuretics (block chloride associated sodium resorption, increasing sodium to collecting ducts, where resorption causes potassium secretion) penicillin (and derivatives) in large doses can promote renal excretion by increasing sodium delivery to distal nephron.")
44
Potassium Replacement
There is no single way to correct potassium serum K+ of 0.3 mmol/L = overall deficiency 100 mmol K+ (but extremely variable) Replace with oral supplements where possible Ideally, correction of potassium should occur over a period of days Account for deficit + ongoing normal requirements A decrease in serum potassium of 0.3 mmol/L indicates an overall deficiency of 100 mmol of potassium, BUT the response is extremely variable. (Ref: Gennari FJ. Hypokalemia. NEJM 1998;339(7):451-8) (nb. steady state – i.e. normal pH, no recent β agonists etc.) Correction of potassium should occur over a period of days (and err on the side of caution). Consider whether patients with low serum K+ have low magnesium. Low magnesium (i.e. Mg2+ < 0.5 mmol/L) makes it very difficult to correct low potassium. Important points to get across: Need to replace deficient potassium Need to account for ongoing normal requirements Rate and concentration should not be above the QH guidelines
 Replace with oral supplements where possible. Ideally, correction of potassium should occur over a period of days. Account for deficit + ongoing normal requirements. A decrease in serum potassium of 0.3 mmol/L indicates an overall deficiency of 100 mmol of potassium, BUT the response is extremely variable. (Ref: Gennari FJ. Hypokalemia. NEJM 1998;339(7):451-8) (nb. steady state – i.e. normal pH, no recent β agonists etc.) Correction of potassium should occur over a period of days (and err on the side of caution). Consider whether patients with low serum K+ have low magnesium. Low magnesium (i.e. Mg2+ < 0.5 mmol/L) makes it very difficult to correct low potassium. Important points to get across: Need to replace deficient potassium. Need to account for ongoing normal requirements. Rate and concentration should not be above the QH guidelines.")
45
Case Study - Mr KCl What happened? 72 y.o. ♂
Med Hx: hypertension, heart failure Rx: frusemide 80mg mane; lisinopril 10mg mane; amlodipine 10mg mane Admitted for elective TKR Pre-op serum potassium: 2.9 mmol/L Registrar: “Give him some IV KCl and fluids pre-op” suggests 40 mmol in 100mL N Sal over 60 min What happened? Ask participants what they think about this suggestion, and why. Concentration too high (no more than 40 mmol/L to prevent phlebitis) Maximum rate is 10 mmol/hr with a burette and 20 mmol/hr with infusion pump What are the alternatives? Students have received information in Module 1 about Graded Assertiveness. This is an ideal time to throw in another case vignette to let the students practise some of the skills they’ve learnt. P = probe A = alert C = challenge E = emergency
 Maximum rate is 10 mmol/hr with a burette and 20 mmol/hr with infusion pump. What are the alternatives Students have received information in Module 1 about Graded Assertiveness. This is an ideal time to throw in another case vignette to let the students practise some of the skills they’ve learnt. P = probe. A = alert. C = challenge. E = emergency.")
46
Potassium Administration
In non critical care cases, Should NOT give KCL > 10 mmol/hour WITHOUT a pump With a pump max. rate = 20 mmol/hour Concentrations > 40 mmol/L: risk causing thrombophlebitis, pain and loss of IV site If via central line, concentration NOT a concern, but RATE is! Why can you give a higher concentration with an infusion pump and not a gravity feed? Massive variation in gravity feed may lead to overdosing! Other problems with concentration include thrombophlebitis. Can overcome this using 100mL isotonic bags of 10 mmol potassium given with an infusion pump.

47
Causes of Hyperkalaemia
↓ K+ excretion (renal insufficiency) ↑ K+ intake (but rapid K+ excretion 2o to ↑ intake) K+ release from cells Metabolic acidoses Medications Hypoaldosteronism/resistance to aldosterone K+ release from cells pseudohyperkalemia - associated with venipuncture (tourniquet on for extended period of time; haemolysis) insulin deficiency and hyperglycaemia intravascular haemolysis; tumour lysis syndrome; rhabdomyolysis Medications K+ sparing diuretics e.g. spironolactone; amiloride; triamterene trimethoprim; heparin; ACEIs; ARAs; NSAIDs; cyclosporin digitalis toxicity (inhibition of Na+/K+ ATPase)
 ↑ K+ intake (but rapid K+ excretion 2o to ↑ intake) K+ release from cells. Metabolic acidoses. Medications. Hypoaldosteronism/resistance to aldosterone. K+ release from cells. pseudohyperkalemia - associated with venipuncture (tourniquet on for extended period of time; haemolysis) insulin deficiency and hyperglycaemia. intravascular haemolysis; tumour lysis syndrome; rhabdomyolysis. Medications. K+ sparing diuretics e.g. spironolactone; amiloride; triamterene. trimethoprim; heparin; ACEIs; ARAs; NSAIDs; cyclosporin. digitalis toxicity (inhibition of Na+/K+ ATPase)")
48
Managing Hyperkalaemia
What are your aims? What are the risks? What do you do? How do you do it?

49
Cardiovascular Protection
Calcium Gluconate by slow IV push decreases membrane excitability 10 mL of 10% calcium gluconate (2.2 mmol) onset 2-5 minutes, lasts up to an hour can repeat if no ∆ ECG after 5-10 minutes Additionally, cease potassium sparing drugs and restrict dietary potassium.
 onset 2-5 minutes, lasts up to an hour. can repeat if no ∆ ECG after 5-10 minutes. Additionally, cease potassium sparing drugs and restrict dietary potassium.")
50
Shift Intravascular → Intracellular
Insulin 10 units insulin in 50 mL of 50% glucose via syringe or free running drip onset minutes, lasts 1-3 hours ↓ plasma K+ by mmol/L Nebulised salbutamol 5 mg onset within 30 minutes, lasts 2-4 hours

51
Removing Excess Potassium
Resonium® A (sodium polystyrene sulfonate) promotes exchange of Na+ for K+ in the GIT 30g orally or 60g enema mixed with glucose onset within 2 hours, peak effect at 6 hours 1 gram binds 1 mmol K+ and releases 2-3 mmol Na+ generally lowers plasma K+ by mmol/L can give up to 4 doses per day (as per levels) Haemodialysis severe life-threatening hyperkalaemia unresponsive to more conservative measures
 promotes exchange of Na+ for K+ in the GIT. 30g orally or 60g enema mixed with glucose. onset within 2 hours, peak effect at 6 hours. 1 gram binds 1 mmol K+ and releases 2-3 mmol Na+ generally lowers plasma K+ by mmol/L. can give up to 4 doses per day (as per levels) Haemodialysis. severe life-threatening hyperkalaemia unresponsive to more conservative measures.")
52
Sodium Replacement Consider
? over filling (heart, renal, liver failure) ? over diuresis ? SIADH – SSRIs; TCAs; carbamazepine Replace Na+ gradually (↑ plasma Na+ by ≤ 10 mmol/L/day) Na+ required to ↑ plasma Na+ by 10 mmol/L: [0.6 * total body weight (kg)] * 10 = x mmol/L Na+ NEVER attempt to replace sodium with hypertonic saline! - IRREVERSIBLE osmotic demyelination of CNS (several cases in QLD in recent years) Hypertonic saline = 3% 0.6 * total body weight (kg) = total body water Hyponatraemia is more likely to be dilutional due to water excess as opposed to a depletion of body Na+. If euvolaemic or overloaded, then fluid restrict and give a diuretic. If hypovolaemic, add water and sodium (normal saline, NOT hypertonic). If there is SEVERE hyponatraemia (< 120 mmol/L), replace Na+ gradually (no more than 10mmol per day) to prevent osmotic demyelination. “Prescribing Intravenous Fluids and Electrolytes” should be at the end of all patient beds. Students should also receive a copy for this session.
 over diuresis. SIADH – SSRIs; TCAs; carbamazepine. Replace Na+ gradually (↑ plasma Na+ by ≤ 10 mmol/L/day) Na+ required to ↑ plasma Na+ by 10 mmol/L: [0.6 * total body weight (kg)] * 10 = x mmol/L Na+ NEVER attempt to replace sodium with hypertonic saline! - IRREVERSIBLE osmotic demyelination of CNS. (several cases in QLD in recent years) Hypertonic saline = 3% 0.6 * total body weight (kg) = total body water. Hyponatraemia is more likely to be dilutional due to water excess as opposed to a depletion of body Na+. If euvolaemic or overloaded, then fluid restrict and give a diuretic. If hypovolaemic, add water and sodium (normal saline, NOT hypertonic). If there is SEVERE hyponatraemia (< 120 mmol/L), replace Na+ gradually (no more than 10mmol per day) to prevent osmotic demyelination. Prescribing Intravenous Fluids and Electrolytes should be at the end of all patient beds. Students should also receive a copy for this session.")
53
Magnesium Indications hypomagnesaemia post MI antiarrythmic
acute asthma pre-eclampsia Oral - limited value (laxative) Be aware of IV rate - vasodilator! Summary from Harrison's Principles of Internal Medicine: Hypomagnesaemia Usually due to excess losses: vomiting, diarrhoea, surgical drainage or renal loss (cisplatin; cyclosporin; aminoglycosides) Patients usually asymptomatic when serum magnesium > 0.5 mmol/L May cause: Abnormalities in neuromuscular function Cardiac arrhythmias (e.g. sinus tachy; SVTs; ventricular arrhythmias) ECG abnormalities (prolonged PR or QT intervals, T-wave flattening or inversion and ST straightening) Consider the need for Ca2+, K+ and PO4- supplementation IV magnesium may worsen hypophosphatemia (via rapid stimulation of PTH secretion) - avoid by administering calcium with magnesium TREATMENT Mild, asymptomatic hypomagnesaemia may be treated with oral magnesium salts, mmol/day in divided doses (diarrhoea may occur with larger doses). More severe hypomagnesaemia should be treated with IV MgCl2 (MgSO4 may bind calcium and aggravate hypocalcaemia). Serum magnesium should be monitored at intervals of hours during therapy, which may continue for several days (impaired renal conservation of magnesium - only 50-70% of daily IV dose is retained.
 Be aware of IV rate - vasodilator! Summary from Harrison s Principles of Internal Medicine: Hypomagnesaemia. Usually due to excess losses: vomiting, diarrhoea, surgical drainage or renal loss (cisplatin; cyclosporin; aminoglycosides) Patients usually asymptomatic when serum magnesium > 0.5 mmol/L. May cause: Abnormalities in neuromuscular function. Cardiac arrhythmias (e.g. sinus tachy; SVTs; ventricular arrhythmias) ECG abnormalities (prolonged PR or QT intervals, T-wave flattening or inversion and ST straightening) Consider the need for Ca2+, K+ and PO4- supplementation. IV magnesium may worsen hypophosphatemia (via rapid stimulation of PTH secretion) - avoid by administering calcium with magnesium. TREATMENT. Mild, asymptomatic hypomagnesaemia may be treated with oral magnesium salts, mmol/day in divided doses (diarrhoea may occur with larger doses). More severe hypomagnesaemia should be treated with IV MgCl2 (MgSO4 may bind calcium and aggravate hypocalcaemia). Serum magnesium should be monitored at intervals of hours during therapy, which may continue for several days (impaired renal conservation of magnesium - only 50-70% of daily IV dose is retained.")
54
Key Messages Use oral route for electrolytes if possible
Significant patient harm 2° to rapid/concentrated KCl K+ reduction - protect heart (short and long term) NO place for hypertonic saline – demyelenitaion risk Magnesium used for hypertension
 NO place for hypertonic saline – demyelenitaion risk. Magnesium used for hypertension.")
55
Questions?

Similar presentations






? CKD stages 1-V How common is it? Creatinine v GFR Basic Principles Scenarios.>")













