Download presentation
Presentation is loading. Please wait.

1
Medicine For Mariners “101”
Robin B. Garelick, MD, FACEP SV Quantum Leap

2
Objectives Learn and Have Fun Common Medical Conditions
Seasickness Hypothermia Hyperthermia Sunburn Trauma Marine Evenomation Wound Care Customizing a Medical Kit Basic First Aid Tips Future Topics and Workshops ?

3
Mal de Mer “Seasickness”
AKA: Motion Sickness

5
Seasickness Throughout the world, it is the most frequent medical problem responsible for maritime search and rescue. Primarily during stormy weather. Can cause a lack of will to persevere in stormy weather and rough seas. “Wet, seasick and scared - they want to go home”.

6
Seasickness can cause…
Mental Deterioration Physical Deterioration Progressive Dehydration Loss of Manual Dexterity Ataxia (walk like you’re drunk!) Impaired Judgment After several hours of illness - loss of will to survive Fatalities due to poor seamanship & complications during emergency evacuation
 Impaired Judgment. After several hours of illness - loss of will to survive. Fatalities due to poor seamanship & complications during emergency evacuation.")
7
What does seasickness look like ?

11
Basic Underlying Mechanism of Seasickness
Your body, inner ear and eyes all send different signals to the brain. A disturbance occurs in the inner ear. Fluid within the vestibular system shifts in relationship to position. Position sensors in our muscles and joints send signals to the brain based upon our movements. Our eyes may have a fixed position when below deck or trying to read. Neural mismatch occurs while we are in motion.

13
The inner ear & it’s 3 canals
Semicircular Canals Purpose of canals is so we stay balanced and live in 3D world 3 Planes of Space Up-Down Left-Right Front-Back

14
The anatomy of motion sensors…
Canals are lined with haircells. The fluid in the canals is called endolymph. The haircells are our motion sensors and when the endolymph moves - a message is sent to our brain.

15
The neural mismatch Dopamine (neurotransmitter) is released and triggers a chemoreceptor zone in the brain which activates our “vomit” center. Initial response to the neural mismatch occurs at the brainstem level. So how do we prevent this or blunt the response???? AKA: How to get your sea legs.

16
Getting your sea legs… Occurs over 24 to 72 hours.
For many - the brain learns to compensate over time and you accommodate. Medication prevents symptoms but may not completely reverse once they occur. After a prolonged period of time at sea the reverse occurs as you get used to being on land.

17
Signs and Symptoms Sleepiness and excess yawning
Nausea (stay positive and tell yourself you won’t vomit) Extreme Nausea and Vomiting Dizziness Headache Pallor Cold Sweats Depression Lack of interest
 Extreme Nausea and Vomiting. Dizziness. Headache. Pallor. Cold Sweats. Depression. Lack of interest.")
18
Seasickness Triggers Going below deck for extended periods of time while underway. Looking through binoculars for extended periods of time (stabilizing binoculars). Reading a book, focusing on compass, detailed work or staring at one point. Keep peripheral vision on the horizon and not staring at an object your brain will interpret as stable because your semicircular canals are screaming motion.
. Reading a book, focusing on compass, detailed work or staring at one point. Keep peripheral vision on the horizon and not staring at an object your brain will interpret as stable because your semicircular canals are screaming motion.")
20
Preventative Measures
Avoid alcohol. Get plenty of rest before departing. Drink plenty of water and stay hydrated. Avoid heavy foods and fatty meals while underway. Consider seasickness aids. Ginger Homeopathics Accupressure/Seasickness Bands

21
Medications for Seasickness
Antihistamines: Meclizine (Bonine, Non -drowsy Dramamine) Cyclizine (Marazine) Diphenhydramine (Benedryl) Cinnarizine (Stugeron) Anticholinergics: Scopolamine (Transderm-Scop) Antiemetics Promethazine (Phenergan tablet or suppository) Prochlorperazine (Compazine) Metoclopramide (Reglan) Odansetron (Zofran)
 Cyclizine (Marazine) Diphenhydramine (Benedryl) Cinnarizine (Stugeron) Anticholinergics: Scopolamine (Transderm-Scop) Antiemetics. Promethazine (Phenergan tablet or suppository) Prochlorperazine (Compazine) Metoclopramide (Reglan) Odansetron (Zofran)")
22
Side Effects of Medications
Antihistamines & Anticholinergics: Sedation/Drowsiness Dry Mouth Blurred Vision Serotonin Receptor Antagonists: Headache Fatigue/Malaise Antiemetics (except Odansetron/Zofran): Akasthesis/Dystonia Sedation
: Akasthesis/Dystonia. Sedation.")
23
Hypothermia AKA: I’m Cold
Primary & Secondary Hypothermia Primary: Cold Exposure Secondary: Medical Conditions or Medications that prevent response to cold or predispose to heat loss. Immersion (Man overboard!!!!) Acute versus Chronic
 Acute versus Chronic.")
24
Hypothermia Defined Mild Hypothermia: core temperature below 95o to 89.6o. Moderate Hypothermia: core temperature below 89.6o to 82.4o. Severe Hypothermia: core temperature less than 82.4o. We set 86o as the CRITICAL Temperature. Mild and early moderate hypothermia are treatable without emergency medical intervention & rescue.

25
Acute vs.Chronic Hypothermia
Thermal Conductivity of water: 25 times greater than air. Acute Hypothermia develops in minutes to hours after sudden immersion in cold water. Chronic Hypothermia develops over hours to days when inadequate protection from cold wind and wet spray.

26
Predictable Rate of Cooling
Based on water temperature Body shape (short round bodies cool slower than tall thin bodies). Insulating fat layers (finally an advantage to having more sub-q fat). If immersed - activity during immersion (less is better). Amount of body immersed. Protective clothing being worn.
. Insulating fat layers (finally an advantage to having more sub-q fat). If immersed - activity during immersion (less is better). Amount of body immersed. Protective clothing being worn.")
27
How do we preserve heat ? Divert warm blood from the surface to our core. skin and muscles to the brain, heart, lungs, kidney and liver. The decrease in surface blood flow improves insulation Shivering occurs to produce heat by increasing metabolic activity. Max shivering at 89.6o to 91.6o. Hypothermia develops when heat loss exceeds heat conservation. Muscle rigidity occurs at 86o.Voluntary shivering stops with we are unable to rewarm ourself.

28
Signs and Symptoms Clumsiness in activity.
Difficulty walking (especially with heavy gear or clothing). Subtle changes in mental status which impair judgment (confusion and disorientation). Decreased responsiveness to verbal and painful stimuli. Coma and unconscious state in severe hypothermia.
. Subtle changes in mental status which impair judgment (confusion and disorientation). Decreased responsiveness to verbal and painful stimuli. Coma and unconscious state in severe hypothermia.")
30
Treatment of Hypothermia
Initial treatment in mild hypothermia: Take shelter from wind and water. Replace wet clothing with multiple layers of dry insulated garments that make the skin feel dry. If no dry clothing then add an extra layer of foul weather gear. Wrap in blankets, sleeping bag, sail or sailbags. Feed simple carbs and light sweet beverages (warm preferred) Allow shivering to continue for self rewarming. In moderate to severe hypothermia - evacuation is required for emergency medical intervention.
 Allow shivering to continue for self rewarming. In moderate to severe hypothermia - evacuation is required for emergency medical intervention.")
31
Treatment of Hypothermia
In moderate to severe hypothermia: Heart can be stunned into ventricular fibrillation - therefore handle the victim gently. Lay victim flat. External hot packs to the armpits, groin, chest wall and neck to stabilize body temperature. Cuddle to help stabilize their body temperature. Cough and gag reflexes are diminished - do not try to give hot liquids or food.

32
Remember to keep them bundled and protected from cold.
Helicopter rescue may incur winds of 100 mph from prop downwash and increase wind-chill for the hypothermic victim.

34
Survival Gear

36
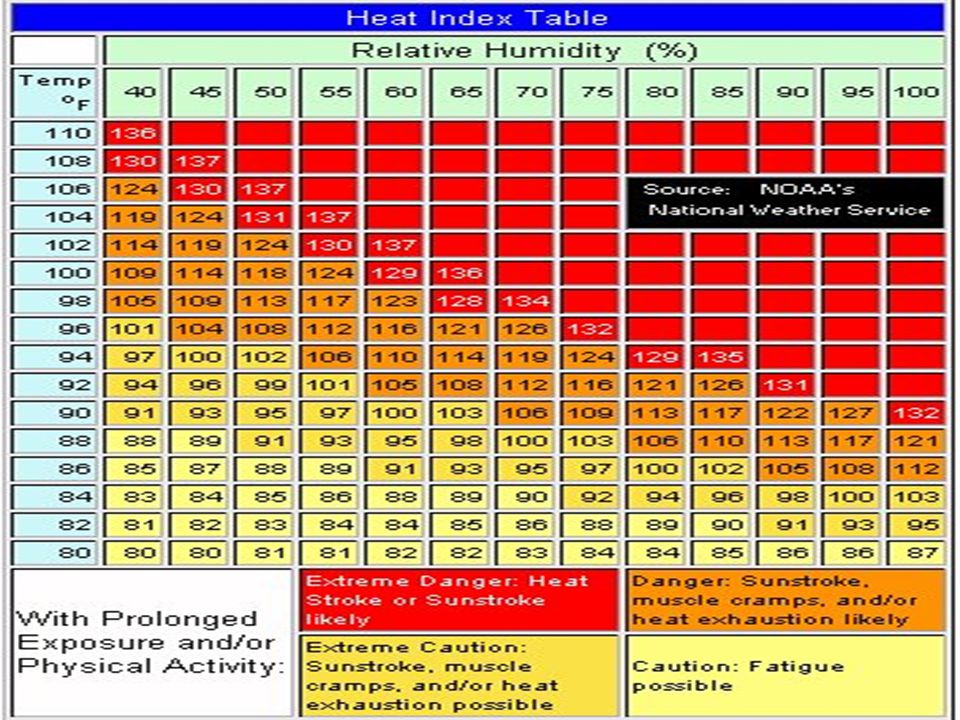
Hyperthermia AKA: I’m hot
Definition: A medical condition arising when the body’s capacity to lose heat does not match the total body heat load. Occurs when a normal physiologic response becomes pathophysiologic (body temperature > than the brain set point).
.")
37
Types of Heat Illness Heat Rash: rash caused by plugged sweat glands and we get a secondary inflammatory reaction. Heat Edema: self limited swelling of the hands and feet seen early in heat exposure. Heat Cramps: muscle cramps associated with exercise and secondary to loss of sodium. Heat Syncope: fainting from dilatation of the surface blood vessels from high temperature. Heat Exhaustion: Loss of circulating volume in the face of heat stress.

39
Types of Heat Illness Heat Stroke: complex clinical condition characterized by: Core temperature of 104o to 106o. Neurologic Changes (aka: change in mental status) Multiorgan dysfunction can occur - breakdown in ability of kidneys and heart to function within normal limits.
 Multiorgan dysfunction can occur - breakdown in ability of kidneys and heart to function within normal limits.")
40
How do we lose heat ? Radiation: 65% of heat loss
Conduction: < 2% of heat loss (increases when immersed in water) Convection: 10% of heat loss Respiration/Breathing: 5% of heat loss Evaporation: 35% at rest and up to 75% of heat loss with activity. Most effective means of heat loss BUT at 95% humidity, evaporation no longer occurs.
 Convection: 10% of heat loss. Respiration/Breathing: 5% of heat loss. Evaporation: 35% at rest and up to 75% of heat loss with activity. Most effective means of heat loss BUT at 95% humidity, evaporation no longer occurs.")
41
Factors that Predispose us to Hyperthermia
Prolonged exertion Poor muscle conditioning Inability to acclimate to the temperature Sleep deprivation Disease states Cardiac, dehydration, endocrine disorders, skin disorders, infections, seizures, etc.

42
Factors that Predispose to Hyperthermia
Rapid change in humidity or temperature Heavy and/or constrictive clothing Extremes of age - the very young and the very old… Medications & Drugs Anticholinergics: TCA’s and Phenothiazines Amphetamines & Cocaine Diuretics (water pills) Alcohol Beta Blockers (drugs that end in -ol) Alpha agonists
 Alcohol. Beta Blockers (drugs that end in -ol) Alpha agonists.")
43
Signs and Symptoms of Heat Exhaustion
Malaise Weakness (low blood pressure) Headache Decreased Appetite Nausea/Vomiting Increased heart rate Profuse sweating
 Headache. Decreased Appetite. Nausea/Vomiting. Increased heart rate. Profuse sweating.")
44
Heat Stroke True Medical Emergency that requires rapid cooling measures: While awaiting assistance - remove excess clothing. Try cooling methods such as body misting, fan, cool wet sheets r ice packs to the groin, axilla, neck and chest area. Rapid cooling improves survival.

46
Treatment of Hyperthermia
Hydration, hydration, hydration!!! “If you can read the newspaper through your urine - you’re well hydrated.” Electrolyte drinks like Gatorade or Powerade (avoid salt tablets). Avoiding excess heat with medication/medical conditions that predispose to heat illness. Decrease alcohol consumption. Minimize sun exposure. Avoid sleep deprivation. Decrease outdoor activity/exercise routines and shift to an indoor environment.
. Avoiding excess heat with medication/medical conditions that predispose to heat illness. Decrease alcohol consumption. Minimize sun exposure. Avoid sleep deprivation. Decrease outdoor activity/exercise routines and shift to an indoor environment.")
47
Treatment of Hyperthermia
Avoid sleep deprivation. Decrease outdoor activity/exercise routine and shift to indoor environment. Cold showers/transom shower/anchor washdown. If going to a hot climate - acclimate slowly over a period of 1 to 2 weeks.

48
Sunburn and Solar Injury
Sunburn is classified as a thermal injury. Red, hot painful 1st degree burns show up 2 to 6 hours after exposure. 2nd degree burns occur when there is swelling, blisters and subsequent peeling.

51
Sunburn Prevention Schedule water activities (when possible) in early morning or late afternoon hours. Chemical sunscreens (PABA) absorb UV rays and require application at least 30 to 60 minutes prior to sun exposure so they can penetrate the deep layers of the skin. Physical sunscreen (zinc oxide) act as physical shields and reflect or scatter light. They are effective immediately. Use on high exposure areas: lips. ears, facial areas.
 absorb UV rays and require application at least 30 to 60 minutes prior to sun exposure so they can penetrate the deep layers of the skin. Physical sunscreen (zinc oxide) act as physical shields and reflect or scatter light. They are effective immediately. Use on high exposure areas: lips. ears, facial areas.")
52
Sunburn Prevention Reapply liberally every 2 to 3 hours and more frequently if in and out of the water or excess perspiration. Waterproof formulations last 2X longer than water resistant formulations. Consider UV block clothing and hats that cover sensitive areas (face/ears/neck/scalp)
")
53
Sun Related Eye Injuries
Excess UV Radiation can lead to cataracts and damage to the retina. Photokeratitis is a “sunburn” type injury to the cornea: Intense eye pain Increased tearing & redness Spasm of the eye itself as well as the lid

54
Sun Related Eye Injuries
Pain & temporary loss of vision starts in 4 to 12 hours. Treatment is with antibiotic ointment or solution. Bacitracin Ophthalmic Ointment Polytrim Eye Drops Cipro Eye Drops (Contact lens wearer) Avoid bright light after a photosensitivity injury (24 hours). Pain medication Sunglasses that block UVA & UVB with a wide brimmed hat.
 Avoid bright light after a photosensitivity injury (24 hours). Pain medication. Sunglasses that block UVA & UVB with a wide brimmed hat.")
55
Photosensitivity Reactions
Exagerrated sunburn or rashes triggered by sun exposure after taking a particular medication or applying a chemicla or plant extract to the skin. Burn appears immediately and lasts up to 2 to 4 days. May get hives or poison ivy type rash.

56
Treatment of Photosensitivity Reactions
Mild: treat like you would a sunburn. Moderate to Severe: May require prednisone (steroids). Pain medication Remove offending agent (if not a required medication) Stay out of the sun Use sunblock frequently and generously. Read the label on all medications and check manufacturer websites.
. Pain medication. Remove offending agent (if not a required medication) Stay out of the sun. Use sunblock frequently and generously. Read the label on all medications and check manufacturer websites.")
57
Sun Poisoning Severe reaction after intense sun exposure.
Fever & Chills Headache Nausea & Vomiting Dehydration and may experience altered mental status if the blood pressure falls Treatment is the same as heat exhaustion with the addition of prednisone for the most severe reactions.

58
Drugs that Cause Photosensitivity Reactions
Antibiotics: Cyclines Flouroquinolones (Cipro, Levaquin, Avelox) Bactrim/Sulfonamides Nalidixic Acid Antihistamines Antiparasitics Antihypertensives Captopril Diltiazem Nifedipine
 Bactrim/Sulfonamides. Nalidixic Acid. Antihistamines. Antiparasitics. Antihypertensives. Captopril. Diltiazem. Nifedipine.")
59
Drugs that Cause Photosensitivity Reactions
Anti-Inflammatory Motrin/Ibuprophen Indocin Naprosyn Piroxicanm (Feldene) Diuretics Diamox HCTZ Lasix/Furosemide Trimaterene (Maxzide) Miscellaneous Benzocine Benzoyl Peroxide OCP Topical Cortisone Amiodarone Xanax Retin-A/Accutane Hypoglycemics Glipizide Glyburide Tolbutamide (Orinase)
 Diuretics. Diamox. HCTZ. Lasix/Furosemide. Trimaterene (Maxzide) Miscellaneous. Benzocine. Benzoyl Peroxide. OCP. Topical Cortisone. Amiodarone. Xanax. Retin-A/Accutane. Hypoglycemics. Glipizide. Glyburide. Tolbutamide (Orinase)")
60
Sunscreens that Cause Photosensitivity
Preps containing the following: Aminobenzoic Acid Avobenzone Benzophenones Cinnamates Homosalate Methyl Anthranilate PABA Esters

61
Treatment of Sunburn Cool wet compresses for 15 to 20 minutes every hour. Frequent cool showers or duse with cold sea water. Pain medication (Ibuprophen, narcotic analgesics). Topical aloe vera gel for comfort and healing. Antibacterial Ointment Lidocaine jelly or anesthetic sunburn spray. Leave blisters intact as your own body fluid & skin are a natural barrier and promote healing.
. Topical aloe vera gel for comfort and healing. Antibacterial Ointment. Lidocaine jelly or anesthetic sunburn spray. Leave blisters intact as your own body fluid & skin are a natural barrier and promote healing.")
62
Perfumes, Lotions and Cosmetics that Cause Photosensitivity
Bergamot Oil Oil of Citron, Lavendar, Cedar, Lime, Sandalwood, Citrus Rind Oils and 6-methylcoumarin Hexachlorophene (Phisohex, etc.)
")
63
Trauma 101 Sprains, strains, fractures, contusions, dislocations…..
All bets are off out to sea! Chest and head trauma are the most common injuries for recreational boaters. Head Injuries include both blunt and penetrating trauma. Chest injuries include both blunt and penetrating trauma

64
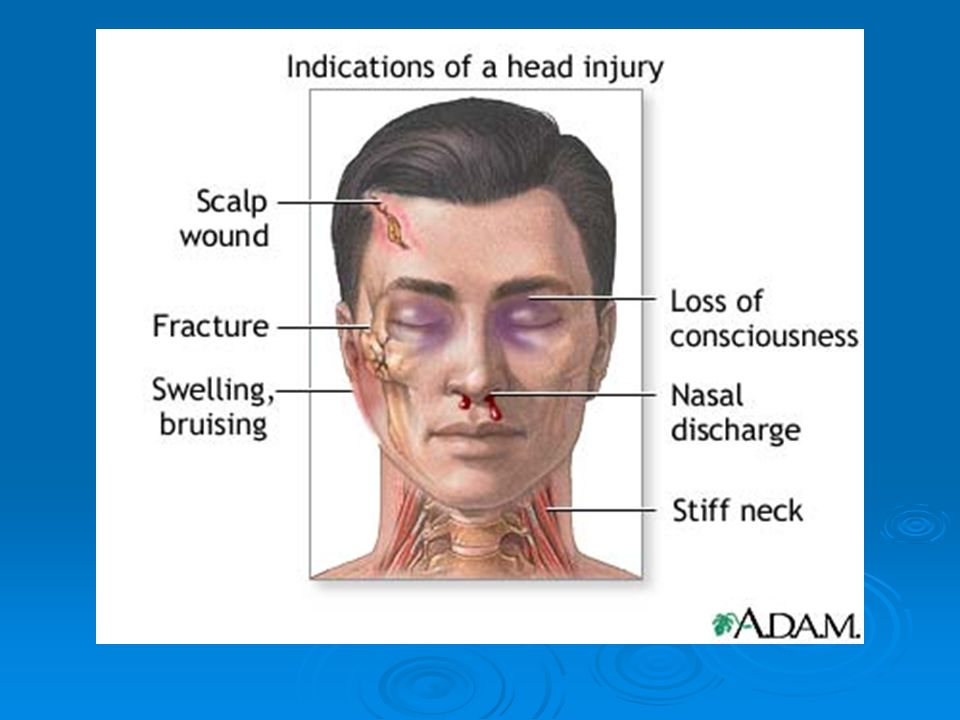
Head Injuries Falls, hit in the head with flying objects and naturally the “boom” . Cuts to the face and scalp. Blunt trauma to facial bones. Nose bleeds secondary to facial trauma.

66
What to look for with a head injury
Was there a loss of consciousness (+LOC)? Is amnesia present? Do they have normal speech, mentation and are they moving all extrmities? Is there a complaint of numbness or tingling in an arm or leg? Is there nausea/vomiting? Is there a complaint of blurry vision?
 Is amnesia present Do they have normal speech, mentation and are they moving all extrmities Is there a complaint of numbness or tingling in an arm or leg Is there nausea/vomiting Is there a complaint of blurry vision")
67
Ouch!!!!!

69
Treatment of Head Injuries
If there is neurological abnormality - immediate evacuation with emergency medical attention. Prolonged loss of consciousness Numb/Tingle in extremities or an inabilty to use an extremity without signs of a broken bone Remember to try and immobilize the neck

70
Treatment of Head Injuries
If there is a brief LOC then it may be safe to remain onboard and observe carefully for the next 24 hours. Signs of a more severe injury include: Nausea/Vomiting Vision Changes Dizziness Change in speech Change in mentation

71
Chest Injuries Most are from blunt force: Can cause rib fractures.
If ribs are fractured then make sure the injured person can breath comfortably as they are at risk of puncturing their lung from a broken rib.

72
What does the rib cage look like ?

73
Examination of the Chest Wall
Expose the area to look for any open wounds. Feel along the chest wall front and back to see if there are “rice crispies”. Feel the breast bone for tenderness. Look for any deformity of the collar bones. Watch the breathing pattern - is it regular or short and gasping?

74
Treatment of Chest Injuries
Pain medication. Ice bruised areas found when you examine the chest. Duck tape??? Monitor for any changes in breathing and pain increase with inspiration (taking a breath).
.")
75
Sprains, Strains, Fractures & Dislocations
RICE: rest, ice, compression and elevation. Pain Medication If a bone appears deformed - splint in anatomically and place in a position of comfort. If severe deformity then medical attention is required. Blood loss can happen with long bone fractures. Nerve injuries can occur with dislocations and fractures - if not treated in a timely manner. Not sure then summon help.

76
Sam Splint - My Personal Favorite

77
Sam Body

78
Sam User Guide

79
Other SAM Products

80
Marine Evenomation The Jellyfish Sting
Reactions vary b the type of jelly fish, venom potency and the amount injected. Symptoms vary from burning to itching to excruciating pain. Anaphylaxis with difficulty breathing, drop in blood pressure and shock.

81
Treatment of Jellyfish Sting
Apply vinegar (Acetic Acid 5%) immediately to inactivate the venom. If vinegar is not available use sea water. NEVER rinse with fresh water or apply ice directly to the skin as it will activate stinging cells and increase pain/reaction. If eyes are involved irrigate immediately with saline or sea water.
 immediately to inactivate the venom. If vinegar is not available use sea water. NEVER rinse with fresh water or apply ice directly to the skin as it will activate stinging cells and increase pain/reaction. If eyes are involved irrigate immediately with saline or sea water.")
82
Treatment of Jellyfish Sting
Rubbing alcohol and vinegar can help with pain over the first hour. Baking soda paste provides relief. 1/4 strength household ammonia may help. Limited usefulness of meat tenderizer. Remove embedded particles or tentacles with a tweezer. Wear protective gloves. You can also apply shave cream and shave the skin gently. Hydrocortisone Cream Prednisone and Benedryl If stung on the mouth - watch for swelling.

83
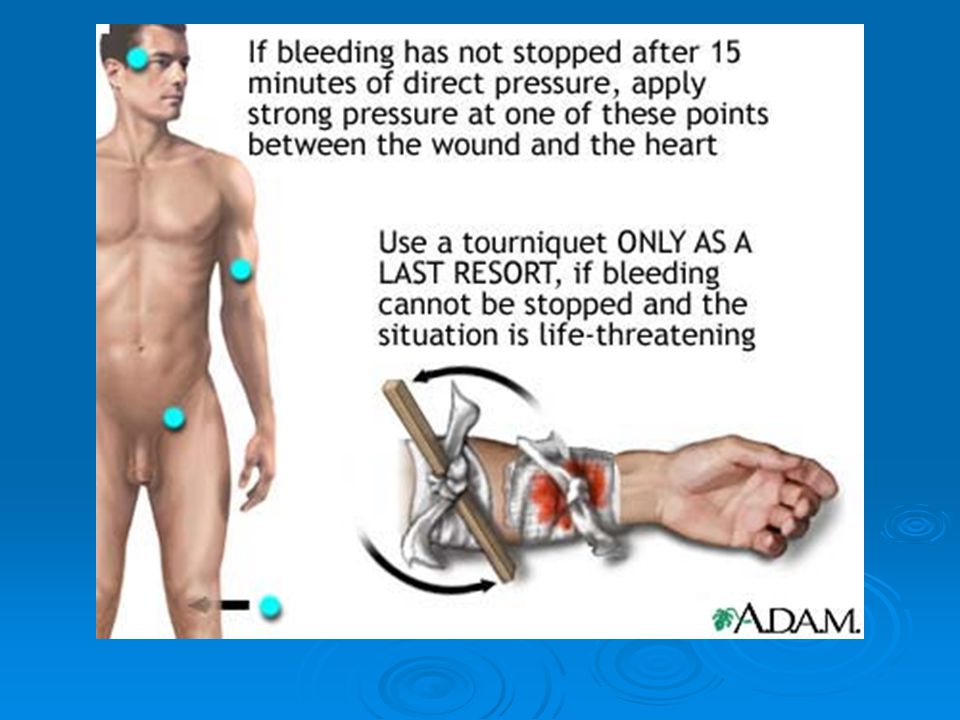
Wound Care All bleeding stops with pressure.
Apply direct pressure over the wound for 15 minutes and elevate the affected body part. Neck wounds - pinch the area instead of pressure.

86
Wound Care Clean wounds with saline or fresh water kept onboard specifically for wound care (boiled and stored). Alcohol and Hydrogen Peroxide applied full strength can be toxic to tissues. “If you can’t put it in your eye then don’t put it in your wounds”. Other wound care information

87
Methods of Wound Closure
Bandaid Butterfly Bandaid Steristrips Occlusive Dressing Skin Glue Staples (surgical staples) Sutures
 Sutures.")
88
Checking the Wound Monitor carefully for signs of infection and age appropriate healing. Pus draining from wound Pain, redness and swelling Fever and Chills Swollen tender lymph nodes Red streaking in the affected area

89
Choosing Your Medical Kit
Based on how far you will travel and your health history. Easy to stow and easily accessible to all onboard. Basic supplies versus advanced medical kit

90
Adventure Kits

91
Adventure Kits

92
Other First Aid Kits

99
Godspeed

Similar presentations



































 Dehydration Snow Blindness.>")

