Download presentation
Presentation is loading. Please wait.

1
Breast Cancer Treatment, Outcomes and Recent Advances
Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School

2
National Statistics 1 in 8 women in the U.S. (12 - 13%) will develop invasive breast cancer over the course of her lifetime. In 2010, an estimated 207,000 new cases of invasive breast cancer were diagnosed in women in the U.S., along with 54,000 new cases of non-invasive (in situ) breast cancer; and an estimated 40,000 cancer related deaths were reported. About 1,970 new cases of invasive breast cancer were diagnosed in men in Less than 1% of all new breast cancer cases occur in men Among women aged years, breast cancer remains the leading cause of cancer death despite a steady decrease in breast cancer mortality since 1990.
 breast cancer; and an estimated 40,000 cancer related deaths were reported. About 1,970 new cases of invasive breast cancer were diagnosed in men in Less than 1% of all new breast cancer cases occur in men. Among women aged years, breast cancer remains the leading cause of cancer death despite a steady decrease in breast cancer mortality since")
3
Essex County Cancer Coalition
* Essex County Cancer Coalition

4
COMPARATIVE INCIDENCE & MORTALITY RATES,
NJ and US, FEMALES, (NAACCR-age-adjusted rates per 100,000 (2000 US population standard)) Cancer Site NJ 2006- 2010 US 2006- BREAST All Races White Black API Hispanic Incidence 129.3 133.6 117.1 86. 91.8 122.2 123.5 118 84.7 91.1 Mortality 25.2 25.1 30.9 11.7 13.2 22.6 22.1 30.8 11.5 14.8
) Cancer Site. NJ US BREAST. All Races. White. Black. API. Hispanic. Incidence Mortality")
5
Distribution of Stage at Diagnosis of Breast Cancer, Females, 2006-2010
ALL RACES WHITE BLACK API HISPANIC* BREAST Total Cases 44,430 37,017 4,895 2,097 3,374 Percent 100% In Situ 23.4% 23.5% 20.3% 27.9% 23.6% Local 46.5% 47.7% 40.8% 41.3% 43.0% Regional 22.6% 21.8% 28.8% 24.0% 26.4% Distant 4.7% 4.5% 6.6% 4.1% Unstaged 2.7% 2.5% 3.6% 2.8% 2.6% API, Asian Pacific Islander; *Hispanic includes all races Cancer Incidence and Mortality in New Jersey, , NJ DOH

6
Trends in Female Breast Cancer Incidence and Death Rates by Race and Ethnicity, United States.
Rates are age-adjusted to the 2000 US Standard Population. Data are from the SEER Cancer Statistics Review, , National Cancer Institute, Bethesda, MD.4 From Huo and Dignam in Kuerer’s Breast Surgical Oncology, 2010.

8
Does Cancer Health Disparity = Health Care Disparity?
Income and education influence health insurance coverage and access to appropriate early detection, treatment and palliative care Socioeconomic factors influence exposure to cancer risk factors: tobacco use, poor nutrition, physical activity, and obesity Cultural factors influence health behavior, attitudes toward disease, and choice of treatment

9
Socioeconomic Factors and Access to Medical Care: Are they the only Factors?
Socioeconomic factors account for stage differences at diagnosis for most cancers but not breast and prostate cancer (Cancer 2002, 94: ; Cancer Causes and Control 2003, 14: ) Traditional socioeconomic, clinical, and pathologic factors do not account for the race-related stage difference at diagnosis for prostate cancer (JNCI 2001, 93: ) Breast cancer survival differs by race (AA versus EA) in an equal-access health care facility (Cancer 1998, 82: ; Cancer 2003, 98: ) Accounting for traditional risk factors explains differences in breast cancer incidence and outcome for all race/ethnic groups except African Americans (JNCI 2005, 97: ) Being insured and having access to medical care does not eliminate the survival disparity for African American women with breast cancer (JNCI Monogr 2005, 35: )
 Traditional socioeconomic, clinical, and pathologic factors do not account for the race-related stage difference at diagnosis for prostate cancer (JNCI 2001, 93: ) Breast cancer survival differs by race (AA versus EA) in an equal-access health care facility (Cancer 1998, 82: ; Cancer 2003, 98: ) Accounting for traditional risk factors explains differences in breast cancer incidence and outcome for all race/ethnic groups except African Americans (JNCI 2005, 97: ) Being insured and having access to medical care does not eliminate the survival disparity for African American women with breast cancer (JNCI Monogr 2005, 35: )")
10
What about biology?? “While data suggest that access to quality care is a factor in cancer disparities, other factors also play a major role, including tumor biology and genetics” (JNCI 2009, 101: 984 – 92)
")
11
Biology and Cancer Health Disparity
Race/ethnic disparity in prevalence of basal-like breast tumors (JAMA 2006, 295: 2492 – 2502) Most common among young women of African descent Caveat: Breast cancer survival disparity in US is irrespective of tumor ER status (JNCI 2009, 101: 993 – 1000) High proportion of breast cancer patients in West Africa present with high grade and triple negative disease (J Clin Oncol 2009, 27: 4514 – 21) Race/ethnic differences in prevalence of 8q24 cancer susceptibility markers (Nat Genet 2007, 39: 638 – 44 & 954 – 6; Genome Res 2007, 17: 1717 – 22) Risk alleles are more common among African-Americans
 Most common among young women of African descent. Caveat: Breast cancer survival disparity in US is irrespective of tumor ER status (JNCI 2009, 101: 993 – 1000) High proportion of breast cancer patients in West Africa present with high grade and triple negative disease. (J Clin Oncol 2009, 27: 4514 – 21) Race/ethnic differences in prevalence of 8q24 cancer susceptibility markers (Nat Genet 2007, 39: 638 – 44 & 954 – 6; Genome Res 2007, 17: 1717 – 22) Risk alleles are more common among African-Americans.")
12
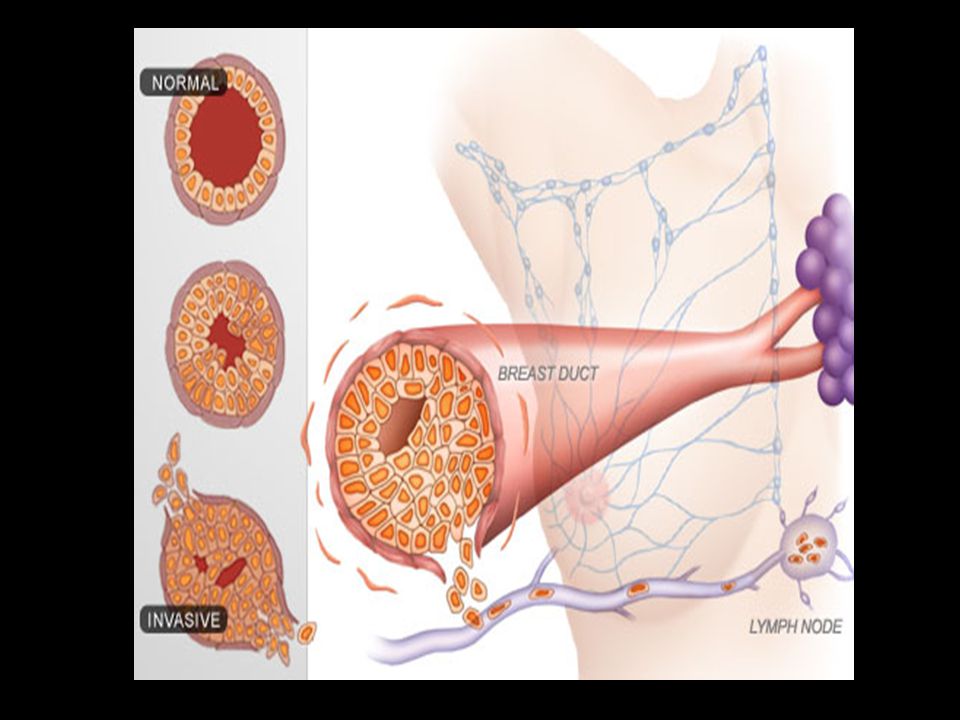
WHAT IS BREAST CANCER?

15
Genomic Subtypes Luminal A: 40%; ER+ and/or PR+; HER2-, slow growing, least aggressive, best prognosis Luminal B: 10-20%; ER+ and/or PR+; HER2+ or high proliferation rate HER2-enriched: 10%; ER/PR- Basal-like: 10-20%; ER/PR/Her2-; worst prognosis Claudin-low: 10%; similar to basal-like

16
HOW DO BREAST CANCER CELLS GROW?

17
Breast Cancer Receptors
ER: estrogen receptor PR: progesterone receptor HER2: human epidermal growth factor receptor-2 E2=estrogen EGF= epidermal growth factor

18
Target specific medications
Trastuzumab (Herceptin) AI=aromatase inhibitors (anastrozole, exemestane) Tamoxifen Lapatinib (Tykerb)
 AI=aromatase inhibitors (anastrozole, exemestane) Tamoxifen. Lapatinib (Tykerb)")
19
Early Breast Cancer Trialists' Collaborative Group (EBCTCG) :
Metaanalysis Tamoxifen Efficacy Figure 5. Effects of about 5 years of tamoxifen on the 15-year probabilities of recurrence and of breast cancer mortality, for ER-positive disease Outcome by allocated treatment in trials of about 5 years of adjuvant tamoxifen The Lancet, Volume 378, Issue 9793, 2011,

20
Adjuvant Endocrine Therapy
Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial The Arimidex, Tamoxifen, Alone or in Combination (ATAC) trial Compare efficacy and safety of anastrozole (1 mg) with tamoxifen (20 mg), as adjuvant treatment for postmenopausal women with early-stage ER+ breast cancer. Anastrazole compared with tamoxifen had improved : disease-free survival time to recurrence time to distant recurrence Fewer contralateral breast cancers as first event compared to tamoxifen daily for 5 years (HR 0.60; 95% CI ; p=0.004) Increased arthralgia and bone fractures Cuzick, et al, The Lancet Oncology, Volume 11, Issue 12, Pages , December 2010
 trial. Compare efficacy and safety of anastrozole (1 mg) with tamoxifen (20 mg), as adjuvant treatment for postmenopausal women with early-stage ER+ breast cancer. Anastrazole compared with tamoxifen had improved : disease-free survival. time to recurrence. time to distant recurrence. Fewer contralateral breast cancers as first event compared to tamoxifen daily for 5 years (HR 0.60; 95% CI ; p=0.004) Increased arthralgia and bone fractures. Cuzick, et al, The Lancet Oncology, Volume 11, Issue 12, Pages , December")
22
Comparison of overall survival by disease stage for women with triple negative breast cancer (TNBC) and those with other phenotypes Adapted from Bauer et al

23
Who gets triple negative breast cancer?
ANY WOMAN CAN GET TRIPLE NEGATIVE BREAST CANCER Highest representation in the following populations: Women of African descent Pre-menopausal women BRCA gene mutation ( BRCA-1) Younger age at menarche, higher parity, younger age at full term pregnancy, shorter duration breast feeding, and higher body mass index (BMI), especially among pre-menopausal women.
 Younger age at menarche, higher parity, younger age at full term pregnancy, shorter duration breast feeding, and higher body mass index (BMI), especially among pre-menopausal women.")
24
Pre-menopausal breast cancer
Unique Challenges Managing Breast Cancer in Young Women

25
Probability of Developing Breast Cancer Within the Next 10 years
By age 20 1 out of 1,681 By age 30 1 out of 232 By age 40 1 out of 69 By age 50 1 out of 42 By age 60 1 out of 29 By age 70 1 out of 27 Lifetime 1 out of 8 American Cancer Society Breast Cancer Facts & Figures,

26
Estimated New Female Breast Cancer Cases and Deaths by Age, US, 2013
Age (yrs) In Situ cases Invasive cases Deaths < 40 1900 10980 1020 <50 15,650 48,910 4,780 50-64 26,770 84,210 11,970 65+ 22,220 99,220 22,870 All ages 64,640 232,340 39,620 Modified from the American Cancer Society, Surveillance and Health Service Research 2013
 In Situ cases. Invasive cases. Deaths. < <50. 15, ,910. 4, , , , , , ,870. All ages. 64, , ,620. Modified from the American Cancer Society, Surveillance and Health Service Research")
27
Different risk factors compared to older women
More likely to be associated with an increased familial risk (BRCA1, BRCA2, TP53, PTEN mutations) Obesity, high caloric intake, high alcohol use, red meat, sedentary lifestyle Recent OCP use, particularly for ER-negative tumors Early childbearing and multiparity
 Obesity, high caloric intake, high alcohol use, red meat, sedentary lifestyle. Recent OCP use, particularly for ER-negative tumors. Early childbearing and multiparity.")
28
Variations according to race and ethnicity
Women >45, breast cancer is more common in whites than blacks Black women under the age of 35 have 2X the incidence of invasive breast cancer and 3X the mortality rate than white women Young black women with Stages II and IV disease had a worse prognosis despite standard therapy (Cancer Causes Control 2003;14: Cancer 2003:97:134-47)
")
29
Survival (%) Age at Diagnosis (Years) Five year relative survival of females diagnosed with breast cancer during , SEER 17
 Age at Diagnosis (Years) Five year relative survival of females diagnosed with breast cancer during , SEER 17.")
30
Clinicopathologic Features
Cancers in women<40: tumors were larger (P=.012) of higher grade (P=.0001) more lymph node positivity (P=.008) lower ER positivity (P=.027) higher rates of HER2/neu over-expression (P=.075) Inferior disease-free survival (HR=1.32,P=.094) J Clin Onc 2008;26:
 of higher grade (P=.0001) more lymph node positivity (P=.008) lower ER positivity (P=.027) higher rates of HER2/neu over-expression (P=.075) Inferior disease-free survival (HR=1.32,P=.094) J Clin Onc 2008;26:")
31
Treatment: variations in outcomes
Women < 50 treated for breast cancer had higher rates of second cancers (bone, ovary, thyroid, kidney) Women <36 y have 13% 10-year cumulative incidence of contralateral breast cancer Women <45 y: Both post lumpectomy and mastectomy radiation conferred an additional 50% incr risk in contralateral breast ca Cancer Epidem Biom Prev 2008;17: J Clin Oncol 2008;26:5561-8
 Women <36 y have 13% 10-year cumulative incidence of contralateral breast cancer. Women <45 y: Both post lumpectomy and mastectomy radiation conferred an additional 50% incr risk in contralateral breast ca. Cancer Epidem Biom Prev 2008;17: J Clin Oncol 2008;26:")
32
Considerations Fertility and pregnancy
Impact of infertility post treatment Bone health Bone density loss after treatment; risk of long term osteopenia, osteoporosis, fractures Psychosocial issues Adequate screening and risk assessment

33
Breast Cancer Treatment
Advances in Surgical Management

34
History of Breast Cancer Surgery
1600 BC: Ancient Egyptians treated breast tumors with cauterization via “fire drill” 17/18th century: Jean Louis Petit, French surgeon linked the concept that cancer spread via lymphatics. First to remove lymph nodes, breast, pectoral muscles 1882: William Stewart Halstead radical mx 1940s: modified radical mastectomy 1971: NSABP B-04: total mx= radical mx 1976: NSABP B-06: lump+ALND+rads=MRM 1999 (2004): NSABP B32: importance of SLNB 2010: ACOSOG Z0011: Futility of ALND for node postive SLNB, for pts undergoing BCT and systemic therapy
: NSABP B32: importance of SLNB. 2010: ACOSOG Z0011: Futility of ALND for node postive SLNB, for pts undergoing BCT and systemic therapy.")
35
1980 : 60 yr old woman with breast cancer Radical Mastectomy : standard treatment

36
Retreat from Mastectomy
Lumpectomy + XRT

38
Optimizing local control
Minimizing disability Minimizing disfigurement

39
Breast Cancer Treatment
SURGERY BREAST CONSERVATION MASTECTOMY Lumpectomy, partial/segmental Simple/total mastectomy or quadrantectomy Modified radical mastectomy Contraindicated in RECONSTRUCTION hx of prior radiation Immediate v delayed Size > 4cm; tumor:breast ratio pregnant women who would require radiation while pregnant

40
Changing Patterns in Surgery
removal of NAC is perceived as mutilating “…NAC seems to be the signature of the breast identity more than the volume or the shape….” J.Y. Petit 2009 Increasing mastectomy and CPM rates Freedom from imaging surveillance Imaging Fatigue or “No Mas” Syndrome Availability of better reconstructive techniques Nipple-sparing mastectomies seemingly oncologically safe

41
Contralateral Prophylactic Mastectomy Rates for Invasive and DCIS
Tuttle, T. M. et al. J Clin Oncol; 27: ALL Mastectomy Patients with CPM (DCIS-SEER) Tuttle, T. M. et al. J Clin Oncol; 25: ALL Mastectomy Patients with CPM (Invasive -SEER)
 Tuttle, T. M. et al. J Clin Oncol; 25: ALL Mastectomy Patients with CPM (Invasive -SEER)")
42
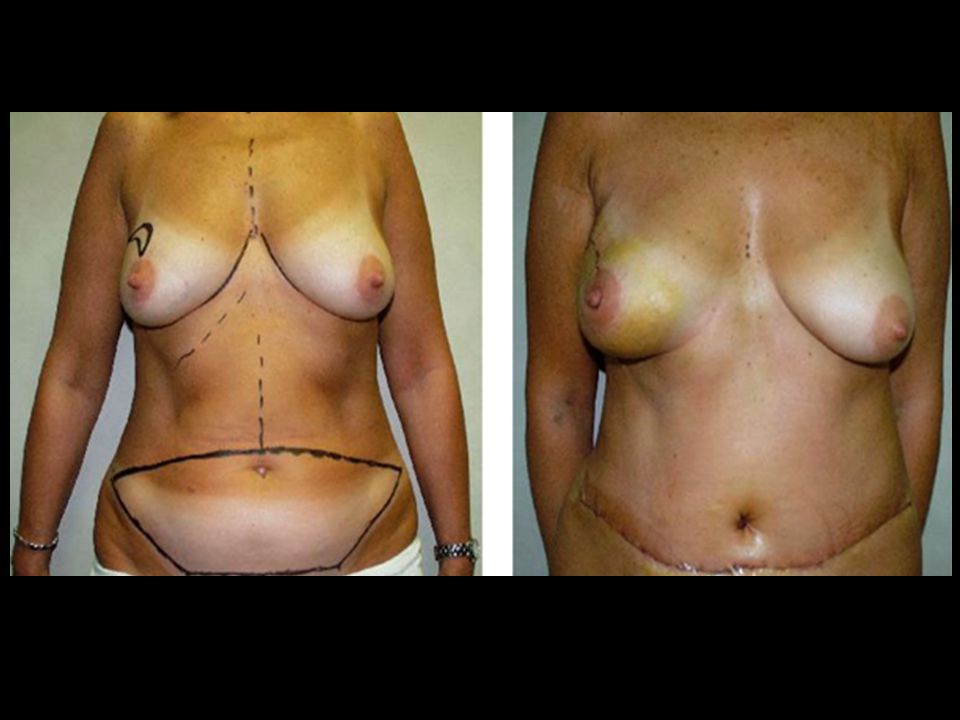
Mastectomy and Breast Reconstruction
Tissue expander placement, followed by permanent implant

43
Skin sparing mastectomy

47
Final thoughts Is breast cancer one disease or actually multiple disease types each requiring a unique treatment Should different screening and treatment algorithms be considered in younger women Will/should future treatment plans be stratified by race

Similar presentations






 Göker E 1, Görümlü G 1, Batıgün O 2 1 University.>")


















