Download presentation
Presentation is loading. Please wait.

1
Cervical Cancer DR KHALID H. WALI SAIT (FRCSC)
1920 colposcopy 1930 was used in Europe USA ACCSP SHORT FOCAL LENGTH CAN NOT DO BIOPSY LONG FOCAL LENGTH NOT COMFORTABLE PERFORM BIOPSY 5 % UNSATSF COLPOSCOPY DR KHALID H. WALI SAIT (FRCSC) ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY King Abdulaziz University Hospital, Jeddah, Saudi Arabia
 ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY. King Abdulaziz University Hospital, Jeddah, Saudi Arabia.")
2
Worldwide cervical cancer rates are high, particularly in developing countries.
According to information published by WHO in 2003:1 Cervical cancer is the second most common cancer (after breast cancer) among women worldwide. Approximately 80% of new cases are reported from developing countries. Worldwide prevalence is estimated at 2,274,000 cases, with approximately 510,000 new cases reported each year. Canada, in contrast, had an estimated incidence of 14,845 cases in Without screening programs (i.e., routine Pap smears), cervical cancer is detected too late and leads to death in almost all cases.1 References World Health Organization. State of the art of new vaccines research and development: Initiative for vaccine research. Geneva, Switzerland: World Health Organization; 2003:1–74. Bosch FX, de Sanjose S. Chapter 1: Human papillomavirus and cervical cancer—burden and assessment of causality. J Natl Cancer Inst Monogr. 2003;(31):3-13.
 among women worldwide. Approximately 80% of new cases are reported from developing countries. Worldwide prevalence is estimated at 2,274,000 cases, with approximately 510,000 new cases reported each year. Canada, in contrast, had an estimated incidence of 14,845 cases in Without screening programs (i.e., routine Pap smears), cervical cancer is detected too late and leads to death in almost all cases.1. References. World Health Organization. State of the art of new vaccines research and development: Initiative for vaccine research. Geneva, Switzerland: World Health Organization; 2003:1–74. Bosch FX, de Sanjose S. Chapter 1: Human papillomavirus and cervical cancer—burden and assessment of causality. J Natl Cancer Inst Monogr. 2003;(31):3-13.")
3
Cancer in Women World Wide Breast Colo-rectal Cervix and Uterus Lung Leukemia-Lymphoma Ovary Saudi Breast Thyroid Leukemia–Lymphoma Colo-rectal Ovary Liver Cervix Uterus

4
Female Genital Tract Malignancy
World Wide Uterus Cervix Ovary Vulva Vagina F.Tube Saudi Ovary Cervix Uterus Vulva Vagina F.Tube

5
Pathogenesis HPV are etiological agent for cancer cervix
HPV DNA can be found in 99.7 % of all cervical carcinoma Type 16, 18, 45 and 31 most frequent. Several epidemiological and molecular studies over two decays

6
HPV Nonenveloped double-stranded DNA virus1 >100 types identified2
~30–40 anogenital2,3 ~15–20 oncogenic*,2,3 types, including 16, 18, 31, 33, 35, 39, 45, 51, 52, 584 HPV 16 (54%) and HPV 18 (13%) accounted for the majority of worldwide cervical cancers.5 Nononcogenic** types include: 6, 11, 40, 42, 43, 44, 544 HPV 6 and 11 are most often associated with external genital warts.3 Key Point There are many different types of HPV; of the ~15–20 oncogenic types, HPV 16 and HPV 18 account for the majority of cervical cancers. Background Papillomaviruses such as HPV are nonenveloped, double-stranded DNA viruses.1 More than 100 HPV types have been detected,2 with >80 types sequenced and classified.3 Approximately 30–40 types of HPV are anogenital, of which ~15–20 types are oncogenic.2,3 In an international meta-analysis (n = 10,058 invasive cervical cancer cases from 85 studies), HPV Types 16 and 18 are oncogenic and account for about two thirds of all cervical cancers—the next 5 most prevalent types (31, 33, 45, 52, 58) account for an additional 18% of cases.4 Other oncogenic HPV types include 35, 39, 51, and 56.5 HPV Types 6 and 11 are nononcogenic and are associated with external genital warts.3 References 1. Howley PM. Papillomavirinae: The viruses and their replication. In: Fields BN, Knipe DM, Howley PM, eds. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1996:2045–2076. 2. Schiffman M, Castle PE. Human papillomavirus: Epidemiology and public health. Arch Pathol Lab Med. 2003;127:930–934. 3. Wiley DJ, Douglas J, Beutner K, et al. External genital warts: Diagnosis, treatment, and prevention. Clin Infect Dis. 2002;35(suppl 2):S210–S224. 4. Clifford GM, Smith JS, Aguado T, Franceschi S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: A meta-analysis. Br J Cancer. 2003:89;101–105. 5. Muñoz N, Bosch FX, de Sanjosé S, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348: 518–527. *High risk; **low risk 1. Howley PM. In: Fields Virology. Philadelphia, Pa: Lippincott-Raven; 1996:2045– Schiffman M, Castle PE. Arch Pathol Lab Med. 2003;127:930– Wiley DJ, Douglas J, Beutner K, et al. Clin Infect Dis. 2002;35(suppl 2):S210–S Muñoz N, Bosch FX, de Sanjosé S, et al. N Engl J Med. 2003;348:518– Clifford GM, Smith JS, Aguado T, Franceschi S. Br J Cancer. 2003:89;101–105.
 and HPV 18 (13%) accounted for the majority of worldwide cervical cancers.5. Nononcogenic** types include: 6, 11, 40, 42, 43, 44, 544. HPV 6 and 11 are most often associated with external genital warts.3. Key Point. There are many different types of HPV; of the ~15–20 oncogenic types, HPV 16 and HPV 18 account for the majority of cervical cancers. Background. Papillomaviruses such as HPV are nonenveloped, double-stranded DNA viruses.1 More than 100 HPV types have been detected,2 with >80 types sequenced and classified.3 Approximately 30–40 types of HPV are anogenital, of which ~15–20 types are oncogenic.2,3 In an international meta-analysis (n = 10,058 invasive cervical cancer cases from 85 studies), HPV Types 16 and 18 are oncogenic and account for about two thirds of all cervical cancers—the next 5 most prevalent types (31, 33, 45, 52, 58) account for an additional 18% of cases.4 Other oncogenic HPV types include 35, 39, 51, and 56.5 HPV Types 6 and 11 are nononcogenic and are associated with external genital warts.3. References. 1. Howley PM. Papillomavirinae: The viruses and their replication. In: Fields BN, Knipe DM, Howley PM, eds. Fields Virology. 3rd ed. Philadelphia, Pa: Lippincott-Raven; 1996:2045– Schiffman M, Castle PE. Human papillomavirus: Epidemiology and public health. Arch Pathol Lab Med. 2003;127:930– Wiley DJ, Douglas J, Beutner K, et al. External genital warts: Diagnosis, treatment, and prevention. Clin Infect Dis. 2002;35(suppl 2):S210–S Clifford GM, Smith JS, Aguado T, Franceschi S. Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: A meta-analysis. Br J Cancer. 2003:89;101– Muñoz N, Bosch FX, de Sanjosé S, et al. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med. 2003;348: 518–527. *High risk; **low risk. 1. Howley PM. In: Fields Virology. Philadelphia, Pa: Lippincott-Raven; 1996:2045– Schiffman M, Castle PE. Arch Pathol Lab Med. 2003;127:930– Wiley DJ, Douglas J, Beutner K, et al. Clin Infect Dis. 2002;35(suppl 2):S210–S Muñoz N, Bosch FX, de Sanjosé S, et al. N Engl J Med. 2003;348:518– Clifford GM, Smith JS, Aguado T, Franceschi S. Br J Cancer. 2003:89;101–105.")
7
Infectious Virus Particle of HPV1,2
1/Baker/p. 1449/Figure 3; p. 1453/col 2/¶ 2 2/Chen/p. 563/col 2/¶ 2 Capsid proteins: L1 L2 Key Point HPV is a nonenveloped, double-stranded DNA virus; its shell is composed of L1 (major) and L2 (minor) proteins. Background HPV is a nonenveloped, double-stranded DNA virus encapsulated with an icosahedral shell.1,2 The virion is made up of 2 late capsid proteins — major (L1) and minor (L2).1,3 The virus shell consists of 72 pentamers, with each pentamer consisting of 5 molecules of L1 that stud the surface of the particle, and 1 molecule of L2 that sits in the conical hollow in the center of the rosette that faces inward.2,4 Virus neutralizing antibodies made in response to natural infections recognize conformational epitopes of L1 on the outer surface of the intact virus particle.5 References 1. Shah KV. Papovaviruses. In: Rose NR, de Macario EC, Folds JD, Lane HC, Nakamura RM, eds. Manual of Clinical Laboratory Immunology. 5th ed. Washington, DC: ASM Press; 1997:655–660. 2. Baker TS, Newcomb WW, Olson NH, Cowsert LM, Olson C, Brown JC. Structures of bovine and human papillomaviruses: Analysis by cryoelectron microscopy and three-dimensional image reconstruction. Biophys J. 1991;60:1445–1456. 3. Kirnbauer R, Booy F, Cheng N, Lowy DR, Schiller JT. Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc Natl Acad Sci USA. 1992;89:12180–12184. 4. Chen XS, Garcea RL, Goldberg I, Casini G, Harrison SC. Structure of small virus-like particles assembled from the L1 protein of human papillomavirus 16. Mol Cell. 2000;5:557–567. 5. Stanley M. Immune responses to human papillomavirus. Vaccine. 2006;24(Suppl 1):S16–S22. 1/Shah/p. 655/col 1/¶ 3 Viral DNA 2/Baker/p. 1448/col 1/¶ 2 3/Kirnbauer/p /col 1/¶ 3/p /col 2/¶ 1 Viral exterior Viral interior 4/Chen/p. 563/col 2/¶ 2/p. 557/col 1/¶2 1. Baker TS, et al. Biophys J. 1991;60:1445–1456. 2. Chen XS, et al. Mol Cell. 2000;5:557–567. 5/Stanley/p. 5/col 1/¶ 1
 and L2 (minor) proteins. Background. HPV is a nonenveloped, double-stranded DNA virus encapsulated with an icosahedral shell.1,2 The virion is made up of 2 late capsid proteins — major (L1) and minor (L2).1,3. The virus shell consists of 72 pentamers, with each pentamer consisting of 5 molecules of L1 that stud the surface of the particle, and 1 molecule of L2 that sits in the conical hollow in the center of the rosette that faces inward.2,4. Virus neutralizing antibodies made in response to natural infections recognize conformational epitopes of L1 on the outer surface of the intact virus particle.5. References. 1. Shah KV. Papovaviruses. In: Rose NR, de Macario EC, Folds JD, Lane HC, Nakamura RM, eds. Manual of Clinical Laboratory Immunology. 5th ed. Washington, DC: ASM Press; 1997:655– Baker TS, Newcomb WW, Olson NH, Cowsert LM, Olson C, Brown JC. Structures of bovine and human papillomaviruses: Analysis by cryoelectron microscopy and three-dimensional image reconstruction. Biophys J. 1991;60:1445– Kirnbauer R, Booy F, Cheng N, Lowy DR, Schiller JT. Papillomavirus L1 major capsid protein self-assembles into virus-like particles that are highly immunogenic. Proc Natl Acad Sci USA. 1992;89:12180– Chen XS, Garcea RL, Goldberg I, Casini G, Harrison SC. Structure of small virus-like particles assembled from the L1 protein of human papillomavirus 16. Mol Cell. 2000;5:557– Stanley M. Immune responses to human papillomavirus. Vaccine. 2006;24(Suppl 1):S16–S22. 1/Shah/p. 655/col 1/¶ 3. Viral DNA. 2/Baker/p. 1448/col 1/¶ 2. 3/Kirnbauer/p /col 1/¶ 3/p /col 2/¶ 1. Viral exterior. Viral interior. 4/Chen/p. 563/col 2/¶ 2/p. 557/col 1/¶2. 1. Baker TS, et al. Biophys J. 1991;60:1445– Chen XS, et al. Mol Cell. 2000;5:557–567. 5/Stanley/p. 5/col 1/¶ 1.")
8
Pathogenesis P53

9
Spectrum of Changes in Cervical Squamous Epithelium Caused by HPV Infection1
Normal Cervix HPV Infection / CIN* 1 CIN 2 / CIN 3 / Cervical Cancer Key Point Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is linked to the activity of E6 and E7 proteins.2 Background HPV infects its host by penetrating through mucosal tears in the basal membrane.3 In benign HPV-associated skin lesions, the HPV virus maintains its genome as episomes at low copy numbers (10–200 copies/cell) in the basal cells of the epithelium separate from the host cell DNA. To maintain its viral DNA as an episome, viral E1 and E2 proteins are expressed. Failure to express E1 leads to the integration of the HPV genome into the host cell chromosome.3 Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is considered an important step in tumor progression.2 In malignant HPV-associated skin lesions, HPV DNA integration into the host cell’s chromosome regularly occurs through a break in the viral genome around the E1/E2 region. Integration-mediated disruption of E2 may trigger uncontrolled expression of E6 and E7, resulting in cellular transformation.2 The E6 protein associates with the tumor suppressor protein p53 and promotes proteolytic destruction of the protein. This leads to malignant transformation and loss of regulated cell growth. The E7 protein associates with the retinoblastoma protein (pRB), which inactivates the cell cycle restriction function of this protein.2 References 1. Gallo G, Bibbo M, Bagella L, et al. Study of viral integration of HPV-16 in young patients with LSIL. J Clin Pathol. 2003;56:532–536. 2. Syrjänen KJ, Syrjänen SM. Molecular biology of papillomaviruses. In: Papillomavirus Infections in Human Pathology. Chichester, United Kingdom: John Wiley & Sons, Inc.; 2000:11–51. 3. Doorbar J. The papillomavirus life cycle. J Clin Virol. 2005;32(suppl):S7–S15. *CIN = cervical intraepithelial neoplasia 1. Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564. Copyright © 2003 Massachusetts Medical Society. All rights reserved. Adapted with permission.
 in the basal cells of the epithelium separate from the host cell DNA. To maintain its viral DNA as an episome, viral E1 and E2 proteins are expressed. Failure to express E1 leads to the integration of the HPV genome into the host cell chromosome.3. Integration of HPV into the DNA of the infected host cell is commonly associated with high-risk oncogenic HPV types1 and is considered an important step in tumor progression.2 In malignant HPV-associated skin lesions, HPV DNA integration into the host cell’s chromosome regularly occurs through a break in the viral genome around the E1/E2 region. Integration-mediated disruption of E2 may trigger uncontrolled expression of E6 and E7, resulting in cellular transformation.2. The E6 protein associates with the tumor suppressor protein p53 and promotes proteolytic destruction of the protein. This leads to malignant transformation and loss of regulated cell growth. The E7 protein associates with the retinoblastoma protein (pRB), which inactivates the cell cycle restriction function of this protein.2. References. 1. Gallo G, Bibbo M, Bagella L, et al. Study of viral integration of HPV-16 in young patients with LSIL. J Clin Pathol. 2003;56:532– Syrjänen KJ, Syrjänen SM. Molecular biology of papillomaviruses. In: Papillomavirus Infections in Human Pathology. Chichester, United Kingdom: John Wiley & Sons, Inc.; 2000:11– Doorbar J. The papillomavirus life cycle. J Clin Virol. 2005;32(suppl):S7–S15. *CIN = cervical intraepithelial neoplasia. 1. Adapted from Goodman A, Wilbur DC. N Engl J Med. 2003;349:1555–1564. Copyright © 2003 Massachusetts Medical Society. All rights reserved. Adapted with permission.")
10
Invasive Cervical Cancer
Natural History of HPV Infection and Potential Progression to Cervical Cancer1 0–1 Year 0–5 Years 1–20 Years Initial HPV Infection Continuing Infection CIN 2/3 Invasive Cervical Cancer CIN 1 Key Point Infection with HPV will typically clear, but some infections with high-risk HPV types may ultimately lead to cervical cancer via a number of intermediate steps. Background Following initial HPV infection, the course of progression to cervical cancer depends on the type of HPV. Low-risk HPV types (such as HPV 6 or 11) have a negligible risk of progressing but may persist.1 Overall, the majority of HPV infections spontaneously clear within the first 24 months.2 High-risk types (such as types HPV 16 and 18) are often associated with CIN 2 or higher lesions. The strong association of HPV 16 with CIN 2 or greater suggests that lesions caused by this infection evolve to CIN 2 without a prolonged period as CIN 1.1 Approximately 57% of low-grade lesions (CIN 1) will regress, 32% will persist, and 11% will progress. The risk of developing invasive cancer is estimated to be 1% in patients with CIN 1. Approximately 43% of CIN 2 lesions will regress, 35% will persist, 22% will progress to CIN 3, and 5% will progress to invasive cancer. The likelihood of CIN 3 regressing is about 32%, persistence is <56%, and rate of progression to invasive cancer is >12%.3 In studies of women with HPV infection who developed CIN 2 or 3, the initial abnormal smear was interpreted as CIN 2 or 3 in two thirds of cases,1,4 indicating that most CIN 3 lesions do not evolve from CIN 1.1 In a large, prospective study, mean times of progression from mild, moderate, or severe dysplasia to development of carcinoma in situ (CIS) were 58, 38, and 12 months, respectively.5 In general, CIN occurs at least a decade earlier than invasive cancer, supporting a concept of the temporal evolution of cervical cancer.3 Based on a Markov model that approximated age-specific incidence of cervical cancer and HPV infection-associated events, the peak prevalence of low-grade squamous intraepithelial lesions (LSIL) is at 28 years of age, at 42 years of age for HSIL, and at 48 years of age for cervical cancer.6 References 1. Pinto AP, Crum CP. Natural history of cervical neoplasia: Defining progression and its consequence. Clin Obstet Gynecol. 2000;43:352–362. 2. Ho GYF, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423–428. 3. Ostor AG. Natural history of cervical intraepithelial neoplasia: A critical review. Int J Gynecol Pathol. 1993;12:186–192. 4. Koutsky LA, Holmes KK, Critchlow CW, Stevens CE, Paavonen J, et al. A cohort study of the risk of cervical intraepithelial neoplasia grade 2 or 3 in relation to papillomavirus infection. N Engl J Med. 1992;327:1272–1278. 5. Richart RM, Barron BA. A follow-up study of patients with cervical dysplasia. Am J Obstet Gynecol. 1969;105:386–393. 6. Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection and cervical carcinogenesis. Am J Epidemiol. 2000;151:1158–1171. Cleared HPV Infection 1. Pinto AP, Crum CP. Clin Obstet Gynecol. 2000;43:352–362.
 have a negligible risk of progressing but may persist.1 Overall, the majority of HPV infections spontaneously clear within the first 24 months.2 High-risk types (such as types HPV 16 and 18) are often associated with CIN 2 or higher lesions. The strong association of HPV 16 with CIN 2 or greater suggests that lesions caused by this infection evolve to CIN 2 without a prolonged period as CIN 1.1 Approximately 57% of low-grade lesions (CIN 1) will regress, 32% will persist, and 11% will progress. The risk of developing invasive cancer is estimated to be 1% in patients with CIN 1. Approximately 43% of CIN 2 lesions will regress, 35% will persist, 22% will progress to CIN 3, and 5% will progress to invasive cancer. The likelihood of CIN 3 regressing is about 32%, persistence is <56%, and rate of progression to invasive cancer is >12%.3 In studies of women with HPV infection who developed CIN 2 or 3, the initial abnormal smear was interpreted as CIN 2 or 3 in two thirds of cases,1,4 indicating that most CIN 3 lesions do not evolve from CIN 1.1 In a large, prospective study, mean times of progression from mild, moderate, or severe dysplasia to development of carcinoma in situ (CIS) were 58, 38, and 12 months, respectively.5. In general, CIN occurs at least a decade earlier than invasive cancer, supporting a concept of the temporal evolution of cervical cancer.3 Based on a Markov model that approximated age-specific incidence of cervical cancer and HPV infection-associated events, the peak prevalence of low-grade squamous intraepithelial lesions (LSIL) is at 28 years of age, at 42 years of age for HSIL, and at 48 years of age for cervical cancer.6. References. 1. Pinto AP, Crum CP. Natural history of cervical neoplasia: Defining progression and its consequence. Clin Obstet Gynecol. 2000;43:352– Ho GYF, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423– Ostor AG. Natural history of cervical intraepithelial neoplasia: A critical review. Int J Gynecol Pathol. 1993;12:186– Koutsky LA, Holmes KK, Critchlow CW, Stevens CE, Paavonen J, et al. A cohort study of the risk of cervical intraepithelial neoplasia grade 2 or 3 in relation to papillomavirus infection. N Engl J Med. 1992;327:1272– Richart RM, Barron BA. A follow-up study of patients with cervical dysplasia. Am J Obstet Gynecol. 1969;105:386– Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection and cervical carcinogenesis. Am J Epidemiol. 2000;151:1158–1171. Cleared HPV Infection. 1. Pinto AP, Crum CP. Clin Obstet Gynecol. 2000;43:352–362.")
11
HPV Clearance In women years of age ~80% of HPV infections are transient Gradual development of cell-mediated immune response presumed mechanism In a study of 608 college women, 443 infected, 70% of new infections cleared within 1 year and 91% within 2 years Mean duration of infection - 8 months HPV 16 and 18 infections persist longer Key Point Several studies have confirmed that HPV 16 is more likely to persist than other HPV types.1 Background Several studies have evaluated the duration of HPV infection. In the study by Ho and colleagues, 608 college women in the United States were followed (mean age, 20 years) for an average of 2.2 years.2 The investigators reported median durations of infections of 11 months (95% CI, 7–12 months) and 12 months (95% CI, 6–17 months) with HPV types and 18, respectively. In contrast, the median duration of HPV 6 infection was 6 months (95% CI, 6–7 months).2 In a study of 1610 Colombian women 15–85 years of age (median age, 32 years), the median duration of high-risk HPV infection was 15 months (95% CI, 13–17 months), whereas the median duration of low-risk HPV infection was 11 months (95% CI, 8–17 months). Duration of infection with HPV types 16 and 18 were 14 months (95% CI, 8–19 months) and 12 months (95% CI, 9–17 months), respectively.3 Among university students 17–42 years of age (mean, 23 years) in Canada, Richardson and colleagues reported a slightly longer median time to loss of HPV infection in individuals infected with high-risk HPV types (17 months; 95% CI, 15–19 months) compared with individuals infected with low-risk HPV types (15 months; 95% CI, 11–18 months). Duration of infection for HPV types 16, 18, and 6 were 19 months (95% CI, 11–28 months), 9 months (95% CI, 5–14 months), and 6 months (95% CI, 5–8 months), respectively.4 In a study of the duration of HPV infection in 1075 women 15–19 years of age (median, 18 years) in the United Kingdom, Woodman and colleagues reported median durations of detectability of 10 months (95% CI, 7–17) for HPV 16, 8 months (95% CI, 6–13) for HPV 18, and 9 months (95% CI, 6–13) for HPV type 6 or 11.5 References 1. Molano M, van den Brule A, Plummer M, et al. Determinants of clearance of human papillomavirus infections in Colombian women with normal cytology: A population-based, 5-year follow-up study. Am J Epidemiol. 2003;158:486–494. 2. Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423–428. 3. Muñoz N, Méndez F, Posso H, et al. Incidence, duration, and determinants of cervical human papillomavirus infection in a cohort of Colombian women with normal cytological results. J Infect Dis. 2004;190:2077–2087. 4. Richardson H, Kelsall G, Tellier P, et al. The natural history of type-specific human papillomavirus infections in female university students. Cancer Epidemiol Biomarkers Prev. 2003;12:485–490. 5. Woodman CB, Collins S, Winter H, et al. Natural history of cervical human papillomavirus infection in young women: A longitudinal cohort study. Lancet. 2001;357:1831–1836.
 for an average of 2.2 years.2 The investigators reported median durations of infections of 11 months (95% CI, 7–12 months) and 12 months (95% CI, 6–17 months) with HPV types 16 and 18, respectively. In contrast, the median duration of HPV 6 infection was 6 months (95% CI, 6–7 months).2. In a study of 1610 Colombian women 15–85 years of age (median age, 32 years), the median duration of high-risk HPV infection was 15 months (95% CI, 13–17 months), whereas the median duration of low-risk HPV infection was 11 months (95% CI, 8–17 months). Duration of infection with HPV types 16 and 18 were 14 months (95% CI, 8–19 months) and 12 months (95% CI, 9–17 months), respectively.3. Among university students 17–42 years of age (mean, 23 years) in Canada, Richardson and colleagues reported a slightly longer median time to loss of HPV infection in individuals infected with high-risk HPV types (17 months; 95% CI, 15–19 months) compared with individuals infected with low-risk HPV types (15 months; 95% CI, 11–18 months). Duration of infection for HPV types 16, 18, and 6 were 19 months (95% CI, 11–28 months), 9 months (95% CI, 5–14 months), and 6 months (95% CI, 5–8 months), respectively.4. In a study of the duration of HPV infection in 1075 women 15–19 years of age (median, 18 years) in the United Kingdom, Woodman and colleagues reported median durations of detectability of 10 months (95% CI, 7–17) for HPV 16, 8 months (95% CI, 6–13) for HPV 18, and 9 months (95% CI, 6–13) for HPV type 6 or References. 1. Molano M, van den Brule A, Plummer M, et al. Determinants of clearance of human papillomavirus infections in Colombian women with normal cytology: A population-based, 5-year follow-up study. Am J Epidemiol. 2003;158:486– Ho GY, Bierman R, Beardsley L, Chang CJ, Burk RD. Natural history of cervicovaginal papillomavirus infection in young women. N Engl J Med. 1998;338:423– Muñoz N, Méndez F, Posso H, et al. Incidence, duration, and determinants of cervical human papillomavirus infection in a cohort of Colombian women with normal cytological results. J Infect Dis. 2004;190:2077– Richardson H, Kelsall G, Tellier P, et al. The natural history of type-specific human papillomavirus infections in female university students. Cancer Epidemiol Biomarkers Prev. 2003;12:485– Woodman CB, Collins S, Winter H, et al. Natural history of cervical human papillomavirus infection in young women: A longitudinal cohort study. Lancet. 2001;357:1831–1836.")
12
Cervical Cancer Prevention
Education About early symptom of cancer cervix Avoid Risk Factors Screening and Vaccine

13
Risk Co Factor: HIV HPV 16,18 SMOKING MULTIPPLE SEXUAL PARTNER ? BCP

14
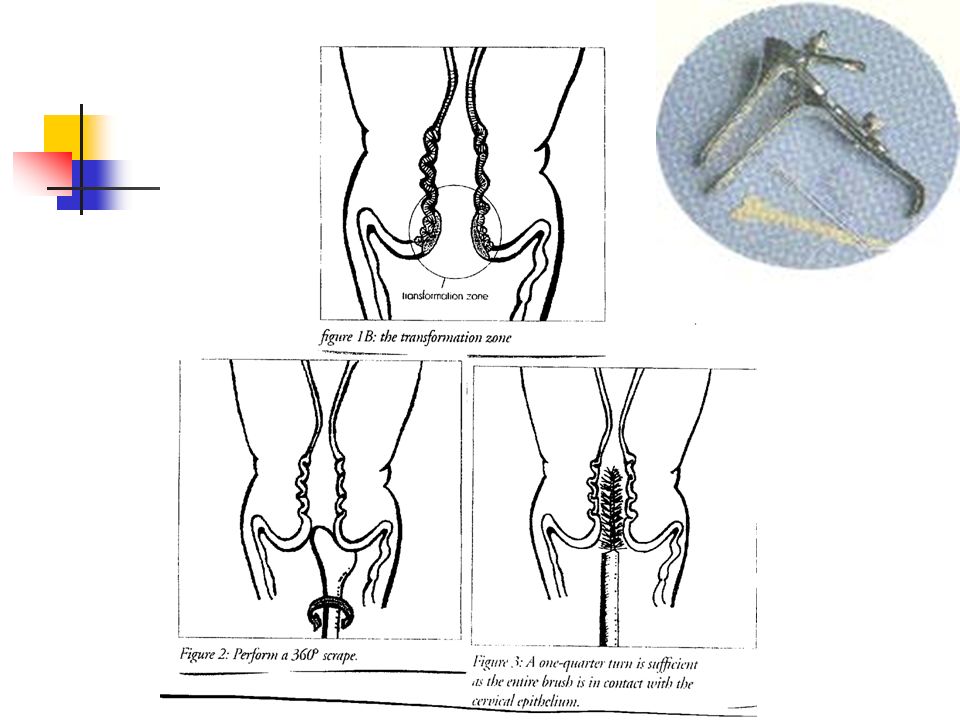
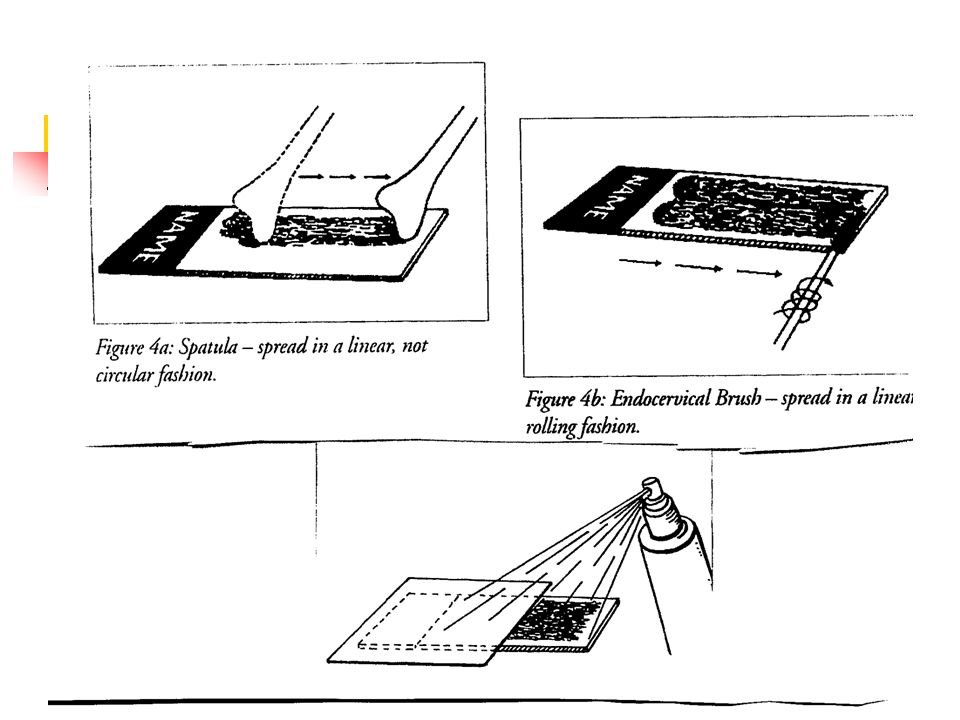
Cancer Cervix Has an easily identified pre-invasive disease and be diagnosed and treated before become an invasive disease Screening Test

18
THIN PREP Liquid based cytology

19
Q7

20
Recommendations of ACS(2004)
The present guideline reflect the current understanding of underlying epidemiology of CIN and the introduction of new technology in screening

21
False negative ( 30%) GOOD SCREENING ?
 GOOD SCREENING")
22
Ideal (not essential) Patient’s Conditions For Screening
No vagina douching for 48 hours Avoided use of contraceptive creams or jellies for 48 hours No intercourse for 24 hours Not recommended during menstruation, mid cycle smear is optimum Patient should be required to provide her LMP

24
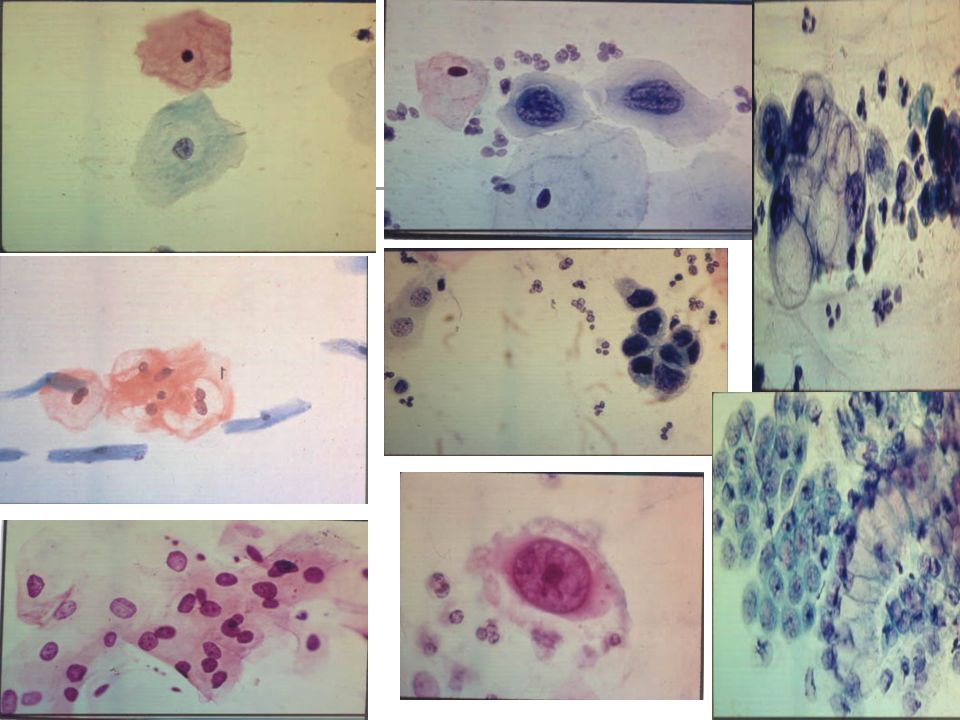
Changes in Terminology
L SIL HPV CIN I Mild Dysplasia H SIL CIN II Moderate Dysplasia CIN III Severe Dysplasia Carcinoma insitu

25
Management Of Pap Smear Result
Pap smear is simply a lab test it is the responsibility of the physician to interpret the result in the context of a given patient and her particular circumstances

26
1920 colposcopy 1930 was used in Europe USA ACCSP SHORT FOCAL LENGTH CAN NOT DO BIOPSY LONG FOCAL LENGTH NOT COMFORTABLE PERFORM BIOPSY 5 % UNSATSF COLPOSCOPY

27
Objective Of Colposcopy
Exclude invasive disease Select the most appropriate area for biopsy

28
Detailed Colposcopic Exam.
Original squamocolumnar junction Present squamocolumnar junction Transformation zone Endocervical canal IS COLPOSCOPY SATISFACTORY ?

30
a grape-like or "sea-anemone"

32
RCT

34
Cancer of the Cervix Clinical presentation
Abnormal vaginal bleeding Postmenopausal Vaginal bleeding Vaginal discharge Pain Asymptomatic

35
Invasive Disease

36
Cancer of the Cervix Histological types
Squamous cell ca Adenocarcinoma Other

37
Cancer of the Cervix Mode of spread
Direct Lymphatic Hematogenous

38
Cancer of the Cervix Investigations
EUA Complete blood count Liver function test Renal function tests CXR/IVP or CT Cystoscopy Sigmoidoscopy

39
Cancer of the Cervix FIGO Staging ( clinical )
I - Tumour confined to the cervix II- Upper 2/3 vagina / parametrium. III- Lower 1/3 vagina / pelvic side wall or hydronephrosis IV- Adjacent organ / Distant metastasis

40
Cancer of Cervix Prognostic Factors

41
Cancer of the Cervix Treatment of patients
Radical Hysterectomy and lymphadnectomy Radiation Therapy and chemotherapy

43
Pelvic Radiation EBR and Brachytherapy
Chemotherapy

44
What is: Radiotherapy

45
How Radiotherapy works ?

46
Follow up

47
RECURRENT CERVICAL CANCER
Treatment depends on: Site of recurrence Mode of primary therapy

48
Pelvic Exenteration:

49
Cancer of the Cervix stage/survival

50
Prophylactic Vaccine Virus – neutralization antibodies to prevent infection Generate antibodies in genital tract epithelium directed against the L1 and L2 capsid proteins

51
Commercial HPV Vaccines
GSK vaccine (Harper 2004) 16/18(100% efficacy) Merck vaccine (villa 2005) 6/11/16/18 ( 88% efficacy (RCT PLACEBO) 0,1,6 months 16-23 y old
 16/18(100% efficacy) Merck vaccine (villa 2005) 6/11/16/18 ( 88% efficacy (RCT PLACEBO) 0,1,6 months y old.")
52
Gardasil: Quadrivalent HPV Vaccine
0.5 ml IM, day 0, month 2, and month 6 COST ~$130 each vaccine dose Storage: 2-8oC, should not be frozen, protect from light. *NEED TO PRESERVE THE “COLD CHAIN”* Contraindications: hypersensitivity to the active substances or components Precautions: May not be effective Not for use in active warts, cervical cancer, CIN VIN, VAIN Does not provide protection against none vaccine HPV types Not recommended for use in pregnancy, Category B

53
Who? Women 9-26 Do not need to have pap smear before vaccination
Testing for HPV is not recommended prior to vaccination Sexually active women can be vaccinated, may be less effective in women who have been previously exposed to HPV

54
Cervical Cancer DR KHALID H. WALI SAIT (FRCSC)
1920 colposcopy 1930 was used in Europe USA ACCSP SHORT FOCAL LENGTH CAN NOT DO BIOPSY LONG FOCAL LENGTH NOT COMFORTABLE PERFORM BIOPSY 5 % UNSATSF COLPOSCOPY DR KHALID H. WALI SAIT (FRCSC) ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY King Abdulaziz University Hospital, Jeddah, Saudi Arabia
 ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY. King Abdulaziz University Hospital, Jeddah, Saudi Arabia.")
Similar presentations







: The Background, Current Status and Future of Vaccines to Prevent HPV Infection, Abnormal Genital Lesions and Cervical Cancer.>")











 Consultant Obstetrician & Gynaecologist Infertility Specialist.>")
 ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY King Abdulaziz University Hospital, Jeddah, Saudi Arabia.>")



