Download presentation
Presentation is loading. Please wait.

1
CCF in Neonates Dr Rajesh Kumar
MD (PGI), DM (Neonatology) PGI, Chandigarh, India Rani Children Hospital, Ranchi
, DM (Neonatology) PGI, Chandigarh, India. Rani Children Hospital, Ranchi.")
2
Aim What are the causes of CCF in neonate?
How to diagnose CCF in a neonate? What are the different investigations required? What is the treatment?

3
Definition Heart is unable to meet the metabolic demands of the tissues

4
Pul edema, hepatomegaly
Stress on heart HR Contractility catecholamine autonomic input Preload renal preservation venous constriction Decompesation HR Pul edema, hepatomegaly ¯ Cardiac output

5
Diagnosis of CCF Clinical Radiographic findings Laboratory findings

6
Signs and symptoms of CCF
Tachycardia Venous congestion Right side Hepatomegaly Ascitis Pleural effusion Edema Left side Tachypnea Retactions Crepitations Pul. edema Low cardiac output Acute Pallor Sweating Cool extremities capillary refill Altered sensorium Chronic Feeding difficulty Fatigue Poor growth

7
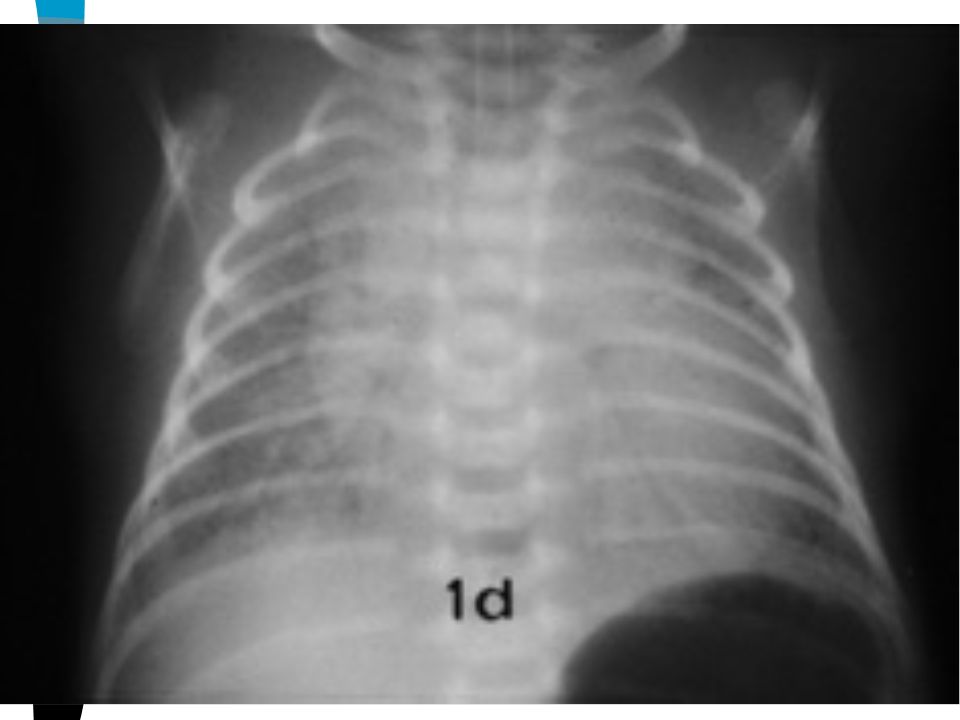
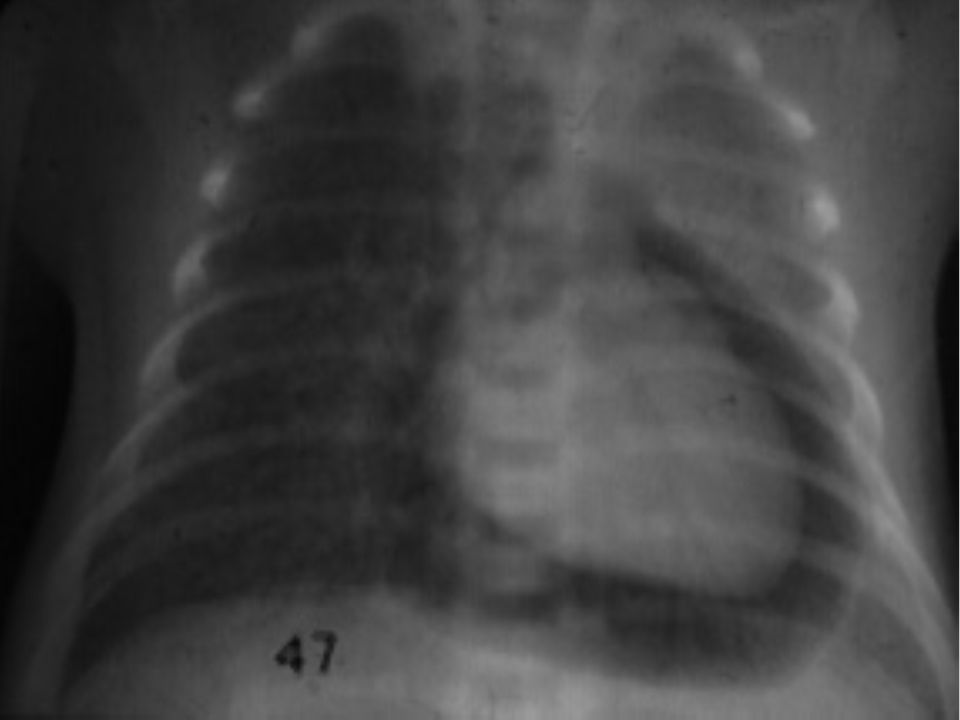
Diagnosis of CCF: X-ray
To rule out primary pulmonary disease Magnitude of pulmonary blood flow Cardiac size Cardiac shape: (boot shaped, egg on side, snow man)
")
9
Diagnosis of CCF: ECG More useful in D/D of cyanotic newborn with ¯ pul blood flow -90 Tricuspid atresia 180 Pul atresia with intact vent septum TOF, Pul stenosis +90

10
Diagnosis of CCF: Echo Rules out associated significant heart disease in pt with pulmonary disease Doppler echo is preffered Operator dependant Examination of extracardiac structure is limited

11
Diagnosis of CCF: Cardiac catheterisation
Necessary to delineate vascular anatomy before surgery in some cases

12
Causes of CCF Cardiac Non-cardiac Preload (ARF) Afterload (HT)
Structural Arrythmia Myocardial dysfunction Extracardiac compression Non-cardiac Preload (ARF) Afterload (HT) ¯ O2 carrying capacity (anemia) Demand (sepsis)
 Afterload (HT) ¯ O2 carrying capacity (anemia) Demand (sepsis)")
14
Case study Term newborn well for first 2-3 hours, developed respiratory distress, gradually worsening CPAP for 3 days, gradually improved but continues to have problem, Day 1 echo ?? coarct Day 5 echo showed significant coarct Dischraged on day 7, worsened in next 4-5 days Operated for coarct at day 25 of life, now (5 months) doing well
 doing well.")
15
Case study 33 weeks, infant of diabetic mother
Had respiratory distress since birth, suspected to have HMD, had murmur Echo showed PDA with Co-actation of aorta Medical management tried, Surgery done in third week, Now asymptomatic

17
Causes of CCF: Cardiac-structural heart disease
Left ventricular outflow tract obstruction Aortic stenosis, co-arctation of aorta Ductus dependant lesions Critical aortic stenosis, preductal coarctation of aorta, interrupted aortic arch, hypoplastic left heart syndrome, TGA Left to right shunt VSD, PDA, ASD Regugitant lesions ECD, truncus arterioisus 00

18
Case study Term newborn, Wt 3.0 Kg
Antenataly suspected congenital heart block At birth heart rate 50 per minute, Echo: normal, ECG: s/o CHB Developed tachypnea and retraction on day 3 Required temporary pacing followed by permament pace maker implant Well till 1 year of life

20
Causes of CCF: Cardiac-arrythmia
Congenital heart block Supraventricular tachycardia Ventricular tachycardia

21
Causes of CCF: Cardiac-myocardial dysfunction
Cardiomyopathy Perinatal asphyxia Myocardial infarction Sepsis Acute LVF

22
Treatment Treatment of underlying cause
Reversing metabolic derangements Improving cardiac performance Altering preload / afterload burden Improved oxygen delivery Enhanced nutrition

23
Improving cardiac performance
Sympathomimetics Dopamine Dobutamine Phenylephrine Adrenaline, Noradrenaline Phosphodiasterase inhibitors Amrinone, Minrinone Digoxin

24
Dopamine Naturally acting catecholamine
Low dose direct stimulation of dopamine receptors, higher dose works through release of norepinephrine Premature babies require lesser dose than term babies Dose (mg/kg/min) Effects 1-5 HR, UOP, contractility 5-10 HR, contractility, BP HR, contractility, BP, SVR
 Effects. 1-5 HR, UOP, contractility HR, contractility, BP HR, contractility, BP, SVR.")
25
Dopamine 40 mg per ml (1mg per unit by insuline syringe) Neonate:
In Pediadrip set: 2mg /kg/ 6hrs fluid (5.5 mg/kg/min) to 6mg/kg/6hours fluid By infusion pump: 15 mg (15 units) dopamine + 50 ml NS, 1ml/kg/hour ( 5mg/kg/min) to 4 ml/kg/hour
 to 6mg/kg/6hours fluid. By infusion pump: 15 mg (15 units) dopamine + 50 ml NS, 1ml/kg/hour ( 5mg/kg/min) to 4 ml/kg/hour.")
26
Dobutamine 50 mg per ml (1.25mg per unit by insuline syringe) Neonate:
In Pediadrip set: 2mg /kg/ 6hrs fluid (6.87 mg/kg/min) to 6mg/kg/6hours fluid By infusion pump: 15 mg (15 units) dopamine + 50 ml NS, 1ml/kg/hour ( 6.87 mg/kg/min) to 4 ml/kg/hour
 to 6mg/kg/6hours fluid. By infusion pump: 15 mg (15 units) dopamine + 50 ml NS, 1ml/kg/hour ( 6.87 mg/kg/min) to 4 ml/kg/hour.")
27
Dobutamine Synthetic catecholamine Does not depend on NE stores
Effects: contractility, ¯SVR, HR Often used with dopamine to contractility and to avoid extreme vasoconstriction associated with high dose dopamine

28
Amrinone Positive inotropy + Vasodilator
Can be combined with sympathomimetics Precautions: not in hypovolumic, not in pt with fixed systemic outflow tract obstruction Dose: Neonate: loading: mg/kg, folowwed by infusion of 3-5 mg/kg/min Infant: loading: mg/kg, folowwed by infusion of 10 mg/kg/min

29
Amrinone 5 mg per ml, 20 ml ampoule, dilute only with saline, never with dextrose Neonate: 10mg (2ml) + NS 48 ml 1ml/kg/hr (3.3 mg/kg/min) to 1.5ml/kg/hr Infant: 30mg (6ml) + NS 44 ml 1ml/kg/hr (10 mg/kg/min)
 to 1.5ml/kg/hr. Infant: 30mg (6ml) + NS 44 ml. 1ml/kg/hr (10 mg/kg/min)")
30
Epinephrine myocardial contractility, SVR
Useful in sepsis induced cardiac failure as second or third line drug Dose: Starting mg/kg/min can be rapidly Preparation: 0.3ml(12 units)+ 50 ml NS, Start with ML in kg /hr (0.1 mg/kg/min ) and then increase
+ 50 ml NS, Start with ML in kg /hr (0.1 mg/kg/min ) and then increase.")
31
Digoxin Inotropic agent Loading dose:
Premature neonate:20-30 mg/kg Term neonate: mg/kg Schedule for loading: ½, ¼, ¼ 8hours apart Maintanance dose: Premature neonate: 5-10 mg/kg/day BD Term neonate: 10 mg/kg/day BD

32
Digoxin Route: IV, IM, oral Injection: 1ml ampoule, 250 mg /ml
1unit = 6.25 mg ; 10 mg /kg = 1.5units/kg Oral (Digoxin Paed elixir): 1ml = 0.05 mg Maintenance dose: 0.01 mg/kg/day Wt in kg /10 ml twice daily 3 kg: 0.3 ml twice daily
: 1ml = 0.05 mg. Maintenance dose: 0.01 mg/kg/day. Wt in kg /10 ml twice daily. 3 kg: 0.3 ml twice daily.")
33
Alteration of preload Fluid retention due to low cardiac output and ¯ renal perfusion Ventricular contractility is compromised due to massive volume overload Diuretics: Acute diuresis: Furosemide 1-4 mg/kg/dose Chronic diuresis: Furosemide + potassium sparing diuretics

34
Alteration of afterload
Precaution: Do not use in hypovolumic condition and in pt with fixed left ventricular outflow obstruction Effective in Regurgitant lesions(ECD, Cardiomyopathy) and left to right shunts (VSD) Acute: Nitroprusside, Dobutamine, amrinone Chronic: ACE inhibitors Enalapril: 0.1 mg/kg /day OD or BD ( 5 kg: ¼ tab OD)
 and left to right shunts (VSD) Acute: Nitroprusside, Dobutamine, amrinone. Chronic: ACE inhibitors. Enalapril: 0.1 mg/kg /day OD or BD ( 5 kg: ¼ tab OD)")
35
Prostaglandin E1 Useful in ductal dependant CHD
Best before 96 hours after birth Dose: 0.5 –0.2 mg/kg/minute Presentation: ALPOSTIN, 1 ml ampoule, 1ml=500mg C/I: PFC, infradiafragmatic TAPVC Side effects: Apnea

36
Correction of metabolic derangements
Correct metabolic acidosis 2 ml/kg bolus, later by ABG report Correct hypoglycemia 2 ml/kg of 10% dextrose Correct hypocalcemia 2 ml/kg calicium gluconate over 5 minutes

37
Improved oxygen delivery
Oxygen content of blood= Hb X %saturation X X PaO2 Start oxygen Blood transfusion if HB <10-13 gm% Iron supplementation

38
PDA in premature babies
Prophylactic indomethacin or ibuprofen in <1500 gms and < 34 weeks Fluid restriction Diuretics: lasix Therapeutic: Indomethacin: 0.2 mg/kg per dose 8 hourly three doses Ibuprofen: 5-10 mg/kg per dose 8 hourly three doses

39
Summary Treat metaboloic derangements aggresively
Get echo done whenever in doubt Many of the structural heart disease is treatable is our setup

40
Thank You

41
Thank you

Similar presentations













 with Suspected Heart Disease (A Pragmatist’s Guide) Nick Pigott Staff Specialist in Paediatric Intensive Care Children’s Hospital.>")







