Download presentation
Presentation is loading. Please wait.

1
Marketing PET in Radiation Treatment Planning
Welcome! Marketing PET in Radiation Treatment Planning PET Marketing Forum – Accelerating Practice Growth May 23, 2007 Dr. Homer Macapinlac

2
Brought To You By Cardinal Health
Part of PET FoundationsSM > comprehensive marketing and education program Continuation of 2006 series > advanced topics Recorded presentation and PowerPoint available on > News > Marketing Forum Exclusive benefit to Cardinal Health PET customers Continuing this Fall

3
Dr. Homer Macapinlac Over 15 years of PET experience
Read over 15,000 clinical PET scans MD Anderson Cancer Center MDA Volume > X PET/CTs per month

4
Promises, Promises Know your target FDG PET is approved for staging
NSCLC Head and Neck Ca FDG PET is approved for staging No CPT code for FDG PET in RT planning

5
From Jemal, A. et al. CA Cancer J Clin 2006;56:106-130.
Copyright ©2006 American Cancer Society

6
Lung Cancer Staging Treatment based on stage
Survival correlates with stage Stage Year Survival I % II % IIIa % IIIb, IV <5%

7
FDG PET Improves Staging
PET potentially avoided unnecessary thoracotomy in 1 out of 5 patients Reed J et.al. Thorac Cardiovasc Surg. 2003;126(6): Van Tinteren et.al. Lancet 2002; 359: 1388–92 Nodal Stage:Sensitivity/Specificity 85/91% High NPV M1 detection – mean 13% Stage I -7.5%, Stage II - 18%, Stage III – 24% McManus, et.al. I J R O B P 2001;50:287293
: Van Tinteren et.al. Lancet 2002; 359: 1388–92. Nodal Stage:Sensitivity/Specificity 85/91% High NPV. M1 detection – mean 13% Stage I -7.5%, Stage II - 18%, Stage III – 24% McManus, et.al. I J R O B P 2001;50:")
9
PET/CT Better Than PET Prospective, Blinded, 120 pts
PET-CT was more accurate for N2 nodes (96% VS 93%) and N1 nodes (90% VS 80%, p=0.001) PET-CT more sensitive, specific, and >PPV for both N2 and N1 nodes (p < 0.05 for all). PET-CT is significantly more sensitive at the 4R, 5, 7, 10 L and 11 stations and more accurate at the 7 and 11 stations than dedicated PET. BACKGROUND: The treatment of patients with nonsmall cell lung cancer (NSCLC) is determined by the stage. We evaluated the accuracy of staging using integrated positron emission tomography (PET) and computed tomography (CT) and compared it with dedicated PET visually correlated with CT scan. METHODS: A prospective blinded trial was performed on a consecutive series of patients with NSCLC. Patients underwent integrated PET-CT scanning with 2-[18F]-fluoro-2-deoxy-D-glucose (FDG-18). A radiologist assigned the T, N and M status. No sooner than 2 weeks the same radiologist read the dedicated PET alone, without the integrated CT images and a T, N and M status was assigned again. The most recent CT scan was available and visually correlated with both studies. All patients underwent biopsies of suspicious N2 or N3 lymph node or distant metastases and if negative, pulmonary resection with lymphadenectomy was performed. RESULTS: There were 129 patients. Integrated PET-CT is a better predictor than PET for all stages of cancer and achieved statistical significance for stage I (52% versus 33%, p = 0.03) and for stage II (70% versus 36%, p = 0.04). It also is a better overall predictor for T status (70% versus 47%, p = 0.001) and the N status (78% versus 56%, p = 0.008). Nodal analysis shows that integrated PET-CT was more accurate for the total N2 nodes (96% versus 93%, p = 0.01) and for the total N1 nodes (90% versus 80%, p = 0.001). It was also more sensitive, specific, and had a higher positive predictive value for both N2 and N1 nodes (p < 0.05 for all). Integrated PET-CT is significantly more sensitive at the 4R, 5, 7, 10 L and 11 stations and more accurate at the 7 and 11 lymph nodes stations than dedicated PET. CONCLUSIONS: Integrated PET-CT using FDG-18 better predicts stage I and II disease as well as the T and N status of patients with NSCLC when compared with dedicated PET alone. It is more accurate at some nodal stations but still only achieves an accuracy of 96% and 90% for the N2 and N1 nodes, respectively. Cerfolio et.al. Ann Thorac Surg Sep;78(3): ;
 and N1 nodes (90% VS 80%, p=0.001) PET-CT more sensitive, specific, and >PPV for both N2 and N1 nodes (p < 0.05 for all). PET-CT is significantly more sensitive at the 4R, 5, 7, 10 L and 11 stations and more accurate at the 7 and 11 stations than dedicated PET. BACKGROUND: The treatment of patients with nonsmall cell lung cancer (NSCLC) is determined by the stage. We evaluated the accuracy of staging using integrated positron emission tomography (PET) and computed tomography (CT) and compared it with dedicated PET visually correlated with CT scan. METHODS: A prospective blinded trial was performed on a consecutive series of patients with NSCLC. Patients underwent integrated PET-CT scanning with 2-[18F]-fluoro-2-deoxy-D-glucose (FDG-18). A radiologist assigned the T, N and M status. No sooner than 2 weeks the same radiologist read the dedicated PET alone, without the integrated CT images and a T, N and M status was assigned again. The most recent CT scan was available and visually correlated with both studies. All patients underwent biopsies of suspicious N2 or N3 lymph node or distant metastases and if negative, pulmonary resection with lymphadenectomy was performed. RESULTS: There were 129 patients. Integrated PET-CT is a better predictor than PET for all stages of cancer and achieved statistical significance for stage I (52% versus 33%, p = 0.03) and for stage II (70% versus 36%, p = 0.04). It also is a better overall predictor for T status (70% versus 47%, p = 0.001) and the N status (78% versus 56%, p = 0.008). Nodal analysis shows that integrated PET-CT was more accurate for the total N2 nodes (96% versus 93%, p = 0.01) and for the total N1 nodes (90% versus 80%, p = 0.001). It was also more sensitive, specific, and had a higher positive predictive value for both N2 and N1 nodes (p < 0.05 for all). Integrated PET-CT is significantly more sensitive at the 4R, 5, 7, 10 L and 11 stations and more accurate at the 7 and 11 lymph nodes stations than dedicated PET. CONCLUSIONS: Integrated PET-CT using FDG-18 better predicts stage I and II disease as well as the T and N status of patients with NSCLC when compared with dedicated PET alone. It is more accurate at some nodal stations but still only achieves an accuracy of 96% and 90% for the N2 and N1 nodes, respectively. Cerfolio et.al. Ann Thorac Surg Sep;78(3): ;")
10
RT Plan PTV GTV CTV Planned target volume Gross tumor volume CTV
Clinical target volume CTV GTV CTV

11
Delineation of GTV & Normal Organs in the Thorax
How to reduce NTCP? 3DCRT/IMRT/Proton Right Lung Left Lung Heart Esophagus Spinal Cord Target Volume (TV) Delineation of GTV & Normal Organs in the Thorax
 Delineation of GTV & Normal Organs in the Thorax.")
12
Effect of FDG-PET on Radiation Treatment Volumes in NSCLC
Study Year Patients w/ change in RTP Hiffer (1998) 7/15 (46%) Nestle (1999) 12/34 (35%) Munley (1999) 12/35 (34%) Vanuystel (2000) 45/73 (62%) Giraud (2001) 5/12 (42%) McManus (2001) 38/102 (37%) Erdi (2002) 7/11 (64%) Ciernik (2003) 18/39 (56%)* Brianzoni (2005) 11/25 (44%)*PET/CT
 7/15 (46%) Nestle (1999) 12/34 (35%) Munley (1999) 12/35 (34%) Vanuystel (2000) 45/73 (62%) Giraud (2001) 5/12 (42%) McManus (2001) 38/102 (37%) Erdi (2002) 7/11 (64%) Ciernik (2003) 18/39 (56%)* Brianzoni (2005) 11/25 (44%)*PET/CT.")
15
559020

17
Differences Between PET and CT
CT – 0.5 sec rotation PET scan takes 3 to 6 mins per bed of 15 cm. CT scan of 90 cm is normally less than 30 sec. PET spatial resolution is about 6 mm. CT spatial resolution can be less than 0.5 mm. PET temporal resolution is around a breathing cycle. CT temporal resolution is normally less than 1 sec. In CT attenuation correction of PET data, the difference in temporal resolution is not accounted for, and it is the major source of misalignment between CT and PET. Scan of 15 cm for 3 to 6 mins, Spatial resolution ~ 6 mm Temporal resolution ~ breathing cycle Scan of 90 cm < 30 sec Spatial resolution < 0.5 mm Temporal resolution < 1 sec Potential Misalignment Between PET and CT Images

18
Misalignment In Breathing States
Helical CT Scout X-ray on End-inspiration (FB) Mid-expiration (BH) Here is a breathing trace of a patient during the CT scan. The X-ray on is shown for both scout and helical CT. The patient was free-breathing until a breathing instruction was given. Breath-in, breath-out and hold your breath at mid-expiration. We can appreciate the difference between the breath-hold state and the free-breathing state. This is one source of misalignment between CT and PET. End-expiration (FB) (sec)
 Mid-expiration. (BH) Here is a breathing trace of a patient during the CT scan. The X-ray on is shown for both scout and helical CT. The patient was free-breathing until a breathing instruction was given. Breath-in, breath-out and hold your breath at mid-expiration. We can appreciate the difference between the breath-hold state and the free-breathing state. This is one source of misalignment between CT and PET. End-expiration (FB) (sec)")
19
4D-CT: Pan et.al. Med Phys. 2004 Feb;31(2):333-40.
Respiratory tracking with Varian RPM optical monitor CT images acquired over complete respiratory cycles Signal from RPM system First couch position Second couch position Third couch We propose a new scanning protocol for generating 4D-CT image data sets influenced by respiratory motion. A cine scanning protocol is used during data acquisition, and two registration methods are used to sort images into temporal phases. A volume is imaged in multiple acquisitions of 1 or 2 cm length along the cranial-caudal direction. In each acquisition, the scans are continuously acquired for a time interval greater than or equal to the average respiratory cycle plus the duration of the data for an image reconstruction. The x ray is turned off during CT table translation and the acquisition is repeated until the prescribed volume is completely scanned. The scanning for 20 cm coverage takes about 1 min with an eight-slice CT or 2 mins with a four-slice CT. After data acquisition, the CT data are registered into respiratory phases based on either an internal anatomical match or an external respiratory signal. The internal approach registers the data according to correlation of anatomy in the CT images between two adjacent locations in consecutive respiratory cycles. We have demonstrated the technique with ROIs placed in the region of diaphragm. The external approach registers the image data according to an externally recorded respiratory signal generated by the Real-Time Position Management (RPM) Respiratory Gating System (Varian Medical Systems, Palo Alto, CA). Compared with previously reported prospective or retrospective imaging of the respiratory motion with a single-slice or multi-slice CT, the 4D-CT method proposed here provides (1) a shorter scan time of three to six times faster than the single-slice CT with prospective gating; (2) a shorter scan time of two to four times improvement over a previously reported multi-slice CT implementation, and (3) images over all phases of a breathing cycle. We have applied the scanning and registration methods on phantom, animal and patients, and initial results suggest the applicability of both the scanning and the registration methods. X-ray on Respiratory Motion Tracking With Retrospective Gating
 Respiratory Gating System (Varian Medical Systems, Palo Alto, CA). Compared with previously reported prospective or retrospective imaging of the respiratory motion with a single-slice or multi-slice CT, the 4D-CT method proposed here provides (1) a shorter scan time of three to six times faster than the single-slice CT with prospective gating; (2) a shorter scan time of two to four times improvement over a previously reported multi-slice CT implementation, and (3) images over all phases of a breathing cycle. We have applied the scanning and registration methods on phantom, animal and patients, and initial results suggest the applicability of both the scanning and the registration methods. X-ray on. Respiratory Motion Tracking With Retrospective Gating.")
20
Impact of Respiratory Motion on IMRT
Components 10 Gy 20 Gy 35 Gy 50 Gy 70 Gy Composite Dong, Zhang, et al MDACC

21
3-mm CTV margins for pathologic lymph nodes <20 mm and more generous margins for lymph nodes >or=20 mm Fig. 1. (a) Representative example of extracapsular extension of a 17-mm metastatic lymph node from a patient with T2N2 non–small-cell lung cancer. Hematoxylin and eosin–stained cross section (×10 magnification) shows tumor (T) extension outside the nodal capsule (C). The extent of extracapsular extension is 3.3 mm from the external capsule border to the farthest extent of the tumor (the line). (b) The site where the tumor ruptured the capsule is denoted by R (×40 magnification). Determining optimal clinical target volume margins on the basis of microscopic extracapsular extension of metastatic nodes in patients with non-small-cell lung cancer. Int J Radiat Oncol Biol Phys Mar 1;67(3):
 Representative example of extracapsular extension of a 17-mm metastatic lymph node from a patient with T2N2 non–small-cell lung cancer. Hematoxylin and eosin–stained cross section (×10 magnification) shows tumor (T) extension outside the nodal capsule (C). The extent of extracapsular extension is 3.3 mm from the external capsule border to the farthest extent of the tumor (the line). (b) The site where the tumor ruptured the capsule is denoted by R (×40 magnification). Determining optimal clinical target volume margins on the basis of microscopic extracapsular extension of metastatic nodes in patients with non-small-cell lung cancer. Int J Radiat Oncol Biol Phys Mar 1;67(3):")
22
Head and Neck CA Sixth Most Common Cancer Worldwide
USA: 2% of all cancers, 2% of all deaths Imaging vital for detection, staging and treatment. Early stage curable (T1/2 N0M0) Most w/ nodal mets 45%, M1-10% Second primary – 5% annual rate
 Most w/ nodal mets 45%, M1-10% Second primary – 5% annual rate.")
24
How Could PET/CT Help XRT?
May improve tumor localization Enlarge/reduce/confirm primary tumor target Enlarge/reduce/confirm neck coverage May improve treatment selection Whole body staging Biological characterization, heterogeneity May improve response assessment Need for neck dissection Dose/treatment selection

25
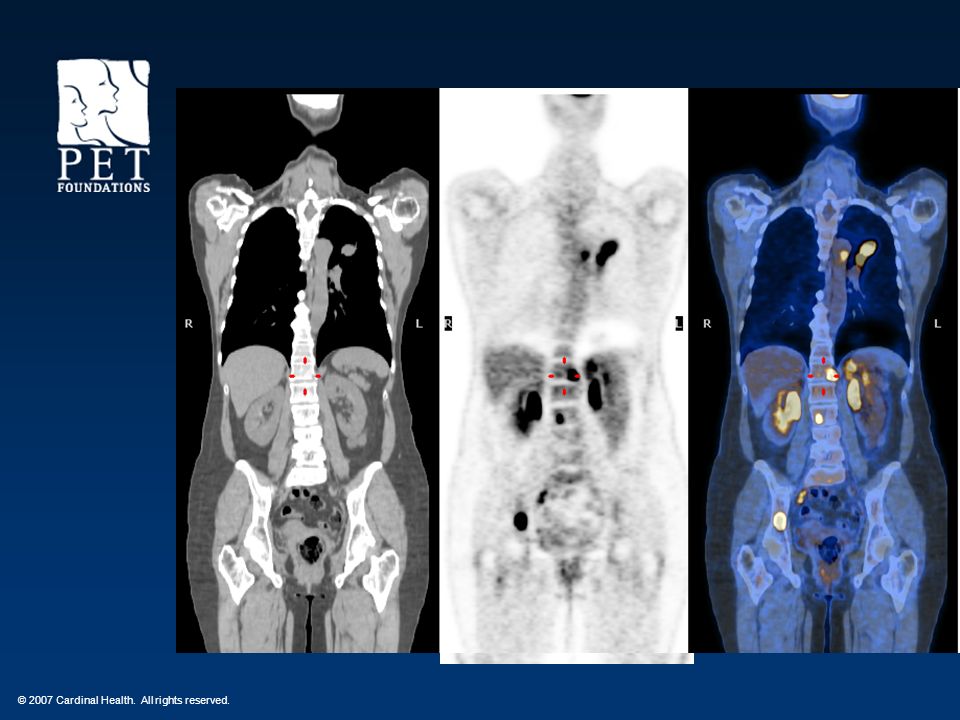
Figure 1 PET/CT images of a 58-year-old male with squamous cell carcinoma of the right tonsil
Frank SJ et al. (2005) Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322
 Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322.")
26
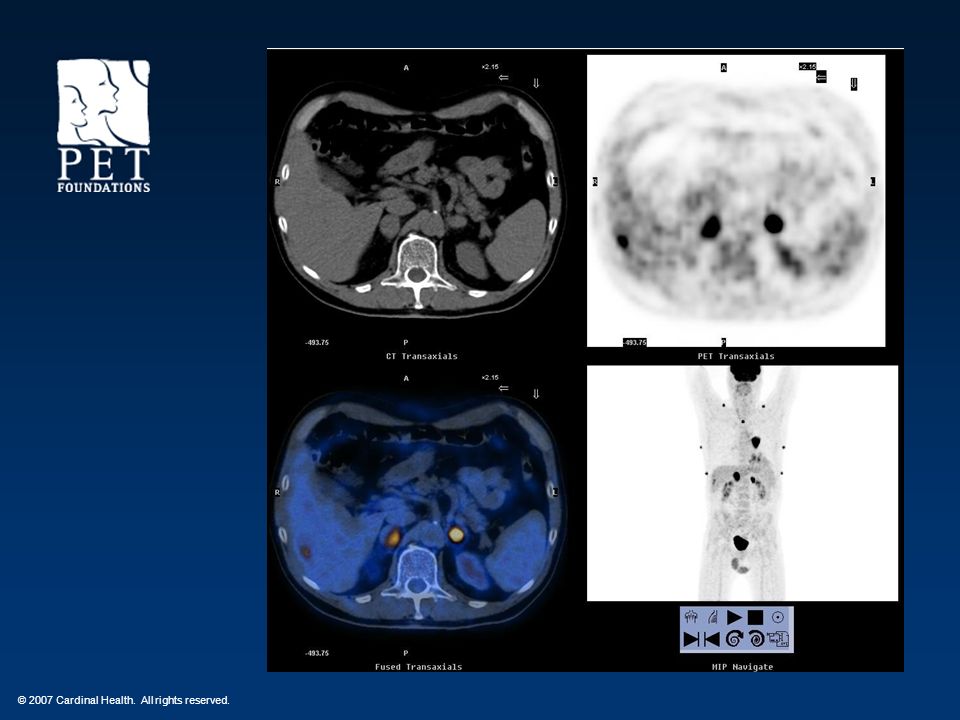
Figure 2 Radiation treatment planning prior to definitive chemoradiation therapy
Frank SJ et al. (2005) Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322
 Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322.")
27
Figure 3 Response to definitive chemoradiation therapy after 3 months
Frank SJ et al. (2005) Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322
 Technology Insight: PET and PET/CT in head and neck tumor staging and radiation therapy planning Nat Clin Pract Oncol 2: 526– /ncponc0322.")
28
PET/CT Challenges—GTV Registration
Nature Clin Oncol :2:10: ;2005

29
PET/CT Challenges—GTV Thresholding
Nature Clin Oncol :2:10: ;2005

30
Nodal CTV Delineation 0.5 – 1 cm CTV margins
Apisarnthanarax et al. Int J Radiat Oncol Biol Phys. 64:678, 2006

31
right-sided oropharyngeal primary

33
Synchronous Primary Cancers References
Head Neck and Esophageal – 12% Radiother Oncol Dec;77(3): Screening for Distant mets or secondary primaries with FDG PET – 6% Oral Oncol Mar;42(3): The detection of distant metastases and second primary tumours at the time of initial evaluation changes the prognosis and influences the selection of treatment modality in patients with HNSCC. Until recently chest CT was the single most effective test to screen for distant metastases in HNSCC patients. In this observational cohort study we prospectively compared the yield of whole body (18)FDG-PET and chest CT to detect distant metastases and synchronous primary tumours. The results of whole body (18)FDG-PET and chest CT were analysed in 34 consecutive HNSCC patients with previously established risk factors for the presence of distant metastases. Four patients were diagnosed with distant metastases or second primary tumours: CT as well as (18)FDG-PET identified one patient with lung metastases and another with primary lung cancer. In addition, (18)FDG-PET detected second primary tumours in two patients (hepatocellular carcinoma and abdominal adenocarcinoma). However increased uptake sites at (18)FDG-PET in lung, liver and pelvis in five patients were not confirmed by other imaging modalities. The added value of whole body (18)FDG-PET versus chest CT was to identify unknown malignancy in 6% of the patients. Confirmation of positive (18)FDG-PET findings is feasible and necessary.
: Screening for Distant mets or secondary primaries with FDG PET – 6% Oral Oncol Mar;42(3): The detection of distant metastases and second primary tumours at the time of initial evaluation changes the prognosis and influences the selection of treatment modality in patients with HNSCC. Until recently chest CT was the single most effective test to screen for distant metastases in HNSCC patients. In this observational cohort study we prospectively compared the yield of whole body (18)FDG-PET and chest CT to detect distant metastases and synchronous primary tumours. The results of whole body (18)FDG-PET and chest CT were analysed in 34 consecutive HNSCC patients with previously established risk factors for the presence of distant metastases. Four patients were diagnosed with distant metastases or second primary tumours: CT as well as (18)FDG-PET identified one patient with lung metastases and another with primary lung cancer. In addition, (18)FDG-PET detected second primary tumours in two patients (hepatocellular carcinoma and abdominal adenocarcinoma). However increased uptake sites at (18)FDG-PET in lung, liver and pelvis in five patients were not confirmed by other imaging modalities. The added value of whole body (18)FDG-PET versus chest CT was to identify unknown malignancy in 6% of the patients. Confirmation of positive (18)FDG-PET findings is feasible and necessary.")
34
New PET Foundations Marketing Tools
Under Construction RTP Module PowerPoints Case Studies Referring Physician Letter New Service Announcement

35
Marketing PET in Radiation Treatment Planning
How Did You Like This Session? Please Fill Out The Polling Questions Before You Leave Thank You! Continuing This Fall!

Similar presentations









 experience.>")










 patients Policy.>")

