Download presentation
Presentation is loading. Please wait.

1
Ventilation of Patients with COPD and Asthma

3
Chronic lung diseases with airflow obstruction
Asthma Chronic Bronchitis Emphysema

4
Chronic lung diseases with airflow obstruction
Asthma Chronic bronchitis Emphysema

5
Asthma Emphysema Bronchitis

6
COPD CXR

7
Near fatal asthma Phenotypes Gradual Onset Sudden Onset

8
Near fatal asthma

9
Mechanical Venitlation of COPD & Asthma Exacerbations
Objectives Pathophysiology - PaCO2 dederminants - Gas trapping - Work of breathing - Auto-PEEP NIPPV - IPAP - EPAP Mechanical ventilation - FIO2 - PEEP - VT

10
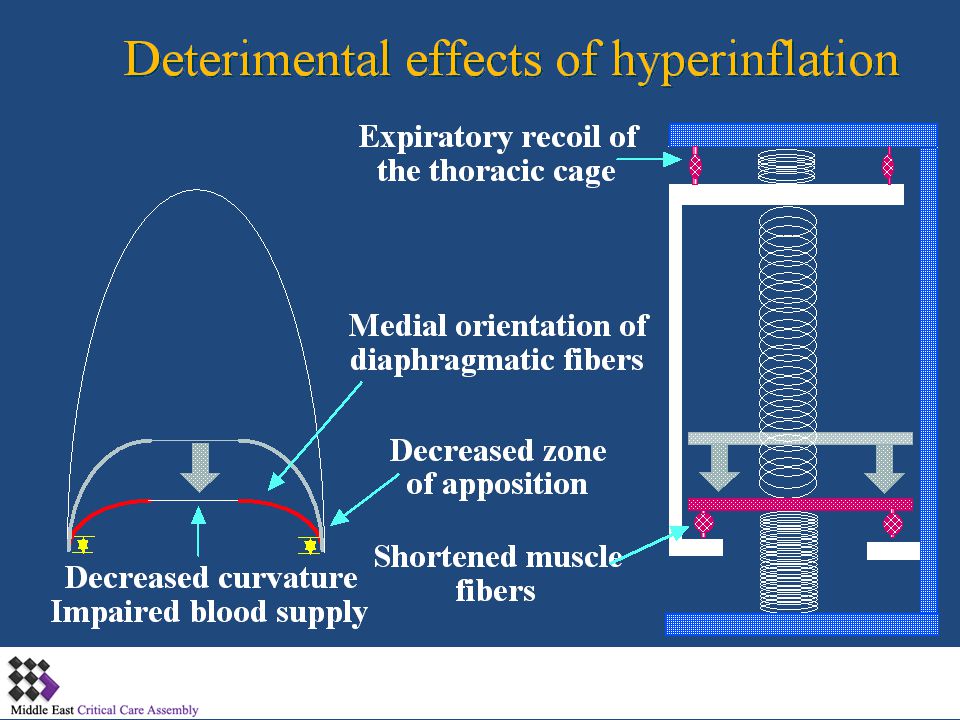
Pathohysiology of Asthma/COPD Exacerbations
Airway narrowing & obstruction Steroids IPAP MV Frictional WOB Airway Inflammation Abx? PEEP Shortened muscles, ¯ curvature Auto- PEEP BDs Elastic WOB Gas trapping MV? ¯ muscle strength VCO2 VT VE IPAP MV? PaCO2 pH PaO2 VA

11
Determinants of PaCO2 PaCO2 VCO2 VA VCO2 VA Work VE
- Agitation - Seizures - WOB Metabolism - Fever - CHO - T4 VA VE - RR - VT - VD (without VE)
")
12
Oxygen Cost of Breathing
Roussos, JCI 1959

13
PV Curve in COPD and Asthma (Stable)
Emphysema 6 Normal/ Asthma VL (L) VT 4 2 VT -10 -20 -30 -40 Ptp (cm H2O) Macklem and Becklake, 1963
 VT VT Ptp (cm H2O) Macklem and Becklake,")
14
PV Curve in COPD & Asthma (Acute Exacerbtion)
Emphysema 6 Asthma VL (L) 4 VT 2 VT -10 -20 -30 -40 Ptp (cm H2O)
 4. VT. 2. VT Ptp (cm H2O)")
15
Implication VT falls because FRC encroaches on TLC
Limited ability to VT with MV/IPAP Best way to PaCO2 is to VCO2 WOB (frictional and/or elastic) PaCO2 even if VT, VE and VA are constant
 PaCO2 even if VT, VE and VA are constant.")
16
Work of Breathing Total Work Elastic Work Frictional Work
RV FRC TLC

17
Effect of VA/Q on PaCO2 (Normal)
PAO2 = 100 PACO2 = 40 PAO2 = 100 PACO2 = 40 DCO2 = 100 ml/min VCO2 = 100 ml/min VCO2 = 100 ml/min DCO2 = 100 ml/min PvCO2 = 46 PvCO2 = 46 PcCO2 = 40 PcCO2 = 40 PaCO2 = 40

18
Effect of VA/Q on PaCO2 (Low VA/Q, Normal)
PAO2 = 50 PACO2 = 40 PAO2 = 100 PACO2 = 40 50% VE 50% VE DCO2 = 50 ml/min VCO2 = 50 ml/min VCO2 = 150 ml/min DCO2 = 150 ml/min PvCO2 = 46 PvCO2 = 46 PcCO2 = 40 PcCO2 = 40 HPV PaCO2 = 40

19
Effect of VA/Q on PaCO2 (Low VA/Q,, AECOPD)
PAO2 = 50 PACO2 = 40 PAO2 = 100 PACO2 = 40 50% VE VE at max DCO2 = 50 ml/min VCO2 = 50 ml/min VCO2 = 100 ml/min DCO2 = 150 ml/min PvCO2 = 46 PvCO2 = 46 PcCO2 = 40 PcCO2 = 44 HPV PaCO2 = 42

20
Effect of VA/Q on PaCO2 (Low VA/Q,, AECOPD, FIO2)
PAO2 = 100 PACO2 = 44 PAO2 = 100 PACO2 = 44 FIO2 50% VE VE constant DCO2 = 100 ml/min VCO2 = 50 ml/min VCO2 = 50 ml/min DCO2 = 100 ml/min PvCO2 = 46 PvCO2 = 46 PcCO2 = 44 PcCO2 = 44 HPV PaCO2 = 44

21
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
22
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
23
Which Patients with COPD benefit from NIV ?

24
NIPPV Pathophysiology of AECOPD & Asthma is amenable to Rx with NIPPV
· EPAP for auto-PEEP · IPAP for inspiratory Raw Will work of breathing · VCO2 · At constant VA, PaCO2 and pH May VA May mortality and intubation rate

25
Which Patients with COPD benefit from NIV ? Hospital Mortality
12% NNT 8 2%

26
NIV in Severe Asthma 17 Episodes of ARF due to asthma
2 patients required intubation for worsening PaC02 Duration of NPPV was 16±21 h. All patients survived. Length of hospital stay was 5±4 days

27
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
29
Peak Airway Pressure & Normal Plateau
Resistance Resistance Compliance Time Time

30
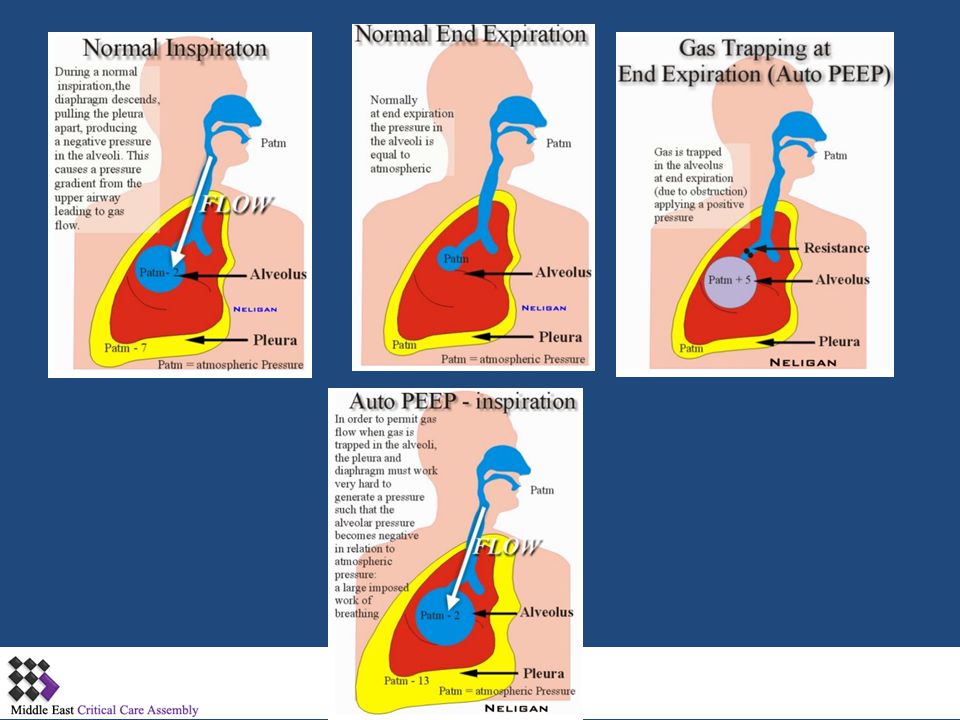
Air-trapping in Asthma/COPD Patients on Mechanical Ventilation
Lung volume Tidal ventilation VEI VT V T I :E 1:1 Hi I : E 1: 6 V EE FRC Time

31
Assessment of Mechanics
Raw= Peak - Plateau Auto-PEEP

32
Obstructive Airway Disease
Beware of auto-PEEP!

34
After the third breath, the airway was occluded at end-expiration using the end-expiratory hold function on the ventilator. During the period of zero flow, pressure in the alveoli and ventilator circuit equilibrate, and the plateau pressure reflects auto or intrinsic positive end-expiratory pressure (PEEPi), indicated by the arrow.
, indicated by the arrow..")
35
Giving CPAP to a patient who has auto-PEEP
The increased work of breathing associated with auto-PEEP can be offloaded by applying CPAP to the trachea/mouth, and splinting open the connecting airways.

36
The use of external PEEP in the setting of auto-PEEP may be conceptualized by the "waterfall over a dam" analogy. In this analogy, the presence of dynamic hyperinflation and 10 cmH20 of auto-PEEP is represented in the top panel by the reservoir of water trickling over the dam represented by the solid block. In the middle panel, as long as the external PEEP is less than or equal to the amount of auto-PEEP, the amount of water in the upstream reservoir, representing dynamic hyperinflation, does not increase. However, once the amount of water in the reservoir does increase (bottom panel), dynamic hyperinflation worsens.
, dynamic hyperinflation worsens..")
39
Excessive Inspiratory Time
Inspiration Normal Patient Increase WOB and “Fighting” of the ventilator Time (sec) Flow (L/min) } Air Trapping Auto-PEEP Expiration
 Flow (L/min) } Air Trapping. Auto-PEEP. Expiration.")
40
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
41
Pressure or Volume Mode?
Predictable TV Peak-Plat gradient Monitor Plat Better acidosis control Pressure Minimise over-distension Monitor Tidal volume Excess volumes as airway resistance improves

42
Mechanical Ventilation of COPD & Asthma Exacerbations
Mode: AC vs IMV PS ? rest respiratory muscles: CMV Better sleep with AC vs. IMV-PS Ventilator-induced diaphragm changes (?) Triggering: key issue with either mode PEEP to counter auto-PEEP Major cause of patient-ventilator dissynchrony
 Triggering: key issue with either mode. PEEP to counter auto-PEEP. Major cause of patient-ventilator. dissynchrony.")
43
Initial Ventilator Settings
Inspiratory time 0.8 – 1.2 secs RR 10-12 TV 6-8 ml/Kg Pplat < 30 cm H2O PEEP ??

44
Assessment of Hyperinflation
CVS effects disconnect Pplat PEEPi measurement

45
Reducing Hyperinflation
I : E 1: 2 Reduce rate Reduce tidal volume Increase expiratory time Increase inspiratory flow rate Increased Peak Airway Pressure Monitor (Pplat) Tolerate increased CO2 (minimise dead space) I : E 1: 6
 Tolerate increased CO2. (minimise dead space) I : E. 1: 6.")
46
COPD flow and frequency
As flow increased from 30 to 60 and 90 L/min (from right to left), frequency increased from (18 to 23 and 26 breaths/min, respectively), Auto-PEEP decreased (from 15.6 to 14.4 and 13.3 cm H2O, respectively) and end-expiratory chest volume also fell. Increases in flow from 30 L/min to 60 and 90 L/min also led to decreases in the swings in Pes from 21.5 to 19.5 and 16.8 cm H2O.
, frequency increased from (18 to 23 and 26 breaths/min, respectively), Auto-PEEP decreased (from 15.6 to 14.4 and 13.3 cm H2O, respectively) and end-expiratory chest volume also fell. Increases in flow from 30 L/min to 60 and 90 L/min also led to decreases in the swings in Pes from 21.5 to 19.5 and 16.8 cm H2O.")
47
Hypercapnia: How permissive?
Defence of intracellular pH Apnoeic oxygenation in dogs to pH 6.5 and PaCO2 of 55kPa Anaesthetic mishap with PaCO2 of > 300 mmHg (40 kPa) and pH of 6.6 survived without sequelae Am J Respir Crit Care Med 1994; 150:
 and pH of 6.6 survived without sequelae. Am J Respir Crit Care Med 1994; 150:")
48
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
49
External & Internal PEEP
Waterfall Concept Pao Pao 10 10 EPP EPP 10 +10 10 Palv Palv 10 10 10 Pel Ppl Ppl

50
Effect of Auto-PEEP Normal airway resistance (end-exhalation)
Ptp = 5 - 5 PA = 0 Patm = 0 Ppl = - 5 Pel = 5 - 5 D Ppl needed to initiate inhalation: - 1 PA drops to - 1 relative to Patm

51
Effect of Auto-PEEP Airway narrowing causing auto-PEEP
Ptp = 8 2 PA = 10 Ppl = 2 Patm = 0 2 Pel = 8 D Ppl needed to initiate inhalation: - 11

52
Treatment of Auto-PEEP with PEEP or CPAP
Airway narrowing with auto-PEEP: Treatment with PEEP Ptp = 8 2 PA = 10 Ppl 2 PEEP = 10 2 Pel = 8 D Ppl needed to initiate inhalation: - 1 The only thing PEEP does is ¯ work of breathing

53
Implication PEEP, EPAP, CPAP No effect on VE, VT or VA
WOB (elastic) - VCO2 (on next breath) - PaCO2 (on next breath)
 - VCO2 (on next breath) - PaCO2 (on next breath)")
54
Treatment of Auto-PEEP with Vinsp
Longer time for exhalation, PA falls Ptp = 5 1 PA = 6 Patm = 0 Ppl = 1 1 Pel = 6 D Ppl needed to initiate inhalation: - 7

55
External PEEP Reduce inspiratory muscle load
Improve ventilator triggering 80% of PEEPi can be matched without increase PEEP tot Reduce hyperinflation by improving expiration

56
Titrating PEEP to PEEPi

57
Heliox and Obstructive Airway Disease
Low density high thermal conductivity Reduce pressure gradient in turbulent flow Administered in NIV IPPV Nebulisers Role in Asthma and COPD?

59
Ventilation in COPD/Asthma
Non Invasive Ventilation Assessment of mechanics (resistance, auto-PEEP) Pressure or volume modes? Role of PEEP Administering Bronchodilators
 Pressure or volume modes Role of PEEP. Administering Bronchodilators.")
60
Theophylline Used for OVER 50 years Lack of benefit has been shown when aggressive inhalation B2-agonist + systemic corticosteroids

61
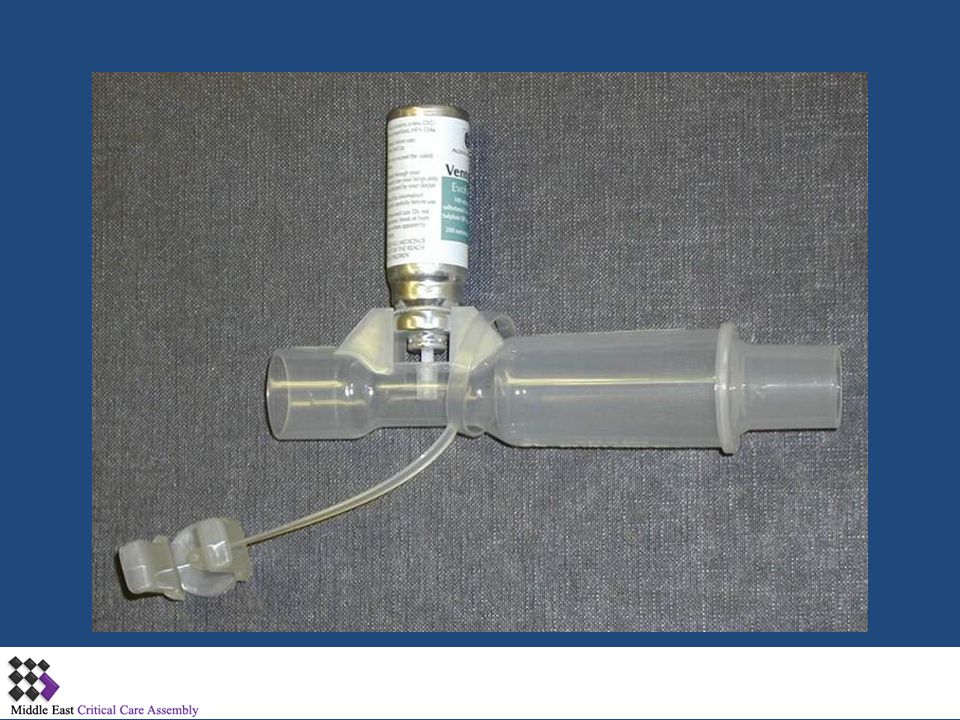
Administration of Bronchodilators

62
Administration of Bronchodilators
Nebuliser or MDI? Lung deposition of radiolabelled drug* MDI 5.6% v Nebuliser 1.2% Urinary excretion** MDI with spacer 38% MDI in line 9% Nebuliser 16% 4-10 puffs MDI effective in reducing RAW * Chest 1999; 115: **Am Rev Respir Dis 1990; 141:440–444

63
MDI adapters for use with MV circuits

65
Myopathy in Asthma Steroid myopathy Muscle relaxants
Polyneuropathy of the critically ill

66
Polyneuropathy of the critically ill
Myopathy in Asthma Proximal muscle Subacute (3 weeks) Normal CPK Steroid myopathy Distal & proximal High myoglobin High CPK Muscle relaxants Sensorimotor Polyneuropathy of the critically ill
 Normal CPK. Steroid myopathy. Distal & proximal. High myoglobin. High CPK. Muscle relaxants. Sensorimotor. Polyneuropathy of the critically ill.")
67
Principles of managing the ventilated patient with obstructive lung disease
Provide adequate support for muscle rest with adequate pH and PO2 Do not over ventilate Minimize minute volume requirements Minimize the risk of barotrauma Maintain adequate bronchial hygiene Maintain appropriate nutrition

Similar presentations