Download presentation
Presentation is loading. Please wait.

1
Adult intussusception
Gabi Gayer Assaf Harofeh Medical Center, Israel AFIIM 2008

2
Adult intussusception
Occurs infrequently Differs from childhood intussusception in: Incidence Presentation Etiology Treatment

3
Adult and childhood intussusceptions
Children Adult % of all intussusceptions Cause of obstruction Frequent Rare Etiology Idiopathic % % Identifiable cause % –90% Clinical symptoms Classic triad Non specific Treatment Mainly non-operative Surgical

4
Mechanism Lesion in the bowel wall or Irritant within the bowel lumen
may alter the normal peristaltic pattern => starting an invagination leading to intussusception

5
Pathophysiology of Intussusception
Kim YH. et al. Radiographics 2006;26:

6
Clinical findings Age: second - ninth decade Mean age ~ 50 years
Male = Female

7
Symptoms and signs Abdominal pain Nausea Vomiting Constipation
Bleeding per rectum Diarrhea Abdominal mass Fever

8
Symptoms and signs Acute – rare! Intermittent Chronic
=> making preoperative diagnosis difficult

9
Classification of Intussusception
Location enteroenteric ileocolic ileocecal colocolic

10
Classification of Intussusception
Lead point (90%?) Neoplastic ~ 65% benign malignant Non neoplastic ~ 35% No lead point (10%?)
 Neoplastic ~ 65% benign. malignant. Non neoplastic ~ 35% No lead point (10% )")
11
Lead point (90%) Neoplastic ~ 65% Benign Hamartoma- Peutz-Jehger polyp
Lipoma Leiomyoma Malignant Adenocarcinoma Lymphoma Leiomyosarcoma Metastases

12
Lead point (90%) Non Neoplastic ~ 35% Meckels' diverticulum Adhesions
Celiac disease Intestinal duplication Henoch-Schonlein purpura Infection (AIDS patients)
")
13
Lead point according to location
Small bowel Benign > Malignant Hamartoma- Peutz-Jehger polyp Lipoma Leiomyoma Metastases - melanoma Colon Malignant > Benign Adenocarcinoma Lymphoma

14
CT the most useful radiological modality
Imaging - CT CT the most useful radiological modality

15
CT Findings Typical bowel-within-bowel appearance
Thickened segment of bowel containing an eccentric crescent-like fatty area representing intussusception & mesentery

16
CT Findings Depending on the angle of the CT beam
vs. the intussusception Oblong sausage-shaped mass Round target mass Crescent: fatty mesentery

17
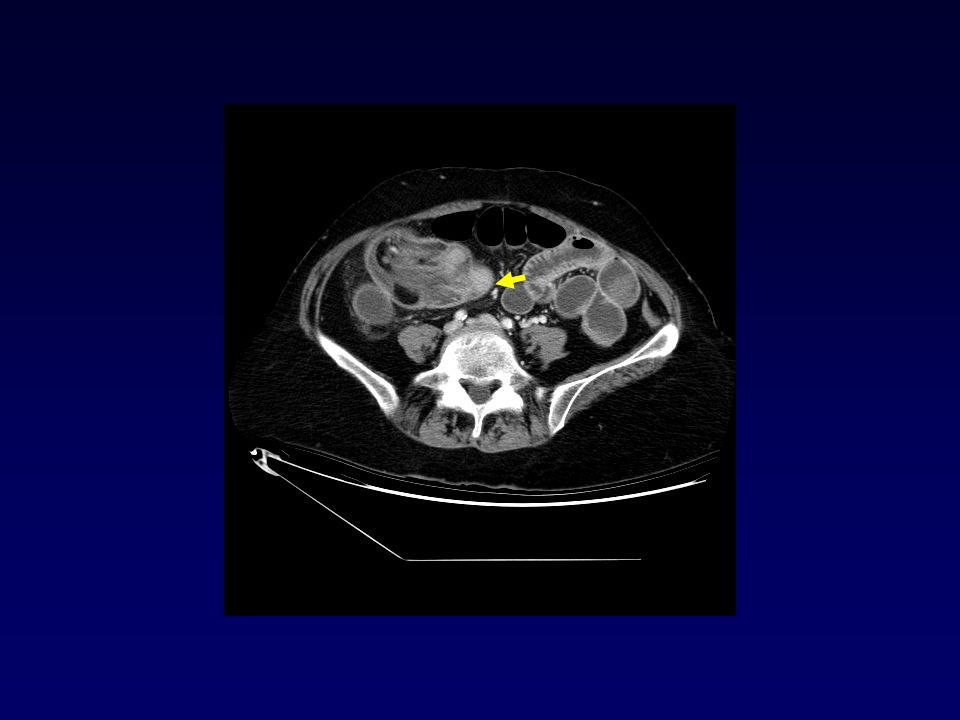
58 y old man abdominal pain, weight loss suspected acute bowel obstruction

20
Left hemicolectomy Pathology: Adenocarcinoma

21
72-year-old man with metastatic non small cell lung carcinoma s/p chemotherapy treatment

22
72-year-old man with metastatic NSCLC
5 week history of intermittent, increasingly frequent, upper abdominal pain Work up included upper and lower endoscopy notable only for some gastritis Abdominal ultrasound and CT

23
5 week intermittent upper abdominal pain

24
5 week intermittent upper abdominal pain

25
Surgery: Resection of jejunum
Intussusception in proximal half of the jejunum The bowel proximal to intussusception was moderately dilated and distally it was decompressed The site of intussusception markedly thickened Multiple large mesenteric nodes up to ~ 3 cm in diameter No evidence of metastatic disease within liver/ peritoneum No additional intra-abdominal pathology was identified Pathology: Melanoma

26
Lead point = obstruction?
NO

27
24y old man intermittent abdominal pain

28
24y old man intermittent abdominal pain

29
24y old man intermittent abdominal pain

30
Right hemicolectomy Pathology: Burkitt Lymphoma

31
56-y male with previously recurrent mantle cell lymphoma
Mantle cell lymphoma cervical and oropharyngeal involvement 10/2002 Treated chemotherapy & radiation therapy Complete response for 2 years Recurrence in the rectum and gastric body 2005 Partial response to treatment

32
56-y male with previously recurrent mantle cell lymphoma
Presenting 8/07 with fever 101.1 Right lower quadrant pain - worsening “Of note, he has complained of chronic right lower quadrant pain for the past two months” Tenderness to palpation in right midabdomen a palpable ~ 5 cm long mass Lab: neutropenia

33
56-y male with previously recurrent mantle cell lymphoma

35
Surgery and pathology Right hemicolectomy
Ileocolic intussusception related to recurrent mantle cell involvement

36
65-y right lower quadrant pain
65-year-old woman presented to the ER with several days of increasing right lower quadrant pain, nausea and vomiting Endoscopy revealed some gastritis

37
65-y right lower quadrant pain

39
Surgery Rt hemicolectomy Ileocecal intussusception
An exophytic, fungating, 5 x 3 cm mass located in the cecum Adenocarcinoma, poorly differentiated Lymph Node Status: uninvolved, 0/35

40
Can we characterize the underlying lead point?
Often not, but sometimes!

41
39y old man intermittent abdominal pain

45
Right hemicolectomy Pathology: Lipoma 5 cm causing ileo-colic intussusception

46
26-y-old woman with rectal bleeding
Symptoms for 2 months: Rectal bleeding Mucus discharge Constipation Tenesmus Grandmother with rectal cancer at age 33 Colonoscopy: a rectal mass Biopsy: adenocarcinoma

47
26-y-old woman with rectal adeno Ca

48
26-y-old woman with rectal adenocarcinoma

49
47 year old woman vague history of Crohn's disease

51
Surgery: Resection of 50cm of SB

52
Pathology: Small bowel wall with areas of hemorrhagic
necrosis of mucosa only, consistent with ischemia, probably due to intussusception No granulomas identified

53
Transient small bowel intussusception
Intussusception may be transient Intussusception detected on imaging but not confirmed by surgery but does not appear on a repeat study

54
Transient small bowel intussusception
Transient intussusception observed on SB barium follow-through studies in patients with adult celiac disease * Mechanism: loss of normal tone in the small bowel induced by the toxic effect of gluten * Transient small bowel intussusception in adult coeliac disease. Cohen MD, Lintott DJ. Clinical Radiology 1978

55
Transient small bowel intussusception
The growing use of CT for abdominal imaging => increased detection of transient intussusceptions with no underlying disease

56
Transient small bowel intussusception
Fresh diagnostic challenge Need to distinguish features of self-limiting small-bowel intussusception identified at CT

57
Transient small bowel intussusception
Retrospective review intussusception on CT or MR 33 patients with intussusception 8 years Location 29 patients had enteroenteric intussusceptions 4 intussusceptions involving the colon Etiology 10 patients (30%) had a neoplastic lead point 23 patients (70%) no neoplastic lead point - variety of causes Warshauer DM et al. Radiology 1999;212:853-60
 had a neoplastic lead point. 23 patients (70%) no neoplastic lead point - variety of causes. Warshauer DM et al. Radiology 1999;212:")
58
Transient small bowel intussusception
~ 1/3 of cases were caused by a neoplastic lead point About half of adult cases in this series were idiopathic Enteric intussusceptions in the nonneoplastic group Length - shorter (median, 4 vs 10.8 cm) Diameter - smaller (median, 3 vs 4 cm) Less likely to be associated with obstruction (4% vs 50%) Warshauer DM et al. Radiology 1999;212:853-60
 Diameter - smaller (median, 3 vs 4 cm) Less likely to be associated with obstruction (4% vs 50%) Warshauer DM et al. Radiology 1999;212:")
59
Transient small bowel intussusception
Intussusception with a neoplastic lead point compared to nonneoplastic ones significantly longer significantly larger diameter significantly more common proximal dilatation of SB Warshauer DM et al. . Radiology 1999;212:853-60

60
Transient small bowel intussusception
Retrospective study: To determine if clinical or CT findings can be used to distinguish self-limiting cases of adult small-bowel intussusception from those requiring surgery Lvoff N et al. Radiology 2003; 227:68–72

61
Transient small bowel intussusception
Retrospective computerized search of 69,040 abdominopelvic CT 4-year period 37 (0.05%) cases of adult SB intussusception 6 patients (16%) underwent surgery, all had lead-point tumors (most mets) 31 patients (84%) treated conservatively none required surgery Lvoff N et al. Radiology 2003; 227:68–72
 cases of adult SB intussusception. 6 patients (16%) underwent surgery, all had lead-point tumors (most mets) 31 patients (84%) treated conservatively. none required surgery. Lvoff N et al. Radiology 2003; 227:68–72.")
62
Distinguishing features of self-limiting transient SB intussusception
Intussusception length of 3.5 cm All 20 patients with intussusception length of <=3.5cm self-limiting 17 patients had an intussusception length > 3.5 cm 11 patients intussusception self-limiting 6 patients intussusception required surgery Lvoff N et al, Radiology 2003;227:68-72

63
Distinguishing features of self-limiting transient SB intussusception
Intussusception length The main factor in distinguishing the majority of small-bowel intussusceptions detected with CT that are self-limiting from the minority that require surgery An intussusception that is less than 3.5 cm in length is likely to be self-limiting Lvoff N et al, Radiology 2003;227:68-72

64
Transient small bowel intussusception 79 y old man following ERCP

65
Elderly lady breast Ca

66
Delayed scan

67
Elderly lady breast Ca

69
Transient small bowel intussusception
33-year-old man Precontrast scan

70
Postcontrast scan

71
Transient small bowel intussusception
33-year-old man Postcontrast scan

72
Transient small bowel intussusception 79 y old man following ERCP

74
Transient small bowel intussusception
80-year-old woman Postcontrast scan

75
Transient small bowel intussusception
Attributed to minor transient disturbances in bowel motility without clinical importance More common in the proximal small bowel, where peristaltic activity is normally greater

76
Transient small bowel intussusception
Most of these cases would not have come to attention were it not for CT being performed to evaluate unrelated disease or symptoms

77
Transient small bowel intussusception
Transient intussusceptions are, however, not necessarily idiopathic and may occur either with or without a pathological lead point

78
Transient small bowel intussusception
No lead point Lead point

79
Lead point- self limiting
Pathologic process acting as lead point Adult celiac sprue Crohn’s disease Eosinophilic enteritis Intestinal lymphoid hyperplasia – infections allergic response to various foods

80
Crohn’s disease

81
Barium follow through next day

82
Transient small bowel intussusception 45y old male with melanoma

83
Transient small bowel intussusception 45y old male with melanoma

84
Transient small bowel intussusception 45y old male with melanoma

85
Melanoma and SB intussusception
Dramatically increasing incidence of malignant melanoma, not infrequently late recurrence Unusual presentations of late gastrointestinal recurrence can be expected

86
Melanoma and SB intussusception
Melanoma is well known for its capricious clinical course in terms of metastatic behavior Melanoma shows an unusual predilection for metastasizing to small bowel A long interval between removal of primary tumor and development of metastasis

87
Melanoma and SB intussusception
Metastasis of malignant melanoma to the GI tract: 50%–60% of autopsy cases Only 2% to 5% of patients with such metastases are diagnosed while they are alive This is due to the fact that symptoms of early development are not specific but general and constitutional

88
Melanoma and SB intussusception
Metastasis to GI tract is seen most frequently in the small intestine, followed by colon, stomach, and rectum, but rare in esophagus Primary malignant melanoma originating in the small intestine is extremely rare

89
Melanoma and SB intussusception
Symptoms of SB metastasis of melanoma: chronic GI blood loss, obstruction, abdominal pain, anorexia, nausea, vomiting, weight loss Time interval between identification of melanoma and diagnosis of GI metastasis: months Aggressive surgical resection is controversial regarding its effect on prognosis

90
Treatment Not the role of the radiologist DO NOT REDUCE!
Radiologist’s role: guiding treatment Differentiating the type of intussusception

91
Intussusception without
Lead Point Transient, Spontaneously resolving No bowel obstruction =>No treatment required Intussusception with Lead Point Persistent or recurrent Bowel obstruction => Surgery required

92
Treatment Transient- no intervention However
If a tumor suspected - surgical resection

93
Treatment Resection of the intussusception without
reduction is the preferred treatment, as about half of both colonic and enteric intussusceptions are associated with malignancy

94
Adult Intussusception
Rare Pathognomonic CT features Underlying pathology – sometimes Small bowel, short segment – consider transient intussusception Colo-colic – consider malignancy

95
MERCI Thank you

96
CT Findings Oral contrast: Rim-shaped accumulation of contrast
material in the periphery of the mass

97
CT Findings Per rectum contrast:
Rim of contrast encircling the intussusceptum, analogous to the coil spring seen in enema

98
The basic facts 5% of all intussusceptions occur in adults
Account for 1% of all bowel obstructions Fact ? 70%–90% of cases have a demonstrable cause based on discharge diagnosis or surgical results

99
Etiology of Intussusception
The etiology of intussusception in the small bowel and the colon is quite different

100
Small Bowel Intussusception: Etiology
Benign lesions -Majority Benign neoplasms (lipoma, leiomyoma, hemangioma, neurofibroma) Adhesions Meckel diverticulum Lymphoid hyperplasia and adenitis Trauma Celiac disease Intestinal duplication Henoch-Schonlein purpura
 Adhesions. Meckel diverticulum. Lymphoid hyperplasia and adenitis. Trauma. Celiac disease. Intestinal duplication. Henoch-Schonlein purpura.")
101
Small Bowel Intussusception: Etiology
Malignant lesions (15% of cases) Metastatic, melanoma most common metastasis to cause intussusception Idiopathic intussusception 20%??
 Metastatic, melanoma most common metastasis to cause intussusception. Idiopathic intussusception 20%")
102
Colon Intussusception: Etiology
Malignant etiology (50%-60%) adenocarcinoma lymphoma Benign lesions (30%) lipoma, leiomyoma, adenomatous polyp, endometriosis, previous anastomosis. Idiopathic intussusception (~ 10%) Less often than in the small bowel
 adenocarcinoma. lymphoma. Benign lesions (30%) lipoma, leiomyoma, adenomatous polyp, endometriosis, previous anastomosis. Idiopathic intussusception (~ 10%) Less often than in the small bowel.")
103
26-y-old woman with rectal adeno Ca

104
26-y-old woman with rectal adeno Ca

107
A feeding tube inserted via jejunostomy
A 22-year-old man with a head injury

109
Intussusception following surgery for abdominal trauma
21 patients after trauma operated for intestinal obstruction Six (29%) intussusception cause of obstruction All males, ages years Mechanisms of injury gunshot wounds 3 stab wounds 2 blunt trauma 1 Duncan A et al. Intussusception following abdominal. J Trauma. 1987;27:
 intussusception cause of obstruction. All males, ages years. Mechanisms of injury. gunshot wounds 3. stab wounds 2. blunt trauma 1. Duncan A et al. Intussusception following abdominal. J Trauma. 1987;27:")
110
Intussusception following surgery for abdominal trauma
Interval surgery intussusception First 8 postoperative days – 4 patients 21 days – 1 patient 10 months – 1 patient Jejunojejunal intussusception - 5 patients Jejunoileal -1 Duncan A et al. Intussusception following abdominal. J Trauma. 1987;27:

111
Intussusception following surgery for abdominal trauma
Increased incidence of postoperative SB obstructions is caused by intussusception in trauma patients Duncan A et al. Intussusception following abdominal. J Trauma. 1987;27:

Similar presentations
























 bowel habit change (-) bearing down sensation PMHx. hemorrhoidectomy,>")






