Download presentation
Presentation is loading. Please wait.

1
Children with Developmental Apraxia of Speech Communication Profiles and Interventions
Laura J. Ball, Ph. D. Munroe-Meyer Institute for Genetics and Rehabilitation University of Nebraska Medical Center, Omaha

2
Demographics Onset Course Gender Prevalence Aggregation
Onset: From birth, see impairments in development of movements for speech production. Course: Often long, arduous treatments. Question if because slp’s didn’t know appropriate interventions, or if just difficult to treat. Gender: Male to female: 3 to 1 For dissertation, had 19% female (or approximately 5 to 1) Prevalence: Generally one in one thousand, not really known. Aggregation: Genetic studies show some familial transmission with certain disorders (Renpenning syndrome, Soto’s syndrome? etc.)
 Prevalence: Generally one in one thousand, not really known. Aggregation: Genetic studies show some familial transmission with certain disorders (Renpenning syndrome, Soto’s syndrome etc.)")
3
Research Classifications
Unitary Entity: isolate one characteristic that differentiates DAS from other childhood speech problems. Syndrome does not require one “necessary and sufficient” dx criterion. Subtypes:behavioral characteristics are associated with dx criteria for each of 2+ subtypes of the disorder.

4
Theoretical Perspective
Shriberg et.al., (1997a, 97b, 97c) present a schema for speech production in DAS with linguistic processing stages. 1. Input processes (auditory-temporal, perceptual) 2. Organizational processes ( representational, transformational) 3. Output processes (selection-retrieval, pre-articulatory sequencing) 4. Articulatory execution.
 present a schema for speech production in DAS with linguistic processing stages. 1. Input processes (auditory-temporal, perceptual) 2. Organizational processes ( representational, transformational) 3. Output processes (selection-retrieval, pre-articulatory sequencing) 4. Articulatory execution.")
5
DAS: Deficit in Input Processes?
Auditory-Temporal & Perceptual input processes are usually proposed from 2 general perspectives. Children with DAS have: 1. Across-the-board deficits in language processes. 2. Specific deficits in either formulation or transformation of appropriate phonological representations.

6
Robin et.al., (1993) noted that children had disordered prosody, suggesting that “impaired temporal perception could impact ability to gain information about durational aspects of prosody and add to the observed prosodic difficulties.”
 noted that children had disordered prosody, suggesting that impaired temporal perception could impact ability to gain information about durational aspects of prosody and add to the observed prosodic difficulties.")
7
DAS: Deficit in Organizational Processes?
Representational & Perceptual Organization Velleman & Strand (1994) implicate representational processing. They suggest that children with DAS “could be seen as impaired in their ability to generate & utilize frames, which would otherwise provide the mechanisms for analyzing, organizing, & utilizing information from their motor, sensory, & linguistic systems for the production of spoken language.”
 implicate representational processing. They suggest that children with DAS could be seen as impaired in their ability to generate & utilize frames, which would otherwise provide the mechanisms for analyzing, organizing, & utilizing information from their motor, sensory, & linguistic systems for the production of spoken language.")
8
Maassen, Thoonen, & Gabreels (1993): Children with DAS demonstrate a “phonological encoding disorder.”
: Children with DAS demonstrate a phonological encoding disorder.")
9
Snow, Marquardt, & Davis (1992): Children with DAS “demonstrate an apparent breakdown in the ability to perceive ‘syllableness’ and access & compare syllable representations with regard to position & structure.”
: Children with DAS demonstrate an apparent breakdown in the ability to perceive ‘syllableness’ and access & compare syllable representations with regard to position & structure.")
10
Groenen, Crul, Maassen, & Thoonen (1993): “weaker auditory memory traces” suggest perceptual discrimination tasks have diagnostic value. “The degree of dysfunction in speech production is related to the degree of dysfunction in speech perception.”

11
Transformational Organization
Morphophonemic, allophonic & sociolinguistic rules appear to be intact.

12
DAS: Deficit in Output Processes?
Pre-articulatory Sequencing (most prevalent) attributes the variability observed in speech output to deficits in pre-articulatory sequencing of the spatio-temporal movements for speech sounds.
 attributes the variability observed in speech output to deficits in pre-articulatory sequencing of the spatio-temporal movements for speech sounds.")
13
Selection-Retrieval Phonetic variability involves a lower-level deficit in motor programming, rather than retrieval of phonemic units. Walton & Pollack (1991) “motor theory”: “Although one could argue that there is a phonemic confusion in the speech of these children, one could also argue that their ability to demonstrate these contrasts is lost when their motor systems are taxed or challenged.”
 motor theory : Although one could argue that there is a phonemic confusion in the speech of these children, one could also argue that their ability to demonstrate these contrasts is lost when their motor systems are taxed or challenged.")
14
DAS is a disorder of movement
Lack consistent error production seen with developmental delay. Not result of immature sound productions, but actual motoric impairment. Dysarthria will also exhibit consistent errors, with some physical signs of weakness, paralysis, etc. DAS is a disorder of movement.

15
Diagnostic Features Speech Errors:
Differ from errors of children with developmental delay, phonological processes. Resemble errors of adult acquired apraxia (contrast between voluntary and involuntary performance, variability of errors). Differ from dysarthria, which has errors in phonation, resonance, articulation & prosody.
. Differ from dysarthria, which has errors in phonation, resonance, articulation & prosody.")
16
DAS impacts all aspects of communication
Researchers have defined DAS solely as sound production error patterns because of a need to eliminate any “outliers” in their research projects. In terms of finding a genetic determinant, a case of “pure DAS” yields a much nicer result. More recently, researchers are indicating more consensus that DAS is actually a disorder of movement and not sound production per se. As clinicians, we all know that these children exhibit a range of communication disorders that happen to include articulation errors. The articulation is frequently not consistently in error: they may produce one sound in error in a particular word one time and a completely different sound in error in that same word the next time. In addition, they may produce completely different sounds each time. It is important to note also that these children may be the ones you hear people saying “she can say it, I heard her do it once, she just doesn’t want to,” “she’s being stubborn!”, etc. Children with DAS have a disorder of movement and sequencing of the oral structures for production of sounds.

17
Why do we Communicate? Light (1988) identified four purposes of social communication: 1. expression of wants or needs, 2. transfer of information, 3. social closeness, and 4. social etiquette.

18
Important Aspects 1. DAS as a disorder of movement
2. DAS as a disorder impacting all aspects of communication

19
DAS Defined Typically defined in terms of sound production error patterns, actually a disorder of movement. Difficulty is noted with purposeful voluntary movements for speech, creating an inability to sequence speech movements in the absence of paralysis. The articulation aspect of DAS is motor in nature. It is a disorder of MOVEMENT, not in actual sound production. So as SLP’s it may be a difficult concept. We are very used to thinking in terms of individual sound production. With these children, we need to focus on the process of movements required. The reason there is so much irregularity in the child’s speech is that they don’t get the sound sequences. Look at production of similar movements with lots of drill.

20
DAS is a disorder of movement
Lack consistent error production seen with developmental delay. Not result of immature sound productions, but actual motoric impairment. Dysarthria will also exhibit consistent errors, with some physical signs of weakness, paralysis, etc. DAS is a disorder of movement.

21
Survey of SLPs Participants regional SLP’s treating DAS Profiles
children actually in treatment Perspective clinical awareness vs. “pure” research version When going through the process of reviewing the literature and identification of these aspects of communication, it occurred to me that some of the controversy regarding (Clare Waldron) DAS may be due to the varied characteristics of the children being seen in clinical practice and those being chosen for research subjects. With different goals in mind: one of the “researcher” looking for necessary and sufficient definitional characteristics and the other of “clinician” looking for the most efficaceous treatment strategy. So, we collected data from groups of SLP’s attending regional conferences on DAS and from clinicians treating children with DAS in their caseloads. At this point, we have collected information from ~ N = 50 SLP’s.
 DAS may be due to the varied characteristics of the children being seen in clinical practice and those being chosen for research subjects. With different goals in mind: one of the researcher looking for necessary and sufficient definitional characteristics and the other of clinician looking for the most efficaceous treatment strategy. So, we collected data from groups of SLP’s attending regional conferences on DAS and from clinicians treating children with DAS in their caseloads. At this point, we have collected information from ~ N = 50 SLP’s.")
22
Profiles Results of the survey showed three general profiles of children with DAS being seen for treatment. We examined: articulation/motor speech/phonological intelligibility of speech receptive/expressive language social interaction behavioral communication academic communication skills. In 100% of the children described, there were communication difficulties noted in addition to the speech articulation.

23
DAS & Communication: Characteristics
Decreased intelligibility Disordered language Social withdrawal Behavioral aggression Academic failure These characteristics have been commonly cited in the research literature and within the books directed at DAS.

24
Important Aspects… gee, notice a pattern here?
1. DAS as a disorder of movement 2. DAS as a disorder impacting all aspects of communication So to summarize to this point, the two overriding aspects found in the research reveal that….

25
Screening for DAS Address increase in referrals & diagnoses of DAS among preschool population Short administration time Organize, streamline assessment process Increase assessment efficiency Morehouse & Linderman, 2000

26
Screening for Developmental Apraxia of Speech (SDAS)
Oral Motor Movements Phoneme Stimulability Intelligibility Checklist of DAS Characteristics Increasing Word Length Multisyllabic Words Across Trials Interpretation & Recommendations Morehouse & Linderman, 2000

27
Assessment of DAS (Strand, 1998)
Neuromuscular Muscle strength, tone, & coordination Reflexes Sensory function Structural Function Structures, tissue characteristics, & sensation Range of motion, strength, coordination, speed, & ability to vary muscle tension. Assessment involves gathering large quantities of data and then sifting through the results to eliminate definite causative factors. Neuromuscular: Overall gait, muscle strength, tone, coordination, reflexes, and sensory function. Oral structural/functional: any limits of function?

28
Motor Speech Production
Simple to complex phonetic sequencing: CV, VC, CVC (vary the vowel) monosyllabic words multisyllabic words phrases sentences of increasing length Examine ability to sequence phonetic segments in various contexts. Follow simple to complex hierarchy. Might try sequence of cueing also: simultaneous presentation, immediate repetition, delayed repetition, delayed consecutive repetition. (E. Strand) Sample variety of vowels. Word repetition, words of increasing length: me meat meeting Sentence repetition, increasing length and varying phonetic complexity. Automatic vs. controlled contexts: count to 10, name particular numbers, familiar/unfamiliar phrases, Connected speech: conversation, picture description, narrative Physiological parameters: pitch: level, breaks, variation, tremor loudness: mono-, excess, decay, alternating voice quality: harsh, hoarse, breathy, strained, nasality, nasal emission respiration: forced inspiration/expiration, audible, grunt at end of expiration prosody: rate, phrasing, increase in rate with speech, variable rate, stress, short rushes of speech
 monosyllabic words. multisyllabic words. phrases. sentences of increasing length. Examine ability to sequence phonetic segments in various contexts. Follow simple to complex hierarchy. Might try sequence of cueing also: simultaneous presentation, immediate repetition, delayed repetition, delayed consecutive repetition. (E. Strand) Sample variety of vowels. Word repetition, words of increasing length: me meat meeting. Sentence repetition, increasing length and varying phonetic complexity. Automatic vs. controlled contexts: count to 10, name particular numbers, familiar/unfamiliar phrases, Connected speech: conversation, picture description, narrative. Physiological parameters: pitch: level, breaks, variation, tremor. loudness: mono-, excess, decay, alternating. voice quality: harsh, hoarse, breathy, strained, nasality, nasal emission. respiration: forced inspiration/expiration, audible, grunt at end of expiration. prosody: rate, phrasing, increase in rate with speech, variable rate, stress, short rushes of speech.")
29
Assess at Level of Breakdown
Examine any vowels NOT heard in spontaneous speech Examine CV/VC combinations, also omitting those heard in spontaneous speech Examine CVC productions, omitting those heard in spontaneous speech same 1st & last phoneme different 1st & last phoneme

30
Examine Words of Increasing Length
simultaneous production with examiner direct imitation delayed imitation

31
Examine Multisyllabic Words
simultaneous production with examiner direct imitation delayed imitation

32
Physiological functioning for speech production
Respiration Laryngeal function Resonance: Large number hyper- nasal hypo- nasal mixed nasality

33
Articulation & Phonology
What evaluation procedures would be most appropriate to address the needs of children with DAS? What evaluation procedures would be most appropriate to address the needs of children with motor-based speech disorders?

34
Intelligibility & Comprehensibility
What are the most appropriate means of assessing intelligibility in young children? How might you get a measure of a child’s comprehensibility vs. intelligibility?

35
Intelligibility/Comprehensibility
Index of Augmented Speech Comprehensibility in Children (I-ASCC) (Dowden, 1997) A non-standardized clinical measure to assess comprehensibility.
 (Dowden, 1997) A non-standardized clinical measure to assess comprehensibility.")
36
I-ASCC Hierarchy Present a picture with a verbal cue such as “What is this?” Present a picture and provide contextual cues such as “It’s a food you might eat. What is it?” Present a picture plus an embedded model such as “It’s pizza. Now you say it.” * Show Pizza overhead With the IASCC, you proceed through a hierarchy of cueing to obtain a response from the child. In addition, you provide the transcriber with a hierarchy of cues during transcription. Initially, they are presented intelligibility cues of the speech sound signal on audiotape only. After initial transcription, they are asked to play back the tape and transcribe the utterance when provided with some contextual information “It is something that children like to eat for dinner.” for a measure of comprehensibility. For example, I may show the child a picture/icon of pizza, the child names it and it is recorded. The transcriber listens once to the word & writes it, then again after reading the cue for that word. *show list of cues

38
Intelligibility Judge listens to taped utterances without contextual cues and transcribes.

39
Comprehensibility After listening to & judging the entire set of utterances without contextual cues, the listener rewinds the tape, reads a contextual cue and transcribes again.

40
Contextual Cues Something children eat at snack time.
Something children use during craft time. Something children eat for lunch. Clothing young girls wear outside. What you see children doing with a book.

41
Language What current methods exist to measure expressive language in unintelligible children? What are the most appropriate assessment procedures for assessing both receptive and expressive language in children with DAS?

42
Clinically, consider of ALL of the following:
Movement skills Receptive & expressive language skills Physical structures and functions Comprehensibility Communication repertoires in use Do the response errors appear to have a motor planning basis? Do the response errors appear to have a phonological or linguistic basis? Do the response errors appear to have a structural basis (e.g., dysarthria)? Does the child have reduced intelligibility? (e.g.,artic, respiration, phonation, & compensatory strategies.) Does the child have reduced comprehensibility? (e.g.,environment, semantic/syntactic context, familiarity & patience of listener.) Does the child communicate appropriate social interactions? Does the child communicate appropriate behavioral interactions? Does the child communicate appropriately for academic interactions, skills? Degree of motor planning vs. physical impairment Severity Intelligibility Degree DAS speech affects overall communication
 Does the child have reduced intelligibility (e.g.,artic, respiration, phonation, & compensatory strategies.) Does the child have reduced comprehensibility (e.g.,environment, semantic/syntactic context, familiarity & patience of listener.) Does the child communicate appropriate social interactions Does the child communicate appropriate behavioral interactions Does the child communicate appropriately for academic interactions, skills Degree of motor planning vs. physical impairment. Severity. Intelligibility. Degree DAS speech affects overall communication.")
43
Differential Diagnosis
Determine which characteristics are most readily apparent. Are there dominant speech characteristics? Dysarthria vs. DAS Fluency disorder vs. DAS Phonological disorder vs. DAS Developmental articulation vs. DAS

44
Research Questions What attributes of overall communication disabilities are found in children with DAS? Do clusters based on communication disabilities exist for children with DAS?

45
Methods N=36 children with DAS Screening:
DAS Screening Instrument (Blakeley, 1980) Child Social Interaction Scales (Adapted from Booth-Butterfield and Gould, 1986; Duran, 1992; Wiemann, 1977; Canary and Spitzberg, 1987; McCrosky, 1982; Christophel, 1990; and Burgoon, 1976.)
 Child Social Interaction Scales (Adapted from Booth-Butterfield and Gould, 1986; Duran, 1992; Wiemann, 1977; Canary and Spitzberg, 1987; McCrosky, 1982; Christophel, 1990; and Burgoon, 1976.)")
46
Criteria for Inclusion
Committee of 3 DAS experts rated “degree of DAS” A mean score 3, considered DAS

47
Articulation and Phonology
Do children with DAS use phonological processes? Examine consistency of productions. Khan-Lewis Phonological Analysis Articulation & prosody Goldman-Fristoe Test of Articulation Consider impact on language skills & reading development

48
Language Language sample if intelligibility allows
Comprehensive receptive & expressive Morphology & syntax Test of Auditory Comprehension of Language (III) (1998) Peabody Picture Vocabulary Test (IIIA/B) For your personal information, you may wish to videotape record and complete analysis for nonverbal/gestural interactions used by the child.
 (1998) Peabody Picture Vocabulary Test (IIIA/B) For your personal information, you may wish to videotape record and complete analysis for nonverbal/gestural interactions used by the child.")
49
Communication Social communication skills
Behavioral communication repertoires Academic communication skills Social Skills Rating System (Gresham and Elliott, 1990)
")
50
Assessment Procedures Contributing to DAS Profile Identification

51
Profile Communication Aspects
Intelligibility & Comprehensibility Language (receptive & expressive) Social Behavioral Academic In general: Determine approach appropriate to the level of motor impairment Methods address strengths and deficits Consider stimuli length, phonetic complexity, number, type of utterances Motor learning theory: Need motivation, focused attention, and prepractice. Repetitive motor drill: enough trials to create automatic processing, reinforcements that don’t take time, facilitate repeated opportunities for production. Mass practice: quick development, poor generalization ( if need child to have quick success) Distributed practice: takes longer to develop but get better generalization Knowledge of results: give info about movement performance, not too specific (lose the anatomy cues!)
 Social. Behavioral. Academic. In general: Determine approach appropriate to the level of motor impairment. Methods address strengths and deficits. Consider stimuli length, phonetic complexity, number, type of utterances. Motor learning theory: Need motivation, focused attention, and prepractice. Repetitive motor drill: enough trials to create automatic processing, reinforcements that don’t take time, facilitate repeated opportunities for production. Mass practice: quick development, poor generalization ( if need child to have quick success) Distributed practice: takes longer to develop but get better generalization. Knowledge of results: give info about movement performance, not too specific (lose the anatomy cues!)")
52
Cluster Analysis Measure used to examine large data set and determine if there are patterns of similarity among the variables. Results in “dendrogram” (see diagram) which depicts the total data set and each stage of grouping the most similar data points (or in this case, children with DAS) into clusters.
 which depicts the total data set and each stage of grouping the most similar data points (or in this case, children with DAS) into clusters.")
53
Cluster Analysis Confirmatory measure of profiles previously obtained (Ball & Beukelman, 1998). Classifies sample into smaller number of mutually exclusive groups based on similarity. Variables analyzed simultaneously to discover underlying structure.

54
Significant Discriminant Functions

55
Profile Identification Procedures
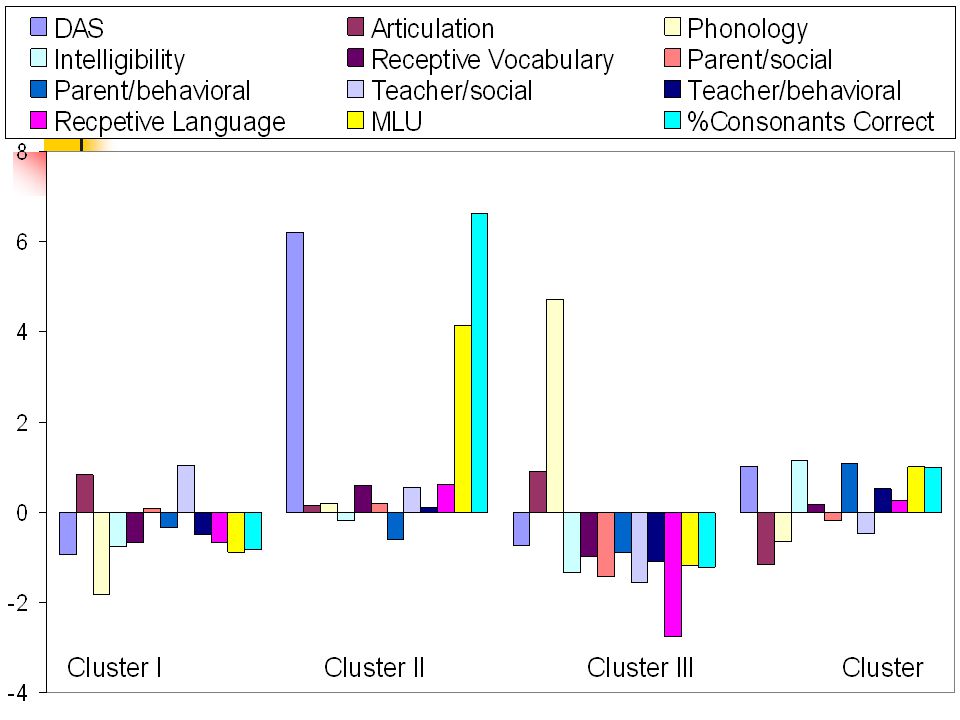
Discriminant Function Structure Weights Articulation-oriented Function 1 Articulation DAS Intelligibility MLU PCC Language-oriented Function 2 Parent/behavior Language comprehension .434 Receptive Vocabulary Phonological skills

56
Cluster One, n = 12 high # articulation errors
high social skill ratings high DAS scores (very DAS) few consistent phonological processes low intelligibility low vocabulary scores high disruptive behaviors low receptive language scores small MLU low PCC
 few consistent phonological processes. low intelligibility. low vocabulary scores. high disruptive behaviors. low receptive language scores. small MLU. low PCC.")
57
Cluster Two, n = 12 high # articulation errors
high social skills ratings less DAS many consistent phonological processes low intelligibility high vocabularyscores few disruptive behaviors high receptive language scores high MLU high PCC

58
Cluster Three, n = 1 high # articulation errors
many consistent phonological processes more DAS low intelligibility low vocabulary scores less socially interactive many behavioral disruptions low receptive language skills low MLU low PCC

59
Cluster Four, n = 11 low # articulation errors
few consistent phonological processes less DAS high intelligibility high vocabulary scores less socially interactive few behavioral disruptions high receptive language scores high MLU high PCC

60
Cluster Status on Significant Variables
I II IV High Articulation Err; Low Language X X Low Articulation Err; High Language X High Behavior Probs.; Low Language X X Low Behavior Probs.; High Language X

62
Intervention

63
Motor Learning Theory Motor learning occurs as a result of experience & practice Relevant factors: Precursors to Motor Learning Conditions of Practice Knowledge of Results Effects of Rate

64
Motor Learning: Prepractice
The prepractice portion of a therapy session involves: Motivation make the tasks seem important set goals with the child with standard to achieve not just “do the best you can” Focused Attention

65
General Idea of Task understand task clearly ways they will learn
keep instructions simple; focus on 1-2 important aspects of movement. DO NOT OVERINSTRUCT

66
Observational Learning
modeling & demonstration with pictures, videotapes, and live demos show the child the movements a few times covering all stimuli being targeted in the session be wary of verbal instructions

67
Establish Reference of Correctness
auditory feedback i.e., for /pa/, may have lip closure as correct to begin, then later move to correct articulation

68
Motor Learning: Practice
Knowledge of Performance Knowledge of Results summary immediate Repetitive Practice mass distributed

69
Knowledge of Performance (KP)
Feedback about the correctness of a particular movement pattern re: accuracy of production. e.g., “I heard you say ….”

70
Knowledge of Results (KR)
Feedback about the outcome of a movement pattern re: environmental goal. e.g., “Yes, you got it!” “No, that’s not quite it.”

71
Avoid extraneous activity (speaking, movements by clinician/child) during the period between the response & when you deliver KR, also after KR
 during the period between the response & when you deliver KR, also after KR")
72
Summary KR is better than immediate KR, better to wait until several (easier wait 15, difficult wait 3-5) responses are obtained
 responses are obtained")
73
Conditions of Motor Speech Practice (DAS)
Repetitive Practice need enough trials/session to allow motor learning to occur & become habituated to automatic use reinforcements that don’t take time develop activities that facilitate repeated opportunities for production of target movement patterns

74
Mass vs. Distributed Practice
decision depends on severity and type mass yields quick development of accurate production distributed requires longer time, but get better generalization direct imitation delayed imitation

75
Examine Sentences of Increasing Length
direct imitation with repeated attempts

76
Speech Practice for DAS
Intensive treatment is required Large number of movement repetitions required (no fewer than 20) Come to neutral position between attempts (rest), do NOT divide into component parts Progress through hierarchy of task difficulty Treat rhythm, stress & intonation to coincide with articulation drills
 Come to neutral position between attempts (rest), do NOT divide into component parts. Progress through hierarchy of task difficulty. Treat rhythm, stress & intonation to coincide with articulation drills.")
77
Augmentative and Alternative Communication Children with DAS

78
Integrating AAC and Natural Speech
Extent of AAC use depends upon the communication load that can be carried by natural speech. Extent of AAC use will vary from child to child. Extent of AAC use will vary for a child depending on the communication goal.

79
Lindblom Model of Mutuality
Rich Information from the acoustic signal (Intelligibility) Poor Poor Signal-Independent Rich Higher Comprehensibility Lower Comprehensibility
 Poor. Poor Signal-Independent Rich. Higher Comprehensibility. Lower Comprehensibility.")
80
Intelligibility Estimates
Mother % Grandmother % School SLP % Classroom teacher % AAC Specialist %

81
AAC Use & Intelligibility of Children with DAS
N = 36 children confirmed with DAS M = 6 years, 1 month age M = 44% intelligibility Range of intelligibility from 0 to 97% N = 1 child using AAC at time of evaluation for DAS

82
Use of AAC systems by Children with DAS (Cumley, 1997)
Participants were children with severe phonological disorder and/or DAS N = 16 Children 3 yrs, 5 months to 7 yrs, 5 months

83
Procedures DAS children with a range of intelligibility were taught to use an AAC technique Children engaged in play situations Interactions were video recorded and analyzed

84
Research Design ABA Design: 1. No AAC Board Present
2. Treatment Condition with AAC Board Present 3. Post-treatment Condition with AAC Board Present

85
Results Increase comprehensible messages
Increased successful communication repairs Children with most severe speech disorders used AAC most frequently

86
AAC use did not decrease the number of speech attempts!!!
AAC use reduced the number of gestures. AAC was used primarily to resolve communication breakdowns.

87
Communication Goals Establishing & maintaining Conversation
Small talk Information sharing Language learning Participation Education & Recreation Social memberships Establishing & maintaining Wants & Needs

88
Multimodal Considerations
Communicative contexts Communicative goals Intent of communication situation Immediate & future communication needs Support development of skills AAC multimodalities: help with multiple disabilities encountered with DAS. Children with more severe intelligibility were more likely to use AAC (Cumley, 1998) Limb apraxia: sign language may be a problem Co-occurring language disorders: traditional orthography may be a problem Social/behavioral disorders: may be due to communication frustration Modality options: natural speech gestures sign language low tech symbol boards-- remnant books, communication dictionaries, community based notebooks, symbol communication boards. high tech voice output communication device--Wolf, Macaw, Voice in the Box, AlphaTalker, etc. Sharp memo writer, etc. “The use of aided or unaided techniques that successfully support natural speech attempts and facilitate the access and participation in communication interactions.” (Cumley & Swanson, 1992) Need easy access, portability, support communication intent & natural speech.
 Limb apraxia: sign language may be a problem. Co-occurring language disorders: traditional orthography may be a problem. Social/behavioral disorders: may be due to communication frustration. Modality options: natural speech. gestures. sign language. low tech symbol boards-- remnant books, communication dictionaries, community based notebooks, symbol communication boards. high tech voice output communication device--Wolf, Macaw, Voice in the Box, AlphaTalker, etc. Sharp memo writer, etc. The use of aided or unaided techniques that successfully support natural speech attempts and facilitate the access and participation in communication interactions. (Cumley & Swanson, 1992) Need easy access, portability, support communication intent & natural speech.")
89
Focus on Communicative Competence
Theme-specific boards Picture/symbol dictionary Remnant books Voice output communication aids Collaborate roles & responsibilities for each partner Establish initiation & repair of breakdowns)
")
90
AAC Strategies Sign Low-tech (situation specific)
Portable digitized speech devices (situation specific) Portable general purpose devices
 Portable general purpose devices.")
91
AAC Evaluation Why children with DAS are difficult to augment
typically ambulatory have developed alternative, often unique communication strategies may have intact cognitive skills language development ongoing may have poor literacy skills

92
AAC Device Specifications
Portability Comprehensive system high tech low tech Cover extensive vocabulary demands Minimize sequencing demands Teach sequencing skills Allow & facilitate language development

93
Family Concerns re: DAS
Qualitative Research Project Garn-Nunn & Katz, 2000 Obtained postings daily from APRAXIA-KIDS listserve Apparent Themes Diagnosis Treatment Securing Treatment Personal

94
Family Diagnostic Concerns
26% of postings Varying descriptive terms Nature of problem Concomitant problems Importance of Early Diagnosis SLP crucial to success Garn-Nunn & Katz, 2000

95
Family Treatment Concerns
28% of postings Importance of speech motor practice Sign language, AAC facilitate speech early Parents intensively involved with treatment Changing nature of treatment Educational concerns Garn-Nunn & Katz, 2000

96
Family Concerns: Securing Treatment Services
22% of postings Intensive treatment, long period of time Secure different sources of treatment IEP procedures, goals, availability of services Private insurance issues Parent advocacy training, IDEA Garn-Nunn & Katz, 2000

97
Family Personal 17% of postings Success stories, thanks, encouragement
Failures, venting Explaining DAS to others & to child Local support groups Garn-Nunn & Katz, 2000

98
Case Study Walt, 10 year 6 month old male
Regular 4th grade classroom Intelligibility <50% to unfamiliar listener Diagnosed with DAS in 1998 8 years of traditional articulation-oriented speech therapy Past evaluation, recommendations

99
Assessment Results Language TACL-3 PPVT-III
Receptive subtests from CELF-R MLU

100
Articulation/Phonology
GFTA KLPA Screening Test for Developmental Apraxia of Speech (Blakeley, 1980) Percent of Consonants Correct Motor Speech Tasks
 Percent of Consonants Correct. Motor Speech Tasks.")
101
Intelligibility/Comprehensibility
Social Communication Social Skills Rating System(Gresham & Elliott, 1990) (AGS) Child Social Interaction Scale Intelligibility/Comprehensibility I-ASCC
 (AGS) Child Social Interaction Scale. Intelligibility/Comprehensibility. I-ASCC.")
102
AAC Assessment for Walt
Examine current communication and communication needs parent & child interview speech evaluation results communication abilities understands symbols for communication emerging literacy skills

103
Physical Status ambulatory, active good fine motor control
hearing and vision WNL

104
Walt’s Communication Device
Lightweight & portable Durable Extensive vocabulary Support emerging literacy skills Support developing language Allow for novel message generation Good quality voice output for communication in a variety of contexts

105
Walt’s Communication System
DynaMyte (DynaVox Systems, Inc) Topic Boards Letter Board Remnant book Natural speech
 Topic Boards. Letter Board. Remnant book. Natural speech.")
106
Classroom Recommendations
Provide multiple avenues of communication Computer supported literacy options Phonetic based word generation (Intellikeys) Story reading (Living Books, Intellikeys) Story writing (Write:Outloud, CoWriter) Organizational software (Inspiration)
 Story reading (Living Books, Intellikeys) Story writing (Write:Outloud, CoWriter) Organizational software (Inspiration)")
107
Speech Therapy Recommendations
Frequent treatment sessions (daily) Brief treatment sessions (15 min) Motor learning concepts stressed knowledge of results knowledge of performance distributed practice Provide tactile, visual, & verbal feedback
 Brief treatment sessions (15 min) Motor learning concepts stressed. knowledge of results. knowledge of performance. distributed practice. Provide tactile, visual, & verbal feedback.")
108
References Bradford & Dodd (1996). Do all speech-disordered children have motor deficits? Clinical Linguistics and Phonetics, 10(2), Davis, B. (1998a). Differential diagnosis of developmental apraxia. Newsletter: ASHA Special Interest Division 1: Language Learning and Education, 5(2), 4-7. Hayden, D.(1994). Differential diagnosis of motor speech dysfunction in children. Clinics in Communication Disorders, 4(2), Hayden & Square (1999). Verbal Motor Production Assessment for Children (VMPAC). The Psychological Corporation: A Harcourt Assessment Company
. Differential diagnosis of developmental apraxia. Newsletter: ASHA Special Interest Division 1: Language Learning and Education, 5(2), 4-7. Hayden, D.(1994). Differential diagnosis of motor speech dysfunction in children. Clinics in Communication Disorders, 4(2), Hayden & Square (1999). Verbal Motor Production Assessment for Children (VMPAC). The Psychological Corporation: A Harcourt Assessment Company.")
109
More References Cumley, G. (1997). Introduction of an augmentative and alternative modality: Effects on the quality and quantity of communication interactions of children with severe phonological disorders. Unpublished Doctoral Dissertation, University of Nebraska-Lincoln. Davis, B., Jakielski, K., & Marquardt, T. (1998). Developmental apraxia of speech: Determiners of differential diagnosis. Clinical Linguistics and Phonetics, 12(1), Dowden, P. (1997). Augmentative and Alternative Communication Decision Making for Children with Severely Unintelligible Speech. AAC, 13(1),
. Introduction of an augmentative and alternative modality: Effects on the quality and quantity of communication interactions of children with severe phonological disorders. Unpublished Doctoral Dissertation, University of Nebraska-Lincoln. Davis, B., Jakielski, K., & Marquardt, T. (1998). Developmental apraxia of speech: Determiners of differential diagnosis. Clinical Linguistics and Phonetics, 12(1), Dowden, P. (1997). Augmentative and Alternative Communication Decision Making for Children with Severely Unintelligible Speech. AAC, 13(1),")
110
More References Hall, P., Jordan, L., & Robin, D. (1993). Developmental apraxia of speech: Theory and clinical practice. Austin, TX: Pro-ed. McNeil, M., Robin, D., & Schmidt, R. (1997). Apraxia of Speech: Definition, differentiation, and treatment. In M. McNeil (Ed.), Clinical management of sensorimotor speech disorders (p. 394). New York: Thieme. Shriberg, L., Austin, D., Lewis, B., McSweeny, J., & Wilson, D. (1997a). The Percentage of Consonants Correct (PCC) metric: Extensions and reliability data. JSLHR, 40(4),
. Apraxia of Speech: Definition, differentiation, and treatment. In M. McNeil (Ed.), Clinical management of sensorimotor speech disorders (p. 394). New York: Thieme. Shriberg, L., Austin, D., Lewis, B., McSweeny, J., & Wilson, D. (1997a). The Percentage of Consonants Correct (PCC) metric: Extensions and reliability data. JSLHR, 40(4),")
111
More References Shriberg, L., Aram, D., & Kwiatkowski, J. (1997a). Developmental apraxia of speech I: Descriptive and theoretical perspectives. JSLHR, 40(2), Shriberg, L., Aram, D., & Kwiatkowski, J. (1997b). Developmental apraxia of speech II: Toward a diagnostic marker. JSLHR, 40(2), Shriberg, L., Aram, D., & Kwiatkowski, J. (1997c). Developmental apraxia of speech III: A subtype marked by inappropriate stress. JSLHR, 40(2), Strand, E. (1998). Treatment of developmental and acquired apraxia of speech. In D. Beukelman & K. Yorkston (Eds.), Motor speech disorders. Baltimore: Brookes.
. Developmental apraxia of speech I: Descriptive and theoretical perspectives. JSLHR, 40(2), Shriberg, L., Aram, D., & Kwiatkowski, J. (1997b). Developmental apraxia of speech II: Toward a diagnostic marker. JSLHR, 40(2), Shriberg, L., Aram, D., & Kwiatkowski, J. (1997c). Developmental apraxia of speech III: A subtype marked by inappropriate stress. JSLHR, 40(2), Strand, E. (1998). Treatment of developmental and acquired apraxia of speech. In D. Beukelman & K. Yorkston (Eds.), Motor speech disorders. Baltimore: Brookes.")
112
More References Strand, E. A. (1995). Treatment of motor speech disorders in children. Seminars in Speech and Language, 16(2), Shriberg, L., Austin, D., Lewis, B., McSweeny, J., & Wilson, D. (1997b). The Speech Disorders Classification System (SDCS): Extensions and lifespan reference data. JSLHR, 40(4), Caruso & Strand (1999). Clinical Management of Motor Speech Disorders in Children. NY: Thieme. Beukelman, D., & Mirenda, P. (1998). Augmentative and Alternative Communication. (2nd ed.). Baltimore: Brookes.
. The Speech Disorders Classification System (SDCS): Extensions and lifespan reference data. JSLHR, 40(4), Caruso & Strand (1999). Clinical Management of Motor Speech Disorders in Children. NY: Thieme. Beukelman, D., & Mirenda, P. (1998). Augmentative and Alternative Communication. (2nd ed.). Baltimore: Brookes.")
Similar presentations


















. Any code employing.>")

