Download presentation
Presentation is loading. Please wait.

1
What’s new in EP. Say no to drugs
What’s new in EP? Say no to drugs? Lionel Faitelson MD FACC FHRS Tucson Heart Group TMC Cardiovascular Symposium 2012

2
New devices for arrhythmias?
Anti-arrhythmic drugs: VT and VF Defibrillators ICDs; ablation Anti-arrhythmic drugs: SVT and AFL and AF Ablation Anti-heart failure drugs Biventricular pacemakers and ICDs Anticoagulant drugs in AF: NEW Alternatives to anticoagulant drugs NEW

3
AF: Managing the LA appendage
Relevance Magnitude of AF issue Risk scores and anticoagulant therapies Surgical options Percutaneous options Lariat Watchman Amplatzer cardiac plug Other

4
Atrial Fibrillation Update 2012
6.4 million San Francisco 700,000 Philadelphia 1.5 million (H.Weitz MD) Miami 400,000 Los Angeles 3.8 million
 Miami 400,000. Los Angeles 3.8 million.")
5
Atrial Fibrillation Update 2035
11.4 million Boston 600,000 Philadelphia 1.5 million San Francisco 700,000 Chicago 2.8 million Houston 2 million Los Angeles 3.8 million

6
Atrial fibrillation treatment

7
March 2010: 1,980,000 hits March 2011: 2,550,000 hits
Atrial fibrillation March 2010: 1,980,000 hits March 2011: 2,550,000 hits January 2012: 9,500,000 hits

8
AF: Public awareness September 2012 is Atrial Fibrillation Awareness Month

9
How do we determine stroke risk ?
CHADS2 (Gage, et al.: JAMA 2001) Congestive heart failure - 1pt Hypertension - 1pt Age > pt Diabetes - 1pt Stroke or TIA pts 0 points – low risk ( strokes per 100 patient years) 1-2 points – moderate risk ( strokes per 100 patient years) > 3 points – high risk ( strokes per 100 patient years)
 Congestive heart failure - 1pt. Hypertension - 1pt. Age > pt. Diabetes - 1pt. Stroke or TIA - 2 pts. 0 points – low risk ( strokes per 100 patient years) 1-2 points – moderate risk ( strokes per 100 patient years) > 3 points – high risk ( strokes per 100 patient years)")
10
How do we determine stroke risk ?
CHADS2 (Gage, et al.: JAMA 2001) Congestive heart failure - 1pt Hypertension - 1pt Age > pt Diabetes - 1pt Stroke or TIA pts 0 points – low risk ( strokes per 100 patient years) 1-2 points – moderate risk ( strokes per 100 patient years) > 3 points – high risk ( strokes per 100 patient years)
 Congestive heart failure - 1pt. Hypertension - 1pt. Age > pt. Diabetes - 1pt. Stroke or TIA - 2 pts. 0 points – low risk ( strokes per 100 patient years) 1-2 points – moderate risk ( strokes per 100 patient years) > 3 points – high risk ( strokes per 100 patient years)")
11
Lip Y, et al. Chest 2010, 137(2):263
:263")
12
Lip Y, et al. Chest 2010, 137(2):263
:263")
13
CHADS2 vs. CHA2DS2VASc CHADS2 score 0: 1.4% events CHA2DS2-VASc score 0: 0 events CHA2DS2-VASc score 1: 0.6% events CHA2DS2-VASc score 2: 1.6 events

15
Non-Valvular Atrial Fibrillation Stroke Prevention Medical Rx
Warfarin Problematic Narrow therapeutic window Multiple drug-drug/drug-food interactions Genetic variability Long half-life PCI issues – triple therapy Compliance Contraindications Bleeding risks

16
Non-Valvular Atrial Fibrillation Warfarin Use in AF Patients by Age
% Only 55% of AF patients with no contraindications have evidence of warfarin use in previous 3 months Other studies cite warfarin use in AF patients from 17-50% Elderly patients with increased absolute risk least likely to be taking warfarin Contraindications 30-40% Ann Int Med 131(12), 1999
,")
17
Atrial fibrillation 2009 Target INR 2-3

18
Non-Valvular Atrial Fibrillation Adequacy of Anticoagulation in Clinic
Low INR <1.6 Efficacy 4-fold Therapeutic INR 2-3 High INR >3.2 % Bungard: Pharmacotherapy 20:1060, 2001

19
Non-Valvular Atrial Fibrillation Stroke Pathology
Major fatal bleed with age >75 = 3%/year (30% over 10 years) Intracranial hemorrhage %/100 patient-years 3% in INR >4.0 10% if INR >4.5 Brass. Stroke 28(12), 1997 VanWalraven: JAMA 288, 2002
 Intracranial hemorrhage %/100 patient-years. 3% in INR > % if INR >4.5. Brass. Stroke 28(12), 1997 VanWalraven: JAMA 288,")
20
Non-Valvular Atrial Fibrillation Stroke Pathology
Insufficient contraction of LAA leads to stagnant blood flow Most likely culprit: embolization of LAA clot 90% of thrombus found in LAA TEE-based risk factors Enlarged LAA Reduced inflow and outflow velocities Spontaneous Echo contrast Blackshear: Ann Thoracic Surg 61, 1996 Johnson: Eur J Cardiothoracic Surg 17, 2000 Fagan: Echocardiography 17, 2000

21
Warfarin Effective Reversible Inexpensive Slow onset of action
Regular monitoring Food interraction Medication interraction Difficult titration-regular dose adjustments

22
Warfarin Effective Reversible Inexpensive Slow onset of action
Regular monitoring Food interraction Medication interraction Difficult titration-regular dose adjustments

24
RELY Dabigatran 110 mg twice daily
Equal to warfarin in stroke prevention Warfarin 1.69%/yr – dabigatran (110mg) 1.53%/yr Less bleeding than warfarin Warfarin 3.36%/year – dabigatran (110mg) 2.71%/yr Dabigatran 150 mg twice daily More effective than warfarin in stroke prevention Dabigatran (150mg) 1.11%/yr Equivalent bleeding to warfarin less hemorrhagic stroke than warfarin
 1.53%/yr. Less bleeding than warfarin. Warfarin 3.36%/year – dabigatran (110mg) 2.71%/yr. Dabigatran 150 mg twice daily. More effective than warfarin in stroke prevention. Dabigatran (150mg) 1.11%/yr. Equivalent bleeding to warfarin. less hemorrhagic stroke than warfarin.")
25
ACC AHA HRS Afib Focused Update (Dabigatran), March 2011
Non-inferior to warfarin re thromboembolism (afib) Caution when CrCl < 30ml/min Increased dabigatran levels with amiodarone, verapamil Half life hours No reversal re hemorrhage dialysis ? shelf life once bottle opened (FDA alert March 30, 2011) Tablets must stay in manufacturer’s container Label: discard product 30 days after opening container Coagulation testing ??? aPTT, dilute thrombin time
 Caution when CrCl < 30ml/min. Increased dabigatran levels with amiodarone, verapamil. Half life hours. No reversal re hemorrhage. dialysis. shelf life once bottle opened (FDA alert March 30, 2011) Tablets must stay in manufacturer’s container. Label: discard product 30 days after opening container. Coagulation testing aPTT, dilute thrombin time.")
27
Dabigatran compared to control (warfarin, enoxaparin, placebo)
Increased absolute risk of MI or ACS 0.27% Increased relative risk of MI or ACS 33%

28
As effective or better than warfarin
Rivaroxaban Once daily As effective or better than warfarin Less hemorrhagic stroke than warfarin Similar reduction in ischemic stroke Less bleeding than warfarin No routine lab testing No reversal Half life 5-9 hours Coagulation testing: aPTT Discontinuation : increased stroke

29
Apixaban Twice daily As effective or better than warfarin
Less hemorrhagic stroke than warfarin Similar reduction in ischemic stroke Less bleeding than warfarin Lower overall mortality No routine lab testing No reversal Half life 8-15 hours Coagulation testing: PT, aPTT

30
New anticoagulants Short half life – less bleeding
Subtherapeutic if misses one or two doses Lack of need for routine monitoring No standard available test to asses if anticoagulated Generally safer than warfarin No antidote ??? Dabigatran Cost of medication Overall cost of care

31
How about Clopidogrel + Aspirin ?
N Engl J Med online publication March 31, 2009

32
How about Clopidogrel + Aspirin ?
stroke 3.4% per year major bleed 1.27% per year Aspirin + clopidogrel: stroke 2.4% per year major bleed 2.0% per year Warfarin still first line ? Role of aspirin + clopidogrel N Engl J Med online publication March 31, 2009

33
LAA: Focus of interest in AF
Anticoagulants contra-indicated in 14 – 44% AF patients Stroke risk 2-5% even with therapeutic INR LAA – 90% of thrombi in nonvalvular nonrheumatic AF LAA volume 0.77 – cc LAA variable anatomy – multimodality imaging Luis, Roper et al; Cardiology Research and Practice 2012

34
LAA: Surgical options Excision with oversew or staples
Exclusion with clips or sutures LAA Occlusion Study: success 45-72% LAA Surgery: excision 73% > exclusion 23% LAA Atriclip: EXCLUDE trial: 98% success Current surgical practice

35
History of Suture Closure
1955 1949 1947 1985 2000 2011 Resection of the Left Auricular Appendix A Prophylaxis for Recurrent Arterial Emboli JOHN L. MADDEN, M.D. Department of Surgery, Long Island College of Medicine, Kings County Hospital, Brooklyn , NY Amputation of the Canine Atrial Appendages Hellerstein, HK SYSTEMIC EMBOLISM AND LEFT AURICULAR THROMBOSIS IN RELATION TO MITRAL VALVOTOMY BY AND J. R. BELCHER, M.S., F.R.C.S. Surgeon, London Chest Hospital; Assistant Thoracic Surgeon, the Middlesex Hospital USE OF THE SURGICAL STAPLER TO OBLITERATE THE LEFT ATRIAL APPENDAGE Laurence H. Coffin, M.D., F.A.C.S., Burlington, VT Appendage Obliteration to Reduce Stroke in Cardiac Surgical Patients with Atrial Fibrillation Division of Cardiovascular Diseases, Mayo Clinic Jacksonville FL & Mayo Clinic, Rochester, MN JL Blackshear, MD, JA Odell, FGRCS(Ed) Ligation of the Left Atrial Appendage Using an Automatic Stapler VJ DiSesa, S Tam, LH Cohn Division of Cardiac Surgery, Brigham & Women’s Hospital, Boston, MA
 Ligation of the Left Atrial Appendage Using an Automatic Stapler. VJ DiSesa, S Tam, LH Cohn. Division of Cardiac Surgery, Brigham & Women’s Hospital, Boston, MA.")
37
LAA: Lariat Prospective study; 82 pts; 3 month FU
Indications: AF; warfarin intolerance or CI, or embolic event on warfarin 96% of pts with successful closure have closure at 1 month Need epicardial and endocardial access (CABG, XRT, valve surgery, pericarditis) Unsuitable if pericardial adhesions present FDA and CE approved Lee at al; Heart Rhythm 2011
 Unsuitable if pericardial adhesions present. FDA and CE approved. Lee at al; Heart Rhythm")
38
Pre-Clinical Results Objective
Evaluate safety & effectiveness in canine model of percutaneous LAA closure with the LARIAT N=26 canines Attempts to Capture 1 attempt: 23/26 ( 88%) 2 attempt: 3/26 ( 12%) Complete Acute Closure: 26/26 (100%) 7d Closure: /3 (100%) 30d Closure: /3 (100%) 90d Closure: /4 (100%) Histological Examination (all) Inflammatory response: /10 ( 0%) Complete Endothelioization: 10/10 (100%) Circ Cardiovasc Interv: June 2010
 2 attempt: 3/26 ( 12%) Complete Acute Closure: 26/26 (100%) 7d Closure: 3/3 (100%) 30d Closure: 3/3 (100%) 90d Closure: 4/4 (100%) Histological Examination (all) Inflammatory response: 0/10 ( 0%) Complete Endothelioization: 10/10 (100%) Circ Cardiovasc Interv: June")
39
Clinical Results – PLACE I
Total Patients N=13 AF History Persistent 12 (92%) Flutter ( 8%) Age Avg: 57.3; Hi 64, Low 43 Sex M = 8 (62%) Type Procedure LAA w/ MVR (15%) LAA w/ ablation 10 (77%) Ablation w/ LAA 1 ( 8%) Type Access Median Sternotomy 2 (15%) Minimally Invasive (15%) Percutaneous (70%) Intent to Treat 12/13 (92%) Acute Closure 12/12 (100%) Complications 1/13 (8%) non-serious (anatomic) Procedural Times Avg: 85.7 min; Median min Heart Rhythm: 2011:8:
 Flutter 1 ( 8%) Age. Avg: 57.3; Hi 64, Low 43. Sex. M = 8 (62%) Type Procedure. LAA w/ MVR 2 (15%) LAA w/ ablation 10 (77%) Ablation w/ LAA 1 ( 8%) Type Access. Median Sternotomy 2 (15%) Minimally Invasive 2 (15%) Percutaneous 9 (70%) Intent to Treat. 12/13 (92%) Acute Closure. 12/12 (100%) Complications. 1/13 (8%) non-serious (anatomic) Procedural Times. Avg: 85.7 min; Median min. Heart Rhythm: 2011:8:")
40
Closure Without Compromise
LAA Pre-procedure 30 day Post-procedure

42
PLACETM Procedure Permanent Ligation Approximation Closure and Exclusion

43
PLACETM Procedure

44
Clinical Results – Confidence in Closure
In a single center, non randomized study(PLACE II)*, 85 patients underwent closure of their left atrial appendage using the LARIAT Suture Delivery Device and accessories. Patients were followed at 1 day, 30 days, 90 days and 1 year with transesophageal echocardiography to determine closure quality. The results were as follows: Intent-to-Treat 85/89 (96%) Adverse Events (defined as access related or device failure) 3/89 (3.3%)** Access 3/89 (3.3%) Device 0/89 (0.0%) Closure (defined as < 1mm residual flow) 1 day 81/85 (95%) 30 day 81/85 (95%) 90 day 77/81 (95%) 1 year 65/66 (98%) * PLACE II Clinical Study -KBET/90/B/2008; Dec Jun Submitted for publication. ** All non-serious: 2 pericardial access related. 1 transseptal access related.
*, 85 patients underwent closure of their left atrial appendage using the LARIAT Suture Delivery Device and accessories. Patients were followed at 1 day, 30 days, 90 days and 1 year with transesophageal echocardiography to determine closure quality. The results were as follows: Intent-to-Treat. 85/89 (96%) Adverse Events (defined as access related or device failure) 3/89 (3.3%)** Access 3/89 (3.3%) Device 0/89 (0.0%) Closure (defined as < 1mm residual flow) 1 day 81/85 (95%) 30 day 81/85 (95%) 90 day 77/81 (95%) 1 year 65/66 (98%) * PLACE II Clinical Study -KBET/90/B/2008; Dec Jun Submitted for publication. ** All non-serious: 2 pericardial access related. 1 transseptal access related.")
45
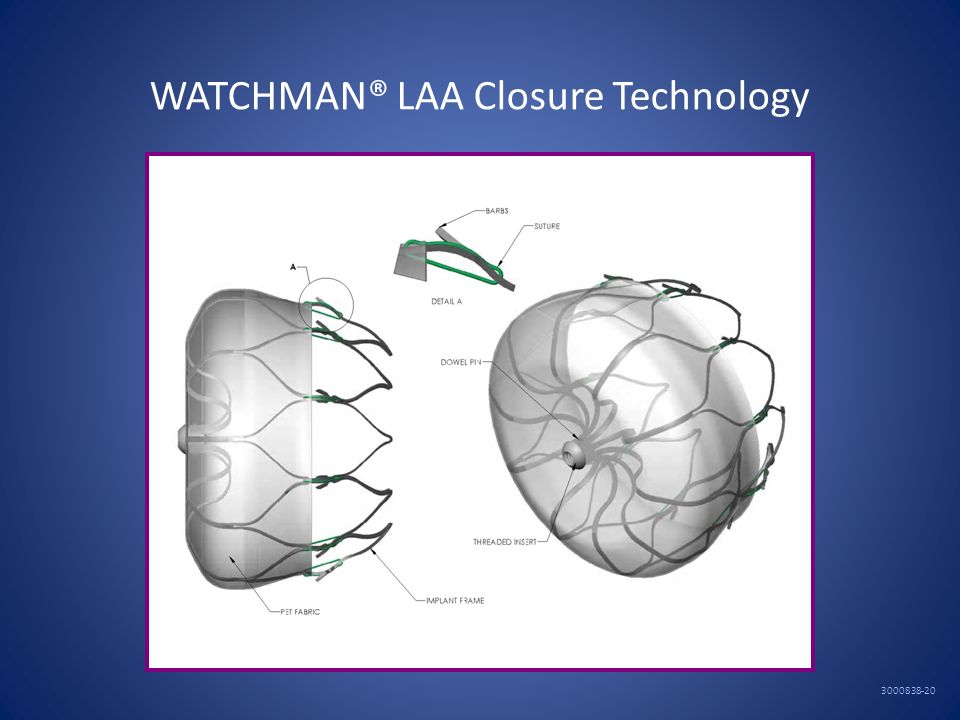
LAA: Watchman

46
WATCHMAN® LAA Closure Technology
48
LAA: Watchman PROTECT AF (RCT); 707 pts; 18 month FU
Indication: Permanent or Paroxysmal AF; CHADS >1; suitable for warfarin Noninferiority of the intervention demonstrated CE approved Reddy et al; Circulation 2011

49
PROTECT AF Clinical Trial Design
Prospective, randomized study of WATCHMAN LAA Device vs long-term warfarin therapy 2:1 allocation ratio device to control 800 patients enrolled from Feb 2005 to Jun 2008 Device group (463) Control group (244) Roll-in group (93) 59 enrolling centers (U.S. & Europe) Follow-up requirements TEE follow-up at 45 days, 6 months and 1 year Clinical follow-up biannually up to 5 years Regular INR monitoring while taking warfarin Enrollment continues in Continued Access Protocol (CAP Study)
 Control group (244) Roll-in group (93) 59 enrolling centers (U.S. & Europe) Follow-up requirements. TEE follow-up at 45 days, 6 months and 1 year. Clinical follow-up biannually up to 5 years. Regular INR monitoring while taking warfarin. Enrollment continues in Continued Access Protocol (CAP Study)")
50
Key Participation Criteria
Key inclusion criteria Age 18 years or older Documented non-valvular AF Eligible for long-term warfarin therapy, and has no other conditions that would require long-term warfarin therapy Calculated CHADS2 score 1 Key exclusion criteria NYHA class IV congestive heart failure ASD and/or atrial septal repair or closure device Planned ablation procedure within 30 days of potential WATCHMAN Device implant Symptomatic carotid disease LVEF <30% TEE criteria: suspected or known intracardiac thrombus (dense spontaneous Echo contract

51
PROTECT AF Trial Endpoints
Primary efficacy endpoint All stroke: ischemic or hemorrhagic Deficit with symptoms persisting more than 24 hours or Symptoms less than 24 hours confirmed by CT or MRI Cardiovascular and unexplained death: includes sudden death, MI, CVA, cardiac arrhythmia and heart failure Systemic embolization Primary safety endpoint Device embolization requiring retrieval Pericardial effusion requiring intervention Cranial bleeds and gastrointestinal bleeds Any bleed that requires 2uPRBC Some events will be counted as both safety and efficacy endpoints

52
Event-free probability
Intent-to-Treat Primary Safety Results Device Control Events Total Rate Events Total Rate RR Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) 600 pt-yr (8.5, 15.3) (1.9, 7.2) (1.48, 6.43) 900 pt-yr (6.4, 11.3) (2.2, 6.7) (1.18, 4.13) Randomization allocation (2 device:1 control) Device ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability Control 900 patient-year analysis Days 244 143 51 11 463 261 87 19
 pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) 600 pt-yr (8.5, 15.3) (1.9, 7.2) (1.48, 6.43) 900 pt-yr (6.4, 11.3) (2.2, 6.7) (1.18, 4.13) Randomization allocation (2 device:1 control) Device. ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability. Control. 900 patient-year analysis. Days")
53
Specific Safety Endpoint Events
Pericardial effusions – largest fraction of safety events in device group Stroke events – most serious fraction of safety events in control group Bleeding events were also frequent

54
Pericardial Effusions by Experience
Throughout PROTECT AF Trial, procedural modifications and training enhancements were implemented Procedural events would be expected to decrease over time Pericardial effusions within 7 days of the procedure are most relevant to the device performance Site implant group (includes roll-in subjects) Any procedure/ device related Any serious Any No. % No. % No. % Early patients (1-3) 13/ / / Late patients (4) 27/ / / Total 40/ / /
 Any procedure/ device related. Any serious. Any. No. % No. % No. % Early patients (1-3) 13/ / / Late patients (4) 27/ / / Total 40/ / /")
55
Effusions in Recent Implant Experience
Rates obtained in the CONTINUED ACCESS Study confirm that the lower rates are sustained Any procedure/ device related Any serious Any No. % No. % No. % 1/ / /88 1.1

56
Event-free probability
Intent-to-Treat Primary Efficacy Results Device Control Posterior probabilities Events Total Rate Events Total Rate RR Non- Superiority Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority pt-yr (2.6, 6.7) (3.0, 9.1) (0.39, 1.67) pt-yr (2.1, 5.2) (2.8, 7.6) (0.37, 1.41) Randomization allocation (2 device:1 control) WATCHMAN ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability Control 900 patient-year analysis Days 244 147 52 12 463 270 92 22
 pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority pt-yr (2.6, 6.7) (3.0, 9.1) (0.39, 1.67) pt-yr (2.1, 5.2) (2.8, 7.6) (0.37, 1.41) Randomization allocation (2 device:1 control) WATCHMAN. ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability. Control. 900 patient-year analysis. Days")
57
Event-free probability
Intent-to-Treat Hemorrhagic Stroke Device Control Posterior probabilities Events Total Rate Events Total Rate RR Non- Superiority Cohort (no.) pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority pt-yr (0.0, 0.9) (0.5, 3.9) (0.00, 0.80) > pt-yr (0.0, 0.6) (0.7, 3.7) (0.00, 0.45) Randomization allocation (2 device:1 control) Device Control ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability 900 patient-year analysis Days 244 147 53 12 463 275 95 23
 pt-yr (95% CI) (no.) pt-yr (95% CI) (95% CI) inferiority pt-yr (0.0, 0.9) (0.5, 3.9) (0.00, 0.80) > pt-yr (0.0, 0.6) (0.7, 3.7) (0.00, 0.45) Randomization allocation (2 device:1 control) Device. Control. ITT cohort: patients analyzed based on their randomly assigned group (regardless of treatment received) Event-free probability. 900 patient-year analysis. Days")
58
Risk/Benefit Analysis
Intent-to-treat analysis Primary endpoint (intent to treat) achieved Other statistically significant endpoint findings Noninferiority for the primary efficacy event rate – 32% lower in device group Noninferiority for stroke rate – 26% lower in device group Superiority for hemorrhagic stroke – 91% lower in device group Noninferiority for mortality rate – 39% lower rate in device group Increased rate of primary safety events for the device group relative to the control group Most events in the device group were procedural effusions that decreased over the course of the study 87% of patients discontinued warfarin at 45 days Death/disability conclusion
 achieved. Other statistically significant endpoint findings. Noninferiority for the primary efficacy event rate – 32% lower in device group. Noninferiority for stroke rate – 26% lower in device group. Superiority for hemorrhagic stroke – 91% lower in device group. Noninferiority for mortality rate – 39% lower rate in device group. Increased rate of primary safety events for the device group relative to the control group. Most events in the device group were procedural effusions that decreased over the course of the study. 87% of patients discontinued warfarin at 45 days. Death/disability conclusion")
59
Risk / Benefit Analysis
Per-protocol analysis Superiority for the primary efficacy event rate Approximately 86% of patients in the device group were able to be successfully implanted and discontinue warfarin therapy Study demonstrates the role of the left atrial appendage in the pathogenesis of stroke due to AF Based on average age, patients will experience a 56% reduction in safety events

60
Summary Long-term warfarin treatment of patients with AF has been found effective, but presents difficulties and risk PROTECT AF trial was a randomized, controlled, statistically valid study to evaluate the WATCHMAN device compared to warfarin In PROTECT AF, hemorrhagic stroke risk is significantly lower with the device. When hemorrhage occurred, risk of death was markedly increased In PROTECT AF, all cause stroke and all cause mortality risk are equivalent to that with warfarin In PROTECT AF, there are early safety events, specifically pericardial effusion; these events have decreased over time

61
Conclusion The WATCHMAN LAA Technology offers a safe and effective alternative to warfarin in patients with non-valvular atrial fibrillation at risk for stroke and who are eligible for warfarin therapy

62
LAA: Amplatzer Cardiac Plug
Different from Amplatzer Septal Occluder Registry; 141 pts; 24 hour FU Indication: Permanent/paroxysmal AF Early experience: Stroke 2.1%, device embolization 1.4%, tamponade 3.5% Clinical trial pending CE 12/2008 Park et al; CCI 2011

63
LAA CLOSURE: Amplatzer Cardiac Plug
CE Marked December 2008 US IDE feasibility phase enrollment is completed: 45 patients, randomized 2:1 US IDE pivotal phase to commence 2012 Evaluate safety & efficacy of ACP vs. warfarin in AF patients Prospective, randomized 2:1 (device : warfarin) Estimated 400 to 2000 patients Primary efficacy endpoint: stroke & peripheral ischemic events Acute safety endpoint Long-term safety endpoint: death and major bleeds Park et al; Cath and CV Intervention 2011
 Estimated 400 to 2000 patients. Primary efficacy endpoint: stroke & peripheral ischemic events. Acute safety endpoint. Long-term safety endpoint: death and major bleeds. Park et al; Cath and CV Intervention")
64
LAA: Other devices Coherex Wave Crest PLAATO
self expanding nitinol with coils and anchors and PTFE covering toward LA; LAA plug actively recruiting PLAATO self expanding nitinol cage with anchors and PTFE covering 2 prospective trials: 111 and 64 pts FU 10 months to 5 years TIA/CVA 2.2% - CVA 3.8% no longer available for clinical use

65
Left Atrial Appendage Closure
Multiple indications Multiple approaches CE and FDA issues Closure

Similar presentations