Download presentation
Presentation is loading. Please wait.

1
Community Systems Change Through Learning Collaboratives: Multidisciplinary Partnerships for Healthy Child Development Jill Houbé, MD, MPhil Debra Lotstein, MD, MPH Early Developmental Screening and Intervention Initiative EDSI

2
Goal and Objectives Goals Objectives
To discuss the principles and practical issues around multidisciplinary learning collaborative models to achieve health system change To review the experience of the EDSI Learning Collaborative To discuss potential applications in Canada. Objectives After participating in this activity, attendees will be able to : To describe the principles and practical applications of the learning collaborative approach to health system change and quality improvement; To identify the role of multidisciplinary partnerships for providing developmental health care services

3
Workshop Outline Introductions Background and scope
Interprofessional collaboration Collaborative system change An example of a multidisciplinary learning collaborative in paediatric healthcare: Early Development Screening Initiative (EDSI) Learning collaboratives and health system change in Canada Discussion
 Learning collaboratives and health system change in Canada. Discussion.")
4
What is interprofessional collaboration?
“Collective action toward a common goal, in a spirit of harmony and trust” D’Amour et al, (2005), Journal of Interprofessional Care, 19:2,
, Journal of Interprofessional Care, 19:2,")
5
What is interprofessional collaboration?
Five underlying concepts Sharing Partnership Interdependency Power Process Five underlying concepts Sharing: responsibilities, decision-making, planning and intervention, philosophy around care Partnership: open and honest communication, mutual respect and trust Interdependency: common desire to achieve patient outcomes Power: simultaneous empowerment of each participant Process: dynamic and interactive, transforming, interpersonal

6
What is interprofessional collaboration?
Multidisciplinary Interdisciplinary Transdisciplinary Multidisciplinary Work is independent and parallel Juxtaposition of various professionals and competencies Interdisciplinary Efforts to integrate themes shared by several professionals Common goal and decision-making process Integration of knowledge and expertise of each professional More flexibility in sharing professional responsibilities Transdisciplinary Consensus-seeking and opening up of professional territories Professional boundaries blur or vanish Deliberate exchange of knowledge, skills and expertise transcends traditional discipline boundaries

7
Determinants of successful collaboration
Systemic Organizational Interactional: microsystem Interpersonal relationships between team members Barriers include: Communication skills Personal maturity Previous experience Professional education Lack of mutual respect Organizational: mesosystem Conditions within the health care organization Traditional hierarchical structures Competitive work environment Lack of managers Lack of realistic objectives Lack of space-sharing Lack of meeting time Poor coordination and communication of standards, policies, protocols, documentation Systemic: macrosystem Social, cultural, educational and professional systems Power disparities based on gender and social status Cultural bias towards autonomy Education that socializes towards strong professional identification Professional territorial behaviour, values and basic theoretical perspectives inherent to their respective professions Interactional

8
What is Collaborative Learning?
“Learning is the social construction of knowledge” Vygotsky Individuals with differing viewpoints, experiences, and levels of knowledge interact with one another Testing, reconciling, and forging a new, shared understanding Acquiring new knowledge and restructuring existing knowledge

9
Principles of Quality Improvement
Performance is a system property Working harder in an unsupportive system will not change outcomes If you want improved performance, you have to seek a new system Improvement itself requires a system Schecter and Margolis (2005), J Pediatr;147: ; Deming WE, The New Economics for Industry, Government, Education ,Cambridge, Massachusetts, USA: The MIT Press; 2000; Berwick (1999), Managed Care Magazine
, J Pediatr;147: ; Deming WE, The New Economics for Industry, Government, Education ,Cambridge, Massachusetts, USA: The MIT Press; 2000; Berwick (1999), Managed Care Magazine.")
10
Promoting Optimal Child Development
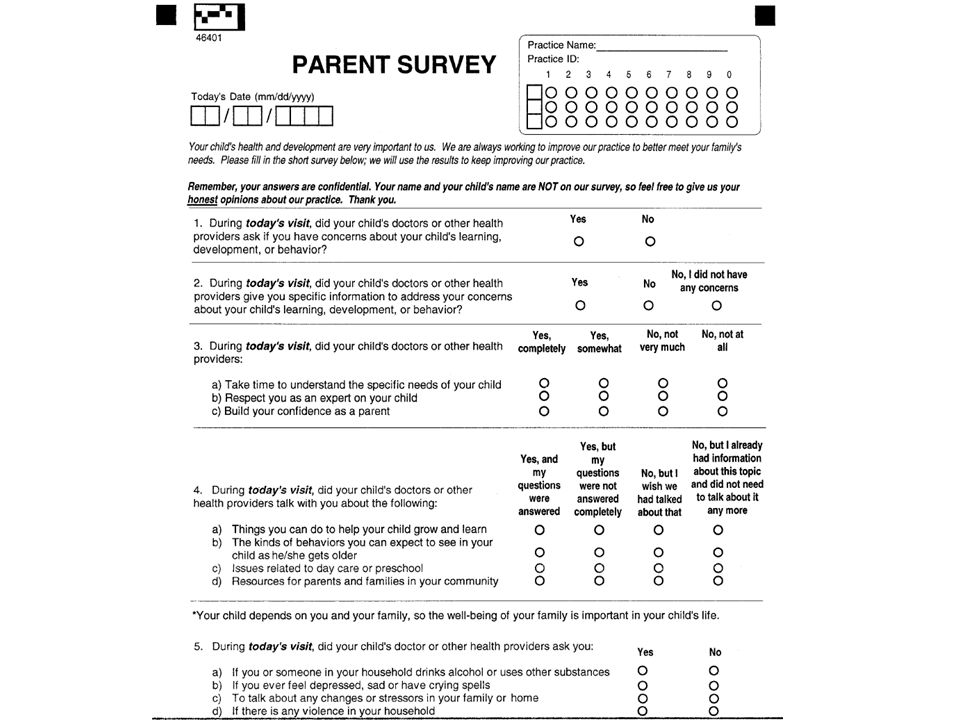
What are some challenges you are facing in: Eliciting parents’ concerns and addressing information needs? Helping parents enhance their child’s development ? Identifying children at risk for developmental and behavioral problems? Linking families with needed community services? Take 5 mins and discuss as a team; ask for comments

11
The Gaps in Care About half of parents are asked about concerns
Under-identification of developmental problems prior to school entry Lack of involvement of parents About half of parents are asked about concerns About half of these receive needed information Underserved families at high risk for poor care Poorer preventive care and elicitation of concerns Social norms about child development Limited time for ECE or PMDs to address concerns Glascoe FP, Dworkin PH. The role of parents in the detection of developmental and behavioral problems. Pediatrics 1995; 95 :829 –836; Glascoe FP, Dworkin PH. Obstacles to effective developmental surveillance: errors in clinical reasoning. J Dev Behav Pediatr 1993; 14 :344 –349; Palfrey JS, Singer JD, Walker DK, Butler JA Early identification of children's special needs: a study in five metropolitan communities. J Pediatr. 1994; 111:

12
Multidisciplinary Collaboration: The EDSI experience
Early Development Screening Initiative (EDSI) Implement reliable systems for providing effective preventive and developmental care to children less than 5 years of age. Create new systems of support through collaboration between physicians, nurses, ECE professionals, administrators, and parents. Funded by First Five, Los Angeles County Microsystem change of key players: MD/ECE practices Macrosystem change- through collaborative activities and other activiies- WIC and Policy discussion 12
 Implement reliable systems for providing effective preventive and developmental care to children less than 5 years of age. Create new systems of support through collaboration between physicians, nurses, ECE professionals, administrators, and parents. Funded by First Five, Los Angeles County. Microsystem change of key players: MD/ECE practices. Macrosystem change- through collaborative activities and other activiies- WIC and Policy discussion. 12.")
13
Providers understand and use pathways to family supports and services
EDSI Aim: To create effective systems for early identification and promotion of optimal development Parents have the knowledge, confidence and supports to promote optimal development Health care and early care and education providers discuss and address development with parents effectively Providers understand and use pathways to family supports and services Relationships between providers and community agencies promote access to resources Marlene to give 1-2 examples of how a transformed system would be different than what we currently have.

14
Recognition and Response Screening and Referral

15
Partners in the EDSI Initiative
Implementation partners Primary care practices Early care and education (ECE) Specialized programs (e.g., regional centers) Women, Infants and Children (WIC) Supplemental Food Program Steering Committee Representatives of implementation partners Opinion leaders, policy-makers, experts Affiliated programs and initiatives We can say more about who will work in these collaboratives as we walk through the system model. It is just important to point out here that we are not looking exclusively at clinicians as the responsible party for communicating with parents about developing, monitoring, discussing concerns, and connecting parents to appropriate resources. We are really looking at the potential for enhanced roles among other “first contact” early childhood professionals. Discuss P to 3 here - EDSI is a service improvement project, whereas P to 3 shares some policy and leveraging ideas but is going to fund direct services. We are hopefully that P to 3 can help change the “landscape” of available services, over time. Finally, our Steering Committee. Have brought together this particular group of advisors because for the integrity of the work, and for sustainability, we want to make sure that our work is moving in a direction that has value to those who are in policy and resource allocation positions. Ultimately these changes need to meet your needs. We really want advisory input that is not just about “what should be” but what is “ambitious but achievable” – so that we don’t end up with some neat ideas and innovations that have little chance of being leveraged or picked up, at the end of the 5 years. Let me turn to how we are thinking about your roles. We would be happy for your ideas here as well.
 Specialized programs (e.g., regional centers) Women, Infants and Children (WIC) Supplemental Food Program. Steering Committee. Representatives of implementation partners. Opinion leaders, policy-makers, experts. Affiliated programs and initiatives. We can say more about who will work in these collaboratives as we walk through the system model. It is just important to point out here that we are not looking exclusively at clinicians as the responsible party for communicating with parents about developing, monitoring, discussing concerns, and connecting parents to appropriate resources. We are really looking at the potential for enhanced roles among other first contact early childhood professionals. Discuss P to 3 here - EDSI is a service improvement project, whereas P to 3 shares some policy and leveraging ideas but is going to fund direct services. We are hopefully that P to 3 can help change the landscape of available services, over time. Finally, our Steering Committee. Have brought together this particular group of advisors because for the integrity of the work, and for sustainability, we want to make sure that our work is moving in a direction that has value to those who are in policy and resource allocation positions. Ultimately these changes need to meet your needs. We really want advisory input that is not just about what should be but what is ambitious but achievable – so that we don’t end up with some neat ideas and innovations that have little chance of being leveraged or picked up, at the end of the 5 years. Let me turn to how we are thinking about your roles. We would be happy for your ideas here as well.")
16
EDSI Project Components
QI Learning Collaboratives Population-based strategy - WIC sessions for parents Policy change and spread Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

17
EDSI Project Components
QI Learning Collaboratives Population-based strategy - WIC sessions for parents Policy change and spread Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

18
Barriers and Opportunities for Promoting Optimal Development
Parent Knowledge about development Skills at managing behavior Views about clinicians and teachers as sources of information about development/behavior Teacher/Provider Time Counseling resources and skills Early Childhood Center/Medical Practice Routine process for eliciting concerns Organized materials and resources to meet families’ needs Ability to link families with community resources These are some things we’ve heard: Parents have varying…

19
"Everyone wants change—they just don't want anything to be any different."
Yogi Berra

20
QI Learning Collaborative Format
Adapted from the Breakthrough Series Method of the Institute for Healthcare Improvement* Each participating site sends a team Three “learning sessions” over 12 months, ongoing coaching Data collection and feedback Uses the Model for Improvement Defines common set of aims, measures and ideas for change for all participants Teams come together 3 learning sessions Work together between meetings on changes, data collection and feedback *** mention this Involvement of important community agencies in LS activities Regional Center Mental Health services *

21
Model for Improvement Act Plan Study Do What are we trying to
accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? In the last session we discussed a framework of a series of strategies to address these challenges, with some more specific ideas about how to bring about those strategies. We will use the Model for Improvement to help you adapt those strategies for your own setting. We provided a short summary of the model that some of you may have seen in the prework, and we are going to go each part of it in more detail over the next 2 days. The Model for Improvement was developed over 10 years ago by a group of QI Experts called the Associates for Process Improvement. By now its been used by hundreds of organizations, many in the Breakthrough Series of QI learning collaboratives that you maybe familiar with. I’m going to preview the whole model- and discuss the first question in depth; we’ll get back to the others. Act Plan Study Do

22
Model for Improvement Act Plan Study Do What are we trying to Aim
accomplish? How will we know that a change is an improvement? What change can we make that will result in improvement? Sometimes we will refer to this as the 3 questions… The first question in the MFI: What are we trying to accomplish? The answer to this is our aim Act Plan Study Do

23
EDSI Practice Goals >75% of parents report needs met: AGPE and child’s development >75% of parents read with child daily >95% of parents have psychosocial screening >20 Office System Inventory items in place >95% of at risk children have documented follow-up plan >75% of parents report receiving family centered care >95% of children have documented developmental screening ECE and Practice goals: (reminder these are in the charter) Need to acknowledge the difference in certainty about how to measure the goals here? Focus on goals that are the most important for your practice or center Practices will get feedback on all the goals, but they could add their own goals, and they don’t have to put all the collaborative goals in their aim if they want to prioritize a few goals for their practice- where their particular gaps are.
 Need to acknowledge the difference in certainty about how to measure the goals here Focus on goals that are the most important for your practice or center. Practices will get feedback on all the goals, but they could add their own goals, and they don’t have to put all the collaborative goals in their aim if they want to prioritize a few goals for their practice- where their particular gaps are.")
24
EDSI ECE Goals >75% of young children (birth to age 5) will have documentation of an age-appropriate structured developmental screening twice yearly. > 75% of young children (birth to age 5) will have documentation of a parent-teacher conference twice yearly. > 95% of at-risk children will have a follow-up plan documented in the child’s folder. > 95% of parents with young children (birth to age 5) report their information needs about their child’s development and behavior were met. > 75% of parents report reading or sharing books daily with their child. > 95% of children will have a documented medical home provider’s name and contact information in their folder, updated within the last six months Also, subset of goals, plus one additional goal they set for self
 will have documentation of a parent-teacher conference twice yearly. > 95% of at-risk children will have a follow-up plan documented in the child’s folder. > 95% of parents with young children (birth to age 5) report their information needs about their child’s development and behavior were met. > 75% of parents report reading or sharing books daily with their child. > 95% of children will have a documented medical home provider’s name and contact information in their folder, updated within the last six months. Also, subset of goals, plus one additional goal they set for self.")
25
Team Aim The Clinica Monsenor Oscar A. Romero EDSI team is determined to improve preventive services and developmental screening and referral for children ages 0-5 years in our community. We intend to develop practice-based systems to facilitate comprehensive preventive care and developmental screening and referral. We will test and implement strategies to integrate evidence-based screening tools and anticipatory guidance into the practice workflow, with an emphasis on parent reporting. The AIM provides a rationale and point of shared vision for team’s efforts Characteristics of a strong aim. S.M.A.R.T S: SPECIFIC M: MEASURABLE A: ACTION-ORIENTED R: RELEVANT T: TIMELY Refer to your LS1 binder for the Model for Improvement Session.

26
Team Aim (continued) Our goals includes:
Greater than 75% of young children (birth to age 5) will have an age appropriate parent report based structured developmental screening at designated well-child visits. Greater than 75% of young children (birth to age 5) will have documentation of a psychosocial screening in the previous 12 months.
 will have an age appropriate parent report based structured developmental screening at designated well-child visits. Greater than 75% of young children (birth to age 5) will have documentation of a psychosocial screening in the previous 12 months.")
27
Team Aim (continued) Greater than 75% of young children (birth to age 5) identified as “at risk” will have a plan for follow up by the practice and/or referral to a community resource partner. Greater than 90% of young children will have a documented provider endorsement of and referral to The Children's Institute School Readiness Program (an organization which will facilitate referral for Early Head Start, Head Start, Preschool, and other family support services)
 identified as at risk will have a plan for follow up by the practice and/or referral to a community resource partner. Greater than 90% of young children will have a documented provider endorsement of and referral to The Children s Institute School Readiness Program (an organization which will facilitate referral for Early Head Start, Head Start, Preschool, and other family support services)")
28
Wilton Place ECC Team Aim
Implement reliable systems for effective preventive and developmental care and support for children 2 – 5. We will achieve our aim by: Enhancing positive discussions with families Building relationships with community resources Building a continuous learning system for our center Goals & Measures 75% of children will have documentation of an age - appropriate structured developmental screening 75% of teachers will have information from screening 95% of children will have contact information in their folder, updated within the last six months

29
Model for Improvement Act Plan Study Do What are we trying to
accomplish? How will we know that a Measures change is an improvement? What change can we make that will result in improvement? The second question How will we know that a change is an improvement- is answered by the data we collect from the processes we’re working on. We will talk about measurement in much more detail tomorrow. Information from measurement, or data, guides the actions we take. Act Plan Study Do

31
Example Data Feedback Reports

32
Model for Improvement Act Plan Study Do What are we trying to
accomplish? How will we know that a change is an improvement? What change can we make that Ideas/Changes will result in improvement? The 3rd question, what change can we make that will result in improvement? is answered by the ideas that we just discussed. Another way of saying this is that the 3 questions help us stay focused on our goal --& it is REALLY easy to get distracted The first question is about our aim, the second is about learning, and the third is what we will do to accomplish our aim. Another way to think about this: The aim is where we are going. The measures are how we will know we are making progress. If I’m headed to Vermont, I know I’ll be part way there when my plane lands in Philadelphia. Act Plan Study Do

33
Multiple Sources of Ideas for Change
Tools from Healthy Development collaborative* Literature review Interviews/site visits with local high-performing early childhood centers Teams develop new ideas and share with each other Examples: Preventive services prompting sheet; using PEDS and tools for that * A Practical Guide for Healthy Development

34
New Ideas are Tested and Implemented Using PDSA Cycles
Act Plan Study Do This is sometimes called the shewhart cycle, or plan do check act, The Plan do study act, or PDSA cycle is used to test and implement the changes we make to see if they lead to improvement. We first Plan the details of the test and predicting what we think will happen We then conduct the test and collect data Study: compare our predictions to the results of the test Finally, we close the circle by taking action based on our new knowledge Again, we will have more time hearing about and practicing using the cycles tomorrow.

35
Use PDSA Cycles to Test and Implement Changes
Plan the details of the test and predict the outcome of the test Act Plan Study Do This is sometimes called the shewhart cycle, or plan do check act, The Plan do study act, or PDSA cycle is used to test and implement the changes we make to see if they lead to improvement. We first Plan the details of the test and predicting what we think will happen We then conduct the test and collect data Study: compare our predictions to the results of the test Finally, we close the circle by taking action based on our new knowledge Again, we will have more time hearing about and practicing using the cycles tomorrow.

36
Use PDSA Cycles to Test and Implement Changes
Plan the details of the test and predict the outcome of the test Act Plan Study Do This is sometimes called the shewhart cycle, or plan do check act, The Plan do study act, or PDSA cycle is used to test and implement the changes we make to see if they lead to improvement. We first Plan the details of the test and predicting what we think will happen We then conduct the test and collect data Study: compare our predictions to the results of the test Finally, we close the circle by taking action based on our new knowledge Again, we will have more time hearing about and practicing using the cycles tomorrow. Do: Conduct the test and collect data

37
Use PDSA Cycles to Test and Implement Changes
Plan the details of the test and predict the outcome of the test Act Plan Study Do This is sometimes called the shewhart cycle, or plan do check act, The Plan do study act, or PDSA cycle is used to test and implement the changes we make to see if they lead to improvement. We first Plan the details of the test and predicting what we think will happen We then conduct the test and collect data Study: compare our predictions to the results of the test Finally, we close the circle by taking action based on our new knowledge Again, we will have more time hearing about and practicing using the cycles tomorrow. Study: Compare predictions to the test results Do: Conduct the test and collect data

38
Use PDSA Cycles to Test and Implement Changes
Plan the details of the test and predict the outcome of the test Act: Take action based on the new knowledge Act Plan Study Do This is sometimes called the shewhart cycle, or plan do check act, The Plan do study act, or PDSA cycle is used to test and implement the changes we make to see if they lead to improvement. We first Plan the details of the test and predicting what we think will happen We then conduct the test and collect data Study: compare our predictions to the results of the test Finally, we close the circle by taking action based on our new knowledge Again, we will have more time hearing about and practicing using the cycles tomorrow. Study: Compare predictions to the test results Do: Conduct the test and collect data

39
The Model Provides Structure for Repeated Tests
This model for improvement picture with one big PDSA is a bit deceiving- your work during the collaborative is NOT one big PDSA cycle; Instead the model provides a framework for repeated, small, rapid cycle testing of ideas; These cycles really are small- You could do a PDSA cycle in an hour (maybe give an example)- let say trying out a brand new form you created for community referrals with one child, one time- you could set that up to be a PDSA cycle, and it would be pretty quick. this testing allows you to move from having some Hunches, theories and good ideas about what will improve your child developmental services all that way to changes that you feel confident will result in improvement and are ready to make a routine part of your center or practice. Planning and carrying out these PDSA cycles will be the focus of our Accelerating improvement talk tomorrow The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. IHI Innovation Series white paper. Boston: Institute for Healthcare Improvement; 2003 39
- let say trying out a brand new form you created for community referrals with one child, one time- you could set that up to be a PDSA cycle, and it would be pretty quick. this testing allows you to move from having some Hunches, theories and good ideas about what will improve your child developmental services all that way to changes that you feel confident will result in improvement and are ready to make a routine part of your center or practice. Planning and carrying out these PDSA cycles will be the focus of our Accelerating improvement talk tomorrow. The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement. IHI Innovation Series white paper. Boston: Institute for Healthcare Improvement;")
40
Example: ECE First Plan-Do-Study-Act Cycle
Questions: Will a structured written form better assist for discussing developmental and behavioral observations of a child? Will this form also be proactive to assist during parent – teacher conferences by answering their questions and concerns? Predictions: Having a form to structure the discussion at the conferences will make it easier for teacher to focus the discussion and assure that important things are not left out. The form will make the conference more helpful in answering parents questions and concerns. DO: Conference took minutes. Family has 4 year old boy, bilingual, developing on track, without any behavioral or developmental concerns. Gave copy of form to parents and put copy in child’s folder. STUDY: Parent ask about Spanish translation of the parent survey. Need to re – word questions because they were not clear to parent. Parent likes being involved and was very open. ACT: Team will revise the form; the teacher will test it out more conferences over the next 2 weeks and report back to the team the following week.

41
Physicians’ Office PDSA Developing Office Systems
Question: Is it helpful to use a case manager to endorse the provider’s referral to an early education program? Are our parents able to access early education programs through the Children’s Institute? Plan for Test: Dr. Prestwich and Dr. Willard will ask the 3 different parents 0-5year old children if the child is enrolled in an early education program. If not, they will refer the parent to The Children’s Institute. Dr. Prestwich and Dr. Willard will have the same discussion with 3 other parents, but they will then refer them on to Alba or Yvonne for reinforcement of the referral. Do/Study: 6 parents were referred and all of them expressed intent to keep an appointment. After 3 weeks we found that 1 (mother of 15 month old, referral by MD without Case Manager assist) kept appointment. She was frustrated that Early Head Start has a waiting list. The other 5 had not yet called, but indicated they plan to. Act: We confirmed that there are long wait lists for kids 0-2 years, but immediate access to early education programs for 3-5 year olds in our area. May need case manager to assure follow-up after the visit. Will continue to follow the 5 parents; test with 5 more.
 kept appointment. She was frustrated that Early Head Start has a waiting list. The other 5 had not yet called, but indicated they plan to. Act: We confirmed that there are long wait lists for kids 0-2 years, but immediate access to early education programs for 3-5 year olds in our area. May need case manager to assure follow-up after the visit. Will continue to follow the 5 parents; test with 5 more.")
42
Multiple PDSA Cycle Ramps
Testing and Adaptation Develop office systems Work as a team Use structured screening tools Discuss parent concerns Partnerships with community resources Continuous learning system Develop office systems Use structured screening tools Develop partnerships with community resounces Care in planned encounters Build continuous learning system Work as team Discuss observations and pt concerns Build communications with medical homes Develop relationships with community resources

43
Lessons Learned (so far…)
Challenges Teams used to top-down approach to change Working effectively as a team Data collection is something “extra” (not able to get from existing processes) Strengths Sharing and learning across disciplines Professional development for staff Staff validation and engagement in the “big picture”
 Strengths. Sharing and learning across disciplines. Professional development for staff. Staff validation and engagement in the big picture")
44
EDSI Project Components
QI Learning Collaboratives Population-based strategy - WIC sessions for parents Policy change and spread Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

45
WIC Sessions for Parents
Women Infants and Children program pre-natal to years old nutritional and educational services provided by trained peers Curriculum developed to teach parents’ skills for talking with clinicians Themes: Parents are the best observers of their child’s development; expectations for their child’s doctor Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

46
EDSI Project Components
QI Learning Collaboratives Population-based strategy - WIC sessions for parents Policy change and spread Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

47
Policy Change and Spread
Clarify specific policy issues for an improved system E.g. shared vision, respective roles, expectations and guidelines, workforce and training, reimbursement Convene several policy summits including County and State policymakers Slide 9 – put the practice work in bigger context – want ECEs to help clinician efforts, also want to make parents more prepared so it makes the hard job that clinicians have easier.

48
“What the best and wisest parent wants for her own child, that must be what the community wants for all its children.” John Dewey

49
Planning for Change in Your System using a Learning Collaborative Approach
What is your general aim for improvement? Who should be involved? What are some incentives for encouraging their participation? Who might help support such an effort? What are some potential facilitators of collaboration (e.g. data sources, aligned incentives, etc) What are some potential barriers to collaboration?
 What are some potential barriers to collaboration")
50
Potential barriers Potential promoters Potential benefits
Multidisciplinary learning collaboratives: A Model for Quality Improvement in Canada? Potential barriers Boundaries between subspecialty and primary care systems Limited communication between systems of care Limited data collection and sharing between systems of care Potential promoters Publicly funded health insurance Population-level data collection Potential benefits Improvement in healthy child development outcomes Improvement in adult health and well-being

51
Percentage of Students Vulnerable Emotional Maturity scale of the EDI (Based on Provincial cutoffs), Wave 1
, Wave 1")
52
Acknowledgements Sunny Hill Foundation
British Columbia Child and Family Research Institute Hillel Goelman and Clyde Hertzman Consortium for Health, Intervention, Learning and Development Human Early Learning Partnership BC Healthy Child Development Alliance Neonatal Follow-Up Program Dana Brynelsen and Infant Development Program Contact:

53
EDSI Team UCLA Center for Healthier Children, Families, and Communities Center for Health Care Quality, Cincinnati Children's Hospital Medical Center RAND Corporation Public Health Foundation Enterprises (PHFE) WIC LA BioMed WIC California State University, Los Angeles Childrens Hospital Los Angeles Cedars-Sinai Medical Center Marlene to give 1-2 examples of how a transformed system would be different than what we currently have.
 WIC. LA BioMed WIC. California State University, Los Angeles. Childrens Hospital Los Angeles. Cedars-Sinai Medical Center. Marlene to give 1-2 examples of how a transformed system would be different than what we currently have.")
Similar presentations