Download presentation
Presentation is loading. Please wait.

1
UPDATES IN ... PEDIATRIC UROLOGY
Dr. Alex Breugelmans, M.D. Head of Department Dept. of Urology, Reg. Hosp. Heilig Hart, Leuven, Belgium

3
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

4
UWI = bacteriuria met symptomen van infectie
5 percent van alle meisjes 1 tot 2 percent van alle jongens 0.1 tot 1.0 percent van alle pasgeborenen (10 percent in low-birth-weights) (hematogenous) < 1 J : jongens > meisjes > 1 J : meisjes > jongens preschool: prevalentie van asymptomatische infecties (diagnose: suprapubiche aspiratie) bij meisjes is 0.8 percent, vergeleken met 0.2 percent bij jongens school-groep: incidentie van bacteriuria bij meisjes is 30 maal deze bij joingens (1.2 versus 0.04 percent)
 (hematogenous) < 1 J : jongens > meisjes. > 1 J : meisjes > jongens. preschool: prevalentie van asymptomatische infecties (diagnose: suprapubiche aspiratie) bij meisjes is 0.8 percent, vergeleken met 0.2 percent bij jongens. school-groep: incidentie van bacteriuria bij meisjes is 30 maal deze bij joingens (1.2 versus 0.04 percent)")
5
UWI : Etiologie en Pathogenese
Escherichia coli : 80 percent Staphylococcus Streptococcus enterobacteria (e.g., Klebsiella, Proteus) occasioneel Candida albicans. AS ALWAYS: virulentie van de bacterie en de vatbaarheid van de gastheer zijn van primordiaal belang in de ontwikkeling van UWI
 occasioneel Candida albicans. AS ALWAYS: virulentie van de bacterie en de vatbaarheid van de gastheer zijn van primordiaal belang in de ontwikkeling van UWI.")
6
UWI : oorzaken Elke conditie die leidt tot urinairer stase
renale calculi obstructieve uropathie Plasproblemen/stoornissen vesicoureterale reflux (ook indien steriel ?)
")
7
UWI : complicaties nierparenchym infectie en littekenvorming
(10-15 %, zeker zo < 1 J, zelden > 5 J) hypertensie (23 %) nierinsufficientie (10 %) Steriele reflux ?
 hypertensie (23 %) nierinsufficientie (10 %) Steriele reflux")
8
Relatie tussen UWI en verlies van nierfunctie.

9
UWI : Klinische Presentatie
VARIABEL ………….. "asymptomatische" bacteriuria: enuresis, “squatting”, … Algemeen zieke neonatus (lethargisch, hypotensief) Hoewel kinderen vaak worden behandeld op basis van klinische symptomen alleen, zijn deze onbetrouwbare predictoren voor het al dan niet risico op pyelonephritis en littekenvorming in de nier
 Hoewel kinderen vaak worden behandeld op basis van klinische symptomen alleen, zijn deze onbetrouwbare predictoren voor het al dan niet risico op pyelonephritis en littekenvorming in de nier.")
10
UWI : Anamnese Zuigeling Peuter - Kleuter : koorts slecht drinken
ongelukkig zijn slecht groeien NIETS Peuter - Kleuter : koorts buikpijn pollakisurie dysurie

11
UWI : Klinisch onderzoek
hypertensie abdominale of flank massa palpabele blaas neurologisch deficit abnormale genitalia abnormale urinaire flow Aanwezigheid van irritatieve urinaire symptomen in afwezigheid van bacteriën suggereert een non-UWI oorzaak zoals vaginitis, urethritis, enterobius-worm, bubbel-baden.

12
UWI : Symptomen Urineweg symptomen Dysuria Frequentie Druppelen/hesitatie Enuresis optredend na succesvolle toilet-training Slechtriekende urine Hematuria “Squatting” Abdominale/suprapubische pijn Systemische tekenen en symptomen Koorts Braken / Diarree Flank/rug pijn

13
UWI : Klinisch Onderzoek
Zuigeling “acuut” abdomen sepsisbeeld meningeaal beeld Failure to thrive NIETS

14
UWI : Klinisch Onderzoek
Groter kind koorts abdominale pijn (sub)acuut abdomen afwezigheid van andere koortsoorzaak
acuut abdomen. afwezigheid van andere koortsoorzaak.")
15
UWI : Diagnose Hoge graad van suspectie bij kinderen met koorts > 48 uren guidelines van de “American Academy of Pediatrics (AAP)”: evaluation of fever (39.0°C [102.2°F] or higher) of unknown origin => urinalysis in all cases (pyuria usually present) urine culture in all boys younger than six months urine culture in all girls younger than two years In recurrent episodes, episodes that fail therapy or in girls with pyuria without bacteriuria, a culture is recommended.
 of unknown origin => urinalysis in all cases (pyuria usually present) urine culture in all boys younger than six months. urine culture in all girls younger than two years. In recurrent episodes, episodes that fail therapy or in girls with pyuria without bacteriuria, a culture is recommended.")
16
UWI : Diagnose Goed afgenomen urine-cultuur is essentiëel
Kleine kinderen : suprapubische aspiratie / blaascatheterizatie Grotere kinderen: “clean-voided midstream” specimen adhesieve perineale zakjes / luiervocht: suboptimaal (fecale contamination of urethrale colonizatie) > 5 witte bloedcellen per high-power veld in gecentrifugeerde verse urine = positieve screening test
 > 5 witte bloedcellen per high-power veld in gecentrifugeerde verse urine = positieve screening test.")
17
UWI : Urine opvangen Zuigeling Peuter Kleuter huid ontvetten
huid ontsmetten steriel urinezakje regelmatig nakijken staal snel naar het labo Peuter huid ontsmetten steriel potje staal snel naar het labo Kleuter midstream urine

18
UWI :Urine-Onderzoek URINE STICK ph glucose eiwit bloed nitriet
leucocyten DIP-SLIDE URINE MICROSKOPIE Morfologie Gramkleuring Telling Sediment URINECULTUUR

19
UWI : Aanvullend Onderzoek
Meisje jonge zuigeling sepsisbeeld pyelonefritis peuter, kleuter cystitis recidief Jongen altijd

20
UWI : Medische beeldvorming
Echografie - heeft IVU grotendeels vervangen - echo alleen is vaak niet voldoende (niet betrouwbaar in opsporen van vesicoureterale reflux, nierlittekens of inflammatoire veranderingen) - indien reflux of morphologische abnormaliteiten gevonden worden, zijn nierscintigrafie en mictie- cystourethrografie aangewezen
 - indien reflux of morphologische abnormaliteiten gevonden worden, zijn nierscintigrafie en mictie- cystourethrografie aangewezen.")
21
UWI : Medische beeldvorming
Intraveneuze Urografie - anatomisch beeld: cysten, hydronefrose - minder gevoelig dan nierscintigrafie in de detectie van pyelonephritis en “renal scarring” - hogere dosis radiatie en risico van reactie op contrast- medium => Nierscintigrafie heeft IVU vervangen als standaardtechniek in de diagnose van nierinflammatie en “renal scarring”

22
UWI : Medische beeldvorming
Nierscintigrafie Technetium-99mlabeled glucoheptonaat of dimercaptosuccinic acid (DMSA) hoge graad van sensitiviteit en specificiteit DMSA scanning heeft het voordeel van zowel vroegtijdige detectie van acute inflammatoire veranderingen en permanente littekenvorming in vergelijking tot echo en IVU ook bruikbaar bij neonati en patiënten met slechte nierfunctie
 hoge graad van sensitiviteit en specificiteit. DMSA scanning heeft het voordeel van zowel vroegtijdige detectie van acute inflammatoire veranderingen en permanente littekenvorming in vergelijking tot echo en IVU. ook bruikbaar bij neonati en patiënten met slechte nierfunctie.")
23
UWI : Medische beeldvorming
Computed tomography (CT) - sensitief en specifiek voor detectie van acute pyelonephritis (geen vergelijkende studie tussen CT en DMSA) - CT is duurder dan scintigrafie en zorgt toch voor hogere stralendosis
 - sensitief en specifiek voor detectie van acute pyelonephritis (geen vergelijkende studie tussen CT en DMSA) - CT is duurder dan scintigrafie en zorgt toch voor hogere stralendosis.")
24
UWI : Medische beeldvorming
Mictie-Cystourethrografie - vesicoureterale reflux is een risicofactor voor reflux- nephropathie en littekens: vroege D/ noodzakelijk ! - uitvoeren NA R/ van UWI (vesicoureterale reflux kan het tijdelijke gevolg zijn van UWI) - door lage sensitiviteit en specificiteit, en wegens irradiatie-effect op de gonaden en NW van catheterizatie: strikte indicatie noodzakelijk
 - door lage sensitiviteit en specificiteit, en wegens irradiatie-effect op de gonaden en NW van catheterizatie: strikte indicatie noodzakelijk.")
25
UWI : Medische beeldvorming
Isotopen Cystogram (met DTPA !) Ionizatie-radiatie dosis is slechts 1 percent van deze bij mictiecystourethrografie Continue monitoring is ook meer sensitief voor het opsporen van reflux dan de intermittente flouroscopische monitoring bij mictiecystourethrografie
 Ionizatie-radiatie dosis is slechts 1 percent van deze bij mictiecystourethrografie. Continue monitoring is ook meer sensitief voor het opsporen van reflux dan de intermittente flouroscopische monitoring bij mictiecystourethrografie.")
26
Vergelijking van de Beeldvormende technieken

27
Belang van de huisarts in vroege herkenning van UWI (en dus voorkomen van nierinfectie en sequellen) is hierdoor nogmaals onderstreept.
 is hierdoor nogmaals onderstreept.")
28
UWI: Behandeling Toxische pt: IV antibiotica=> opvolgen symptomen (verdwijnen na 3-5d) (dan ontslag en nog d AB per os) Initiële antibiotica therapie zou moeten afgestemd zijn op leeftijd, klinische ernst, locatie van de infectie, aanwezigheid van structurele afwijkingen en allergische voorgeschiedenis tov. evt. AB Starten met breed-spectrum antibioticum => cultuur afwachten en zo nodig aanpassen Hospitalizatie: symptomatische babies (< 3 maanden) en alle kinderen met klinische evidentie van acute ernstige pyelonephritis (hoge koorts, toxisch uitzicht, flankpijn). Duur van outpatient treatment : controversiëel (3-7d, 7-10d)
 en alle kinderen met klinische evidentie van acute ernstige pyelonephritis (hoge koorts, toxisch uitzicht, flankpijn). Duur van outpatient treatment : controversiëel (3-7d, 7-10d)")
29
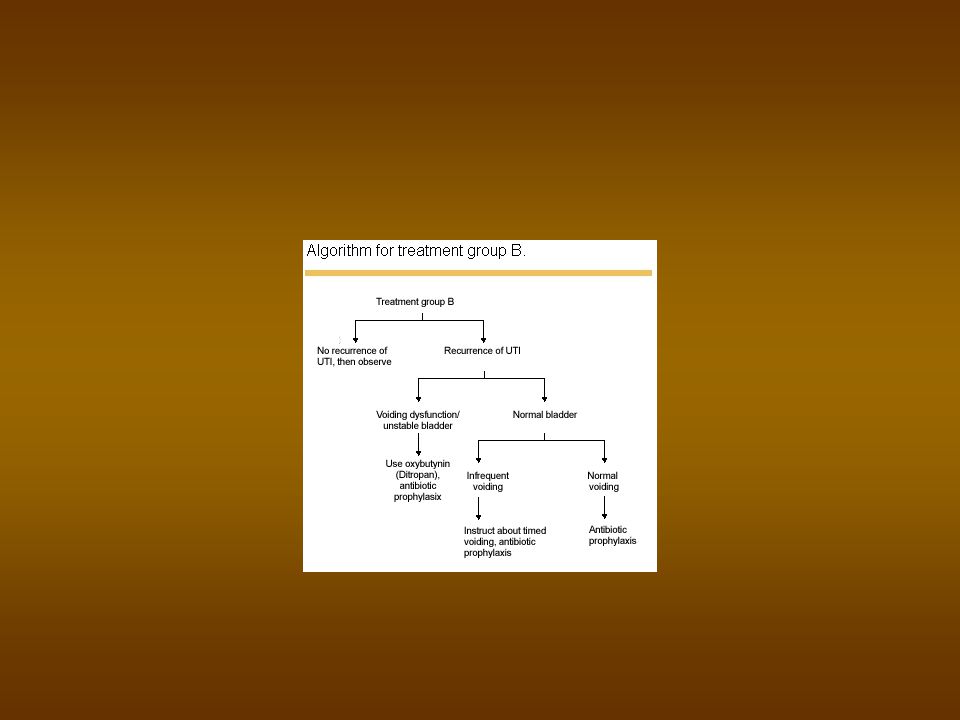
Algoritme voor R/ UWI bij kinderen

32
UWI : Praktische Aanpak van de Banale Infectie
Cefaclor (Ceclor) 30 mg/kg/dag in 2x gedurende 10 dagen Cefadroxyl (Duracef) 30mg/kg/dag in 2x gedurende 10 dagen Trimetoprim-Sulfa (Bactrim, Eusaprim, Co-Trimoxazole) 8 mg T/kg/dag in 2x gedurende 10 dagen
 30 mg/kg/dag in 2x gedurende 10 dagen. Cefadroxyl (Duracef) 30mg/kg/dag in 2x gedurende 10 dagen. Trimetoprim-Sulfa. (Bactrim, Eusaprim, Co-Trimoxazole) 8 mg T/kg/dag in 2x gedurende 10 dagen.")
33
UWI : Praxis acute ernstige infectie
opname Kinderafdeling correctie shock e.d. Antibiotica I.V. Amoxy-Clavulaanzuur (Augmentin) 100 mg/kg/dag in 2x (1g per ampul) Cefotaxim (Claforan) 50 à 100 mg/kg/d in 2 tot 4 doses (1g per ampul)
 100 mg/kg/dag in 2x (1g per ampul) Cefotaxim (Claforan) 50 à 100 mg/kg/d in 2 tot 4 doses (1g per ampul)")
34
UWI : Praxis recidieven
zoals voorgaande Amoxy-Clavulaanzuur (Augmentin, Clavucid) 30-50 mg/kg/dag in 3x gedurende 14 dagen Nitrofurantoïne (Furadantine) 6 mg (1ml) /kg/dag in 2x ged.14 dagen
 mg/kg/dag in 3x gedurende 14 dagen. Nitrofurantoïne (Furadantine) 6 mg (1ml) /kg/dag in 2x ged.14 dagen.")
35
UWI : Praxis preventie preventie na infectie voor bv cystografie
verlengen normale kuur eenmalige dosis verder preventie bij afwijking voor lange tijd Cefaclor in 1 of 2 doses 10 mg/kg/dag Co-Trimoxazole in 1x 2 mg/kg/dag Nitrofurantoïne in 1 x 1 mg/kg/dag

36
UWI : Special Issues Asymptomatic Bacteriuria AB-R/ ???
If recurrent bacteriuria is truly asymptomatic, no antimicrobial treatment may be the best option, as some studies have shown that asymptomatic children are at very low risk of renal scarring, and prophylactic treatment did not decrease the risk of UTI recurrence

37
UWI : Special Issues Recurrent UTI
two or more UTIs over a six-month period can be caused by inadequate treatment of an unrecognized anatomic site of bacterial persistence (small infected calculus or unrecognized anatomic abnormality) UTI increases the risk of subsequent renal scarring.
 UTI increases the risk of subsequent renal scarring.")
38
UWI : Special Issues Breakthrough UTI
- change in the resistance pattern of organisms colonizing the urethra => the treating antimicrobial agent for a breakthrough UTI should, ideally, be different from the prophylactic agent - noncompliance - vesicoureteral reflux - voiding dysfunction

39
=> “Voiding Dysfunction”
detrusor instability and incomplete bladder emptying (UDT) often w/ daytime enuresis and constipation increased risk for the development of vesicoureteral reflux and UTI treatment of voiding dysfunction includes timed voiding, treatment of constipation, prophylactic antibiotics and, in some cases, use of anticholinergic medication (e.g., oxybutynin [Ditropan] or propantheline [Pro-Banthine]) or biofeedback patients with otherwise unexplained recurrent UTI, especially in the setting of daytime enuresis or constipation, may merit urodynamic testing (UDT)
 often w/ daytime enuresis and constipation. increased risk for the development of vesicoureteral reflux and UTI. treatment of voiding dysfunction includes timed voiding, treatment of constipation, prophylactic antibiotics and, in some cases, use of anticholinergic medication (e.g., oxybutynin [Ditropan] or propantheline [Pro-Banthine]) or biofeedback. patients with otherwise unexplained recurrent UTI, especially in the setting of daytime enuresis or constipation, may merit urodynamic testing (UDT)")
40
UWI : Chemoprophylaxis
A urine culture should be obtained seven days after the completion of treatment to exclude relapse. Prophylaxis is recommended for all children younger than five years of age with vesicoureteral reflux (who are not surgical candidates) or other structural abnormalities and in children who have had three documented UTIs in one year With careful monitoring for side effects, a prophylactic trial of a single nightly dose of nitrofurantoin 1 to 2 mg per kg per day, or trimethoprim-sulfamethoxazole 2 mg per kg of trimethoprim per day, may be used for six months or more. Using low doses of antibiotics for prophylaxis has a theoretic advantage since this may minimize serum levels and subsequent enteric bacterial resistance while urinary concentration of the antibiotic remains high enough to maintain sterile urine.
 or other structural abnormalities. and in children who have had three documented UTIs in one year. With careful monitoring for side effects, a prophylactic trial of a single nightly dose of nitrofurantoin 1 to 2 mg per kg per day, or trimethoprim-sulfamethoxazole 2 mg per kg of trimethoprim per day, may be used for six months or more. Using low doses of antibiotics for prophylaxis has a theoretic advantage since this may minimize serum levels and subsequent enteric bacterial resistance while urinary concentration of the antibiotic remains high enough to maintain sterile urine.")
41
UWI : Preventie good hygiene (including "front-to-back" wiping after urination in girls)$ avoidance or correction of constipation avoidance of bubble baths, chemical irritants and tight clothing The role of circumcision in preventing UTI is controversial.

42
UWI : guidelines pt 1 most common bacterial infections encountered by primary care physicians source of significant morbidity in children minority of UTIs progress to renal scarring, hypertension and renal insufficiency Clinical presentation of UTI in children may be nonspecific, and the appropriateness of certain diagnostic tests remains controversial

43
UWI : guidelines pt. 2 diagnostic work-up : uncover functional and structural abnormalities such as dysfunctional voiding, vesicoureteral reflux and obstructive uropathy more aggressive work-up, including renal cortical scintigraphy, ultrasound and voiding cystourethrography, is recommended for patients at greater risk for pyelonephritis and renal scarring, including infants less than one year of age and all children who have systemic signs of infection concomitant with a UTI Antibiotic prophylaxis is used in patients with reflux or recurrent UTI who are at greater risk for subsequent infections and complications.

45
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

46
ABDOMINALE MASSA NIERGEZWEL CYSTISCH VAST
DILATATIE OBSTRUCTIEF (PUJ - VUJ) REFLUX NO-NR MEGACALYCOSIS / URETER
 REFLUX. NO-NR MEGACALYCOSIS / URETER.")
47
POSTNATALE EVALUATIE echo D1 of 2 : dilatatie = pyelum >15 mm
= > cave : fysiologische dilatatie dehydratatie lage diurese (GFR) asymptomatisch en geen kleppen (cystogram ??) : 2 m AB => DMSA
 asymptomatisch en geen kleppen (cystogram ) : 2 m AB => DMSA.")
48
controle echo (D5 en D21): + cystogram (laattijdige opname) isotopen (MAG3) + furosemide blaassonde : PUJ, VUJ, lager ?

49
Multicystische nieren
"druiventrosnieren" (ureteratresie) extreem = Potter K.O. : abdominale massa echo : cysten D f , geen parenchym R/ indien pijn (geen Ca-risico)
 extreem = Potter. K.O. : abdominale massa. echo : cysten D f , geen parenchym. R/ indien pijn (geen Ca-risico)")
50
Polycystische nieren autosomaal recessief zeldzaam
K.O. : abdominalemassa echo : vergrote echogene nieren bilateraal nierfalen

51
Niertumoren tumor : neuroblastoma mesoblastisch nefroma
Wilms: zeldzaam, 3j, multiloc. cystenier vena renalis trombose : + hematurie

52
Antenatal Hydronephrosis (AHN)
outflow of urine from the kidney is obstructed detected by ultrasound (first trimester) mild, moderate, or severe
 mild, moderate, or severe.")
53
AHN : Causes UPJ stenosis (developing before second trimester)
UVJ stenosis Posterior urethral valves Reflux Duplication anomaly (occurs in 1% of the population and involves two ureters leading from the kidney; one may have an obstruction called a uterocele) Multicystic kidney (nonfunctional kidney)
 Multicystic kidney (nonfunctional kidney)")
54
OBSTRUCTIEVE MEGAURETER
fetale hydrouretronefrose, UWI, buikpijn, hematurie isotopen (MAG3) + furosemide + BS (Whitaker) R/ heelkunde indien symptomatisch (+ "tailoring") quid fetale HUN (follow-up +/- AB)
 + furosemide + BS (Whitaker) R/ heelkunde indien symptomatisch (+ tailoring ) quid fetale HUN (follow-up +/- AB)")
55
UPJ obstruction: blockage at the left ureteropelvic junction

56
Vesicoureteral reflux on the left

57
Posterior urethral valves: blockage at the outlet of the bladder

58
Multicystic kidney

59
Duplication of ureters on both sides with ureterocele on left causing blockage

60
AHN : Diagnosis prenatal ultrasound
during evaluation for a urinary tract infection in infancy

61
AHN : Treatment carefully observing kidney growth and function throughout the pregnancy by ultrasound multicystic kidney: removal of the nonfunctioning kidney is not required unless complications (e.g., tumor, excessive size) moderate or severe antenatal hydronephrosis: pyeloplasty (success rate of 90–95%) However, in many cases (even moderate to severe cases), the condition resolves and does not result in kidney damage. Carefully monitoring kidney growth and function is the preferred treatment unless surgery proves necessary.
 moderate or severe antenatal hydronephrosis: pyeloplasty (success rate of 90–95%) However, in many cases (even moderate to severe cases), the condition resolves and does not result in kidney damage. Carefully monitoring kidney growth and function is the preferred treatment unless surgery proves necessary.")
62
AHN : Follow-up kidney function must be regularly monitored (usually by ultrasound performed every 6 months) throughout childhood low-dose antibiotics may be administered to prevent infection cystogram may be performed to determine reflux

64
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

65
MEGAURETER obstructief (cfr. Supra)
. alleen circulaire spier . jongens, links % bilateraal refluerend niet-obstructief niet-refluerend

66
UPJ Obstruction : Overview
severe, minimal can be intermittent often diagnosed during prenatal ultrasound It is the most common cause of hydronephrosis in utero and in newborns.

67
UPJ Obstruction : Incidence
1% of prenatal ultrasounds detects AHN UPJ obstruction in 50% of these more common in males (5:2) affects the left kidney more often than the right (5:2) about 15–30% of cases occur in both kidneys
 affects the left kidney more often than the right (5:2) about 15–30% of cases occur in both kidneys.")
68
UPJ Obstruction : Causes
Congenital abnormalities - abnormality in the muscles that surround the UPJ (APERISTALSIS) - abnormality in the structure or position of the ureter, kidney, and renal blood vessels in older children - compression of the ureter caused by inflammation - VUR with kinking of the ureter (10 %) - retroperitoneal fibrosis - kidney stones - scar tissue from previous surgery to correct UPJ-O
 - abnormality in the structure or position of the ureter, kidney, and renal blood vessels. in older children. - compression of the ureter caused by inflammation. - VUR with kinking of the ureter (10 %) - retroperitoneal fibrosis. - kidney stones. - scar tissue from previous surgery to correct UPJ-O.")
69
UPJ Obstruction : Signs
Back pain Blood in the urine (hematuria) Failure to thrive Flank pain Flank mass Kidney infection (pyelonephritis) Urinary tract infection (UTI) (usually in adults only !!)
 Failure to thrive. Flank pain. Flank mass. Kidney infection (pyelonephritis) Urinary tract infection (UTI) (usually in adults only !!)")
70
UPJ Obstruction : Diagnosis
If hydronephrosis : prenatal ultrasound Neonatal patients suspected to have this condition are evaluated for the obstruction using renal ultrasound. Other diagnostic tests used to evaluate kidney function and determine the severity of the blockage include the following: Creatinine, BUN (blood urea nitrogen), and electrolyte levels Complete blood count (CBC) Diuretic renal scan Urine culture Voiding cystourethrogram (VCUG; used to rule out vesicoureteral reflux)
, and electrolyte levels. Complete blood count (CBC) Diuretic renal scan. Urine culture. Voiding cystourethrogram (VCUG; used to rule out vesicoureteral reflux)")
71
UPJ Obstruction : Treatment
Newborns with UPJ obstruction and hydronephrosis are placed on antibiotics to prevent infection and are monitored with renal ultrasound every 3 to 6 months. If UPJ obstruction causes a significant reduction in renal function, a surgical procedure called pyeloplasty is performed to remove the obstruction. Patients require follow-up care for several years following pyeloplasty. Tests to evaluate kidney function are performed regularly (6 months to 1 year). The success rate for patients who undergo pyeloplasty is higher than 95%.
. The success rate for patients who undergo pyeloplasty is higher than 95%.")
73
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

74
VUR : Incidence 17–37% of prenatal ultrasounds M:F = 1:10 (redhair …)
Healthy children : 1 % Children with UTI : up to 50 % with VUR ! 30 % hereditary (how?) siblings in 75 % asymptomatic : screening because risk of scarring and reflux nefropathie
 siblings in 75 % asymptomatic : screening because risk of scarring and reflux nefropathie.")
75
VUR : Types & Grades Primary reflux Secondary reflux
Grade I results in urine reflux into the ureter only. Grade II results in urine reflux into the ureter and the renal pelvis, without distention (hydronephrosis). Grade III results in urine reflux into the ureter and the renal pelvis, causing mild hydronephrosis. Grade IV results in moderate hydronephrosis. Grade V results in severe hydronephrosis and twisting of the ureter.
. Grade III results in urine reflux into the ureter and the renal pelvis, causing mild hydronephrosis. Grade IV results in moderate hydronephrosis. Grade V results in severe hydronephrosis and twisting of the ureter.")
76
VUR : Causes Primary reflux : abnormality in the intravesical ureter (short or superolaterally / if duplication : lower pole). This condition often resolves as the child grows and the ureter lengthens (L: ). Other causes: abnormalities in detrusor muscle tissue of the bladder, abnormalities in the location of the urethral opening (e.g., hypospadias), and abnormalities in the shape of the urethral opening: high pressure, dysfunctional voiding
. Other causes: abnormalities in detrusor muscle tissue of the bladder, abnormalities in the location of the urethral opening (e.g., hypospadias), and abnormalities in the shape of the urethral opening: high pressure, dysfunctional voiding.")
77
VUR : Causes Secondary reflux is often caused by urinary tract infection (e.g., cystitis) that results in inflammation and swelling of the ureter. UTI may cause vesicoureteral reflux or vesicoureteral reflux may promote the growth of bacteria in the urinary tract, causing UTI (One-third of UTIs in children are caused by vesicoureteral reflux). Secondary reflux may also be caused by urinary tract abnormalities (e.g., narrowing, or stricture, of the ureter; duplicated ureters; ureterocele) and obstructions (e.g., UPJ obstruction, stones, tumor).
 that results in inflammation and swelling of the ureter. UTI may cause vesicoureteral reflux or vesicoureteral reflux may promote the growth of bacteria in the urinary tract, causing UTI (One-third of UTIs in children are caused by vesicoureteral reflux). Secondary reflux may also be caused by urinary tract abnormalities (e.g., narrowing, or stricture, of the ureter; duplicated ureters; ureterocele) and obstructions (e.g., UPJ obstruction, stones, tumor).")
78
VUR : Scarring scar-risk: 1) UTI (Big Bang : scar distorsion - intrarenal reflux) 2) sterile reflux + high P (check lower tractus) complications : - hypertension (10 %) - renal failure (DMSA)
 sterile reflux + high P (check lower tractus) complications : - hypertension (10 %) - renal failure (DMSA)")
79
VUR : Signs and Symptoms
UTI Bedwetting (nocturnal enuresis) Hydronephrosis / Distention in the abdomen (caused by HN) Failure to thrive Hypertension, caused by kidney damage Nausea and vomiting Proteinuria Pyelonephritis, kidney damage, and progressive renal failure
 Hydronephrosis / Distention in the abdomen (caused by HN) Failure to thrive. Hypertension, caused by kidney damage. Nausea and vomiting. Proteinuria. Pyelonephritis, kidney damage, and progressive renal failure.")
80
VUR : Diagnosis reflux opsporen bij . kind met pyelonefritis ("febriele UWI") . jongen met UWI . meisje < 5j met UWI . meisje > 5j met > 2 x UWI voiding cystogram (Tc ?) – passive / active
 – passive / active.")
81
VUR : Diagnosis The most common radiologic studies for the evaluation of reflux are the voiding cystourethrogram and the isotope cystogram. The isotope cystogram is more sensitive than the voiding cystourethrogram Only the voiding cystourethrogram provides enough anatomic detail to identify the severity of reflux and the presence of anatomic abnormalities. In boys: initial work-up should include a voiding cystourethrogram to detect urethral abnormalities such as urethral diverticulum or posterior Urethral valves.

82
VUR : Diagnosis Prenatal ultrasound
Bladder ultrasound (to detect abnormalities that cause reflux) Renal ultrasound and renal scan (to evaluate hydronephrosis, kidney growth, and scarring) Urodynamic studies (e.g., filling cystometrogram, voiding cystometrogram)
 Renal ultrasound and renal scan (to evaluate hydronephrosis, kidney growth, and scarring) Urodynamic studies (e.g., filling cystometrogram, voiding cystometrogram)")
83
spontane genezing a 1/ graad
u resol. scarring G1 10 % 90 % 10 % G2 35 % 75 % 15 % G3 30 % 50 % 30 % G4 20 % 40 % 50 % G5 5 % % 85 %

84
VUR : Treatment : Grade I - III
AB profylaxis : daily low-dose antibiotics (e.g., trimethoprim-sulphamethoxazole, amoxicillin) tot reflux verdwenen of risico op scarring klein (postpuberteit) FOLLOW UP ULTRASOUND & URINALYSIS mictietraining (voiding regime) anticholinergica (oxybutinin, propant.)
 tot reflux verdwenen of risico op scarring klein (postpuberteit) FOLLOW UP ULTRASOUND & URINALYSIS. mictietraining (voiding regime) anticholinergica (oxybutinin, propant.)")
85
VUR : Treatment : Grade I - III
AB met lage serum-/hoge urine- concentratie gering effect op de darmflora nitrofurantoine (1-2 mg/kg pm)(G6PDH) cefalexin ( mg) TMP(-SMX) (2 mg/kg) (bili-albumine)
(G6PDH) cefalexin ( mg) TMP(-SMX) (2 mg/kg) (bili-albumine)")
86
VUR : Treatment : Grade IV - V
Secondary reflux that does not resolve with antibiotic treatment, or that results in UTI despite antibiotic therapy (called breakthrough infections), and primary reflux that is severe (grades IV and V) require surgery to prevent permanent kidney damage. heelkunde igv. doorbraak-UWI scarring bij controle-echo follow-up na heelkunde blijvend vereist (subklinische scarring) STING : 70 % ipv. 98 % ( %) : collageen - autoloog vet - Teflon
, and primary reflux that is severe (grades IV and V) require surgery to prevent permanent kidney damage. heelkunde igv. doorbraak-UWI scarring bij controle-echo. follow-up na heelkunde blijvend vereist (subklinische scarring) STING : 70 % ipv. 98 % ( %) : collageen - autoloog vet - Teflon.")
87
URETEROCOELE duplicatie-ectopie (bovenpool) (meisjes, 10 % bilateraal)
50 % + VUR ." prenatale hydronefrose" .UWI

88
URETEROCOELE echo en cystogram isotopen (MAG3) (HUW)
R/ . endoscopische incisie (+/- 2° reïmplantatie) bovenpool-resectie pyelopyelostomie
 . bovenpool-resectie . pyelopyelostomie.")
90
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

91
De twee meest voorkomende blaasproblemen bij kinderen zijn :
INCONTINENTIE (Wetting) PLASPROBLEMEN (Voiding Dysfunction)
 PLASPROBLEMEN (Voiding Dysfunction)")
92
ENURESIS : Het blijven voorbestaan van een ongecontroleerde mictie
NOCTURNA : geen controle ‘s nachts DIURNA : geen controle overdag

93
The Cinderella Subject
“Even though nobody dies from incontinence, it is hardly a glamorous condition” “Treatment = A Dream Come True”

94
E.N. : History Papyrus Ebers, dated 1550 B.C. : potions from animals, organs, or plants (e.g. placing a comb from a hen in tepid water and giving it to the child to drink or putting testicles from a hare into a glass of wine and having the child drink it, drying the comb of a cock and scattering it over the enuretic's bed) Mid-1800s : induce blisters on the child's sacrum 1927 (Friedell) : psychic treatment by restricting fluids and injecting sterile water along with positive reassurance that this treatment will work => 87% success rate and those children who did not respond were found to have low urine specific gravity at night. This monitoring of urine concentration holds significant merit in regards to common treatment modalities used today. Punishment and public humiliation were also historically very common. Unfortunately, parents still punish their children for wetting the bed. 61% of parents perceived bed-wetting as a significant problem and that one-third dealt with it by punishment.
 Mid-1800s : induce blisters on the child s sacrum (Friedell) : psychic treatment by restricting fluids and injecting sterile water along with positive reassurance that this treatment will work. => 87% success rate and those children who did not respond were found to have low urine specific gravity at night. This monitoring of urine concentration holds significant merit in regards to common treatment modalities used today. Punishment and public humiliation were also historically very common. Unfortunately, parents still punish their children for wetting the bed. 61% of parents perceived bed-wetting as a significant problem and that one-third dealt with it by punishment.")
95
Chronologie van de mictiecontrole (stadia)
van 0 tot 6 maand : reflexblaas van 6 maand tot 1 jaar : grotere volumes kleinere frequentie van 1 tot 2 jaar : gevoel van volle blaas van 3 tot 4 jaar : onderdrukken van mictiereflex vanaf 4 jaar : volledige blaascontrole

96
Stadium I : van 0 tot 6 maand
Zuivere reflexblaas Frequentie : ongeveer 20/dag Prikkeling afferente banen ruggemerg reflex (S2- S4) efferente banen detrusorcontractie sfincterrelaxatie Geen centrale invloeden
 efferente banen. detrusorcontractie. sfincterrelaxatie. Geen centrale invloeden.")
97
Stadium II : van 6 maand tot 1 jaar
Het volume per mictie stijgt De mictiefrequentie daalt is het gevolg van een onbewuste inhibitie van de mictiereflex (centraal) is eveneens het gevolg van de groei van de blaascapaciteit
 is eveneens het gevolg van de groei van de blaascapaciteit.")
98
Stadium III : van 1 tot 2 jaar
Het gevoel van een volle blaas ontwikkelt zich Eerste aanzet tot controle van de mictie

99
Stadium IV : van 3 tot 4 jaar
ontwikkelen van de eigenschap, ook bij niet volle blaas, om te plassen of plassen te inhiberen = mogelijkheid om een reflex te onderdrukken bij elke blaasvulling

100
Controle darm (stoelgang) versus blaas (mictie)
eerst : stoelgangscontrole ‘s nachts daarna : stoelgangscontrole overdag daarna : mictiecontrole overdag daarna : mictiecontrole ‘s nachts

101
ENURESIS (definitie) = het blijven voortbestaan van deze (infantiele) ongecontroleerde mictie, hetzij overdag, hetzij ‘s nachts.
 = het blijven voortbestaan van deze (infantiele) ongecontroleerde mictie, hetzij overdag, hetzij ‘s nachts.")
102
Enuresis: Definitions & Categories
Diurnal enuresis Wetting that occurs during waking hours (daytime incontinence). Nocturnal enuresis Wetting that occurs during sleep. Uncomplicated enuresis Nocturnal enuresis, normal physical examination, and negative urine analysis and urine culture. Complicated enuresis Secondary onset of enuresis, history of urinary tract infection(s), abnormal neurologic examination, and a history of voiding dysfunction.
. Nocturnal enuresis. Wetting that occurs during sleep. Uncomplicated enuresis. Nocturnal enuresis, normal physical examination, and negative urine analysis and urine culture. Complicated enuresis. Secondary onset of enuresis, history of urinary tract infection(s), abnormal neurologic examination, and a history of voiding dysfunction.")
103
Enuresis diurna Various degrees 15% - 20% of bed-wetters
prevalence rapidly decreases in children over 5 years of age +/- symptoms indicative of urgency and/or frequency: squatting, sitting on one's heel, crossing the legs, "dancing," or holding the perineum (bladder instability / detrusor-sphincter dyssynergia) => valid voiding history!
 => valid voiding history!")
104
E.N. : Terminology Primary
Bed-wetting since birth without any significant periods of dryness. Secondary Onset of bed-wetting after the child has been dry for at least 6 months. Monosymptomatic Nocturnal enuresis that occurs with normal daytime urination. Polysymptomatic Nocturnal enuresis associated with urinary frequency, urgency or other signs of bladder instability.

105
Enuresis Nocturna : Voorkomen
op 5 jaar : 15 à 20 % van de kinderen daarna wordt elk jaar 10 à 15 % van de bedwateraars droog op 15 jaar heeft nog 1 à 2 % der jongeren E.N.

106
Enuresis Nocturna : Voorkomen
Primair: % Secundair: % 15 à 20 % der patiëntjes hebben ook E.D. Jongens hebben meer E.N., meisjes meer E.D.

107
E.N. : Incidence

108
E.N. : causes Genetic Factors
both parents bed-wetters => their children 77% chance only one parent => 43% molecular genetic heterogeneity (chromosomes 13q and 12q)
")
109
E.N. : oorzaken Enuresis = een symptoom, geen ziekte
Late rijpheid of ontwikkelingsstoornis Nachtelijke polyurie Slaapstoornissen Psychische factoren Urinaire infectie zonder oorzaak

110
ONTWIKKELINGSSTOORNIS
Het grootste deel geneest met de tijd toch Urodynamisch valt op: kleine blaascapaciteit onstabiele contracties Stoornis in het aanleren van zaken

111
E.N. : oorzaken Reduced Bladder Capacity
Bed-wetting occurs when functional bladder capacity is reached The bladder is too small to hold all the urine that is produced at night. Urodynamic studies indicate that children with NE exhibit frequent uninhibited bladder contractions and a lower functional bladder capacity. Conversely, another study revealed that bladder instability was found in only 15% of patients with isolated NE, when compared to 97% having both diurnal and nocturnal enuresis (Breugelmans, et al.) Children with monosymptomatic PNE rarely exhibit abnormal urodynamic findings and usually have a normal bladder capacity. This group may either produce large volumes of urine at night, thereby reaching functional bladder capacity despite normal bladder function, or may be unresponsive during sleep, or both.
 Children with monosymptomatic PNE rarely exhibit abnormal urodynamic findings and usually have a normal bladder capacity. This group may either produce large volumes of urine at night, thereby reaching functional bladder capacity despite normal bladder function, or may be unresponsive during sleep, or both.")
112
E.N. : oorzaken Sleep Disorders "deep sleepers“ : arousal disorder ??
NO : The fact that the child is a deep sleeper or difficult to arouse may be merely a characteristic and not a cause bed-wetting occurs only during the deep sleep stages or when transitioning from one sleep stage to another ??? NO : enuresis is independent of sleep stages and occurred randomly throughout the night proportional to the time spent in each sleep stage => Treatment should be directed towards limiting urine output at night rather than sleep modulation.

113
SLAAPSTOORNISSEN Ze slapen «te diep»
Nachtelijk EEG zou een verband aantonen??? Een bepaald percent (10%?) zou E-tekenen op EEG vertonen
 zou E-tekenen op EEG vertonen.")
114
E.N. : oorzaken Sleep Apnea (Obstructive sleep apnea syndrome (OSAS))
Occasionally, nocturnal enuresis is an associated issue. Cessation of NE with the surgical removal of the obstructing lesion (adenotonsillectomy) or treatment with continuous positive airway pressure. Children who experience NE associated with sleep apnea historically snore heavily due to enlarged tonsils and adenoids. Explanations for enuresis in these situations are related to alteration in hormonal activity and renal pathology: urine volume and sodium excretion are increased at night in patients with OSAS => nocturnal polyuria.
 or treatment with continuous positive airway pressure. Children who experience NE associated with sleep apnea historically snore heavily due to enlarged tonsils and adenoids. Explanations for enuresis in these situations are related to alteration in hormonal activity and renal pathology: urine volume and sodium excretion are increased at night in patients with OSAS => nocturnal polyuria.")
115
E.N. : oorzaken Endocrine Factors (pituitary ADH)
Urine output occupies a circadian rhythm in normal individuals, with a decrease of urine production normally occurring at night. E.N. children have lower mean nocturnal urine osmolalities and higher mean urinary excretion rates However sometimes no alteration in both nocturnal ADH secretion or nighttime urine output. Furthermore, nocturnal polyuria may be a factor in the presence or absence of abnormal ADH secretion. This endocrine-based theory may apply to some enuretics but does not account for all cases.

116
NACHTELIJKE POLYURIE Veranderd dag-nachtritme van de ADH-secretie
bij een normaal kind stijgt de ADH-productie ‘ s nachts minder en meer geconcentreerde urine

117
NACHTELIJKE POLYURIE Bij enuretische kinderen stijgt die niet ‘ s nachts blaascapaciteit (van overdag) wordt overschreden E.N. MAAR : Waarom worden ze dan niet wakker van die volle blaas?
 wordt overschreden E.N. MAAR : Waarom worden ze dan niet wakker van die volle blaas")
118
E.N. : causes Psychological Factors
incidence of psychopathology is relatively infrequent Enuresis itself can result in psychologic, individual, and interpersonal distress The onset of secondary enuresis may be brought about by an emotional or psychological disturbance, for example, divorce, death in the family, illness, emotional or physical trauma, or the birth of a new sibling. Even though there may be instances wherein a psychologic event may cause secondary enuresis, it is usually a matter of a relapse of physiologic enuresis.

119
PSYCHISCHE FACTOREN ? Emotionele Stoornissen Onrijpheid
Minder zelfzeker

120
E.N. : oorzaken ADHD (Attention-deficit hyperactivity disorder )
>10 Y : an increase in the percentage of children with E.N. will have symptoms associated with ADHD … it is difficult if not impossible to determine whether the disruptive behavior of children with ADHD stems from the embarrassment of enuresis or whether enuresis is one of the several "soft" signs of an underlying neurologic disorder.

121
E.N. : oorzaken Diet 10% of children are believed to have a food-related allergy as a key factor in their nocturnal enuresis. Patients who were on food-restrictive diets for managing childhood migraines and/or hyperactive behavior had cessation in their nocturnal enuresis Avoid: products high in caffeine and sugar, citrus fruits and juices, dairy products (especially afternoon), artificially colored foods and drinks, and chocolate.
, artificially colored foods and drinks, and chocolate.")
122
E.N. : oorzaken Secondary nocturnal enuresis may be caused by psychological issues (e.g., death in the family, sexual abuse, extreme bullying) and is often associated with stress. It may also result from an acquired condition such as diabetes, hyperthyroidism, seizure disorder (e.g., epilepsy), and obstructive sleep apnea (OSA). Heart condition that causes an irregular heartbeat (heart block). Neurological disorders (e.g., cerebral palsy, spinal cord disorders, neurogenic bladder). Urinary tract infection (UTI; e.g., cystitis). Sickle cell disease Chronic renal failure R.T.A.
 and is often associated with stress. It may also result from an acquired condition such as diabetes, hyperthyroidism, seizure disorder (e.g., epilepsy), and obstructive sleep apnea (OSA). Heart condition that causes an irregular heartbeat (heart block). Neurological disorders (e.g., cerebral palsy, spinal cord disorders, neurogenic bladder). Urinary tract infection (UTI; e.g., cystitis). Sickle cell disease. Chronic renal failure. R.T.A.")
123
E.N. : oorzaken Meer a-symptomatische bacteriurie bij
enuretische kinderen

124
E.N. : Causes - Summary Bladder Capacity (small / unstable): no evidence Urine Concentration: in 2/3 ADH production is not increased at night. This does not explain why they do not wake up. Sleep and Arousal: not all children are deeper sleepers Sleep Apnoea (stopping breathing) is associated with night time wetting. This is usually manifest by snoring, stopping breathing and restarting with a gasp. Large adenoids may be to blame. Social and Emotional: Whilst in some children that wet, there may sometimes be associated emotional or behavioural problems, the association is not clear. Maturity: Delayed maturity would account for the spontaneous cure rate, however as most children respond very rapidly to an alarm, this is less likely as a cause. Toilet Training: Variable opinions exist. Attempts to train before 18 months may inhibit the normal processes of getting dry. There is also postulated a sensitive period for bladder training around the 3rd year of life. Stresses around this time may interfere with the chances of the dryness. Constipation: Often associated with wetting. Possibly by giving confusing signals to the brain, or by "irritating the bladder“ Medical Problems: Uncommon - Must Exclude Structural problems / InfectionsDietCaffeine can irritate the bladder Fluids: Reducing fluids is of NO Help Increased fluids during the day is helpful.
 is associated with night time wetting. This is usually manifest by snoring, stopping breathing and restarting with a gasp. Large adenoids may be to blame. Social and Emotional: Whilst in some children that wet, there may sometimes be associated emotional or behavioural problems, the association is not clear. Maturity: Delayed maturity would account for the spontaneous cure rate, however as most children respond very rapidly to an alarm, this is less likely as a cause. Toilet Training: Variable opinions exist. Attempts to train before 18 months may inhibit the normal processes of getting dry. There is also postulated a sensitive period for bladder training around the 3rd year of life. Stresses around this time may interfere with the chances of the dryness. Constipation: Often associated with wetting. Possibly by giving confusing signals to the brain, or by irritating the bladder Medical Problems: Uncommon - Must Exclude Structural problems / InfectionsDietCaffeine can irritate the bladder. Fluids: Reducing fluids is of NO Help Increased fluids during the day is helpful.")
125
ENURESIS (Onderzoek) 1. Anamnese 2. Klinisch onderzoek
3. Urine onderzoek 4. Uroflow 5. Echo Nieren en Blaas, evt. IVP - DTPA 6. Cystogram (Kleppen, reflux) 7. UDO (instabiliteit) 8. Neurologisch onderzoek 9. Psychisch onderzoek
 7. UDO (instabiliteit) 8. Neurologisch onderzoek. 9. Psychisch onderzoek.")
126
ANAMNESE Wanneer is het begonnen? (periodes van grote «droogte»?)
Welke vorm? E.N. of E.D. Hoe vaak? elke Nacht? meerdere malen per nacht? Slaappatroon

127
ANAMNESE Hoe veel? een beetje kliedernat
Andere symptomen? urgency moeilijke mictie Familiale enuresis? Plaspatroon - Vochtinname (kalender)
")
128
KLINISCH ONDERZOEK Volle blaas? Genitalia? Lage rug (S.B.)
Meatus fimosis Lage rug (S.B.) Neurologisch: reflexen, stap, sensorium Bloeddruk
 Neurologisch: reflexen, stap, sensorium. Bloeddruk.")
129
WELKE ONDERZOEKEN TE DOEN?
1. Bij de onverwikkelde vorm van 1 tot 5 2. Bij de verwikkelde vorm alles

130
E.N. : Definitions & Categories
Diurnal enuresis Wetting that occurs during waking hours (daytime incontinence). Nocturnal enuresis Wetting that occurs during sleep. Uncomplicated enuresis Nocturnal enuresis, normal physical examination, and negative urine analysis and urine culture. Complicated enuresis Secondary onset of enuresis, history of urinary tract infection(s), abnormal neurologic examination, and a history of voiding dysfunction.
. Nocturnal enuresis. Wetting that occurs during sleep. Uncomplicated enuresis. Nocturnal enuresis, normal physical examination, and negative urine analysis and urine culture. Complicated enuresis. Secondary onset of enuresis, history of urinary tract infection(s), abnormal neurologic examination, and a history of voiding dysfunction.")
131
ENURESIS (Onderzoek) 1. Anamnese 2. Klinisch onderzoek
3. Urine onderzoek 4. Uroflow 5. Echo Nieren en Blaas, evt. IVP - DTPA 6. Cystogram (Kleppen, reflux) 7. UDO (instabiliteit) 8. Neurologisch onderzoek 9. Psychisch onderzoek
 7. UDO (instabiliteit) 8. Neurologisch onderzoek. 9. Psychisch onderzoek.")
132
E.N. : Diagnosis : RX vesicoureteral reflux hydronephrosis
bladder instability detrusor sphincter dyssynergia urethral abnormalities

133
BEHANDELING VAN ENURESIS
2 grote groepen : 1. Gedragstherapie 2. Medicamenteuze therapie

134
BEHANDELING VAN ENURESIS
Dubieus : niet drinken na een bepaald uur het kind ophalen en laten plassen Slecht : het kind straffen

135
BEHANDELING VAN ONVERWIKKELDE ENURESIS
Basisvraag : Houding van het kind? Houding van de ouders? Houding van de omgeving? (broers en zussen) Therapie wordt slechts ingesteld als de enuresis een probleem wordt (zelden voor 5 à 6 jaar)
 Therapie wordt slechts ingesteld als de enuresis een probleem wordt (zelden voor 5 à 6 jaar)")
136
BEHANDELING VAN ENURESIS
1. Gedragstherapie motivatietherapie conditionering 2. Medicamenteuze therapie

137
GEDRAGSTHERAPIE Motivatietherapie kind aanmoedigen
kalender met NAT/DROOG (pos. Feedback) duurt meestal lang cure rate (monotherapie): 25% "marked improvement" > 70%
 duurt meestal lang. cure rate (monotherapie): 25% marked improvement > 70%")
138
GEDRAGSTHERAPIE Conditioneringstherapie = Plaswekker
Werking : reactie op urine. Het kind wordt wakker gedurende of na de mictie. Het kind associëert de bel met het gevoel van een volle blaas. Het leert aldus het gevoel van een volle blaas bewust kennen.

139
PLASWEKKER (Bedenkingen)
Niet bij te kleine kinderen (vanaf 7 j) Sommigen worden er niet wakker van Sommigen worder er bang van Deep sleeper => motivatie van ouders ! success rate : 65% not the quick way (time & energy consuming) stop indien > 4 weken droog 30 % recidiveert later
 Sommigen worden er niet wakker van. Sommigen worder er bang van. Deep sleeper => motivatie van ouders ! success rate : 65% not the quick way (time & energy consuming) stop indien > 4 weken droog. 30 % recidiveert later.")
140
Bladder Retention Training
based on the presumption that the child has a decreased functional bladder capacity normal bladder capacity = {Age (in years) + 2} x 28 ml = {24.5 x Age (in years)} + 62 ml (< 9 Y) conscious attempts at "bladder stretching" by prolonging the voiding intervals cure rate : only 35% (probably due to the demanding nature of the program and the element of bladder instability and urinary frequency/urgency seen in some of these children)
 + 2} x 28 ml. = {24.5 x Age (in years)} + 62 ml (< 9 Y) conscious attempts at bladder stretching by prolonging the voiding intervals. cure rate : only 35% (probably due to the demanding nature of the program and the element of bladder instability and urinary frequency/urgency seen in some of these children)")
141
FARMACOTHERAPIE in vraag gesteld: Sedativa Stimulantia
Alfa-adrenergica centraal sfincter

142
= management therapy rather than a cure: high relapse rates after short-term treatment
long-term therapy either continuously or on an as-needed basis (sleepovers or camp)
")
143
FARMACOTHERAPIE VAN ENURESIS
Tricyclische antidepressiva IMIPRAMINE = TOFRANIL ADH-analogen DESMOPRESSINE = MINIRIN Parasympatholytica OXYBUTININE = DITROPAN / DRIPTANE

144
TOFRANIL Werking : Verandering slaapmechanisme
Anticholinergisch-antispasmodisch Anti-depressief (humeur) Beïnvloeden van ADH-secretie
 Beïnvloeden van ADH-secretie.")
145
TOFRANIL DOSIS : 6 tot 8 jaar: 25 mg/dag meer dan 8 jaar: 50 à 75 mg/dag gedurende minimaal 6 maand

146
TOFRANIL NEVENWERKINGEN : angst slapeloosheid droge mond nausea karakterstoornissen Overdoses can cause myocardial effects (arrhythmias and conduction blocks) and hypotension. World Health Organization (WHO) does not recommend using this drug for nocturnal enuresis.
 and hypotension. World Health Organization (WHO) does not recommend using this drug for nocturnal enuresis.")
147
MINIRIN WERKING : Nachtelijke diurese doen dalen tot een volume, kleiner dan de functionele blaascapaciteit The effect usually lasts 6 to 12 hours 68 % respons (monosympt. EN)
")
148
MINIRIN DOSIS (spray) : 2 à 4 pufjes ‘ s avonds (1 pufje = 10 microgram) NEVENWERKINGEN : - congestion, rhinitis, mild headache, and epistaxis - Hyponatriemie secondary to water intoxication (zeldzaam) => CAVE HIGH WATERINTAKE !!!!!!!!!! Relaps ! (use as safety – sleepovers etc. – until growout)
 => CAVE HIGH WATERINTAKE !!!!!!!!!! Relaps ! (use as safety – sleepovers etc. – until growout)")
149
Minirin : Cave H20-intoxicatie
Rule out : cystic fibrosis renal disease endocrine disorders other disorders that may produce electrolyte imbalances Psychogenic polydipsia and habit polydipsia DDAVP should not be used in instances where fluid and electrolyte balance would be affected, such as fever, viral illnesses, vomiting, or diarrhea, where increased fluid intake is required.

150
Combination Therapy Behaviour modification Alarm Therapy
Minirin : quick onset counters delayed effect of other two

151
DITROPAN WERKING : inhibitie van de onstabiele contracties
mucosa-anesthetisch vergroten van de blaascapaciteit

152
DITROPAN DOSIS : 5 mg 2 à 3x/dag
NEVENWERKINGEN: Droge mond Gezichtsstoornissen Constipatie Gedragsstoornissen / Humeur Hyperpyrexie in de zon

153
Success rates of 90% have been reported for enuretic children with significant daytime incontinence and/or bladder instability. However, anticholinergics are rarely beneficial for children with exclusive nocturnal enuresis.

154
FARMACOTHERAPIE : RESULTATEN
Initieel : 50 % Op termijn : 25 % (na stoppen medicatie) Eventueel : * kuur herhalen * combinatietherapie
 Eventueel : * kuur herhalen * combinatietherapie.")
155
E.N. : Other treatments Oral antibiotics (e.g., Bactrim®, amoxicillan, Macrobid®, Levaquin®) are used to treat UTIs that cause bed-wetting. Surgery Structural abnormalities in the urinary system (e.g., ectopic ureter) and other conditions, such as obstructive sleep apnea and heart block, may require surgery.
 and other conditions, such as obstructive sleep apnea and heart block, may require surgery.")
156
Hypnotherapy Hypnotherapy is not based on conditioning therapy. It involves the explanation of the bladder-brain connection and teaching self-hypnosis and visual imaging to the child in responding to a full bladder during sleep. One controlled study comparing hypnotherapy with imipramine reported a 76% dryness rate after initiating both types of therapy. After 9 months, 68% of the hypnotherapy group remained dry in comparison to only 24% in the imipramine group.

157
OORZAKEN VAN PLASMOEILIJKHEDEN
Neurogene blaas Blaastumor (zeer zeldzaam) Megacystis (+ megaureter) Prune-Belly Urethrakleppen Dyssynergie blaas-sfincter Stenosen (meatus) Vreemd voorwerp
 Megacystis (+ megaureter) Prune-Belly. Urethrakleppen. Dyssynergie blaas-sfincter. Stenosen (meatus) Vreemd voorwerp.")
158
AANDOENINGEN VAN DE URETHRA
Bij Jongens : Urethrakleppen vaak afwijkingen van de HUW Bij Meisjes : Terminale urethrastenose zelden afwijkingen van de HUW

162
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

163
SCROTUM " ZWELLING " ACUUT NIET-ACUUT TORSIO HYDROCOELE
EPID.-ORCHITIS TUMOR VARICOCOELE

164
TORSIO testis : . hooggelegen . geen cremaster-reflex . gezwollen funniculus . opheffen pijnvermindering appendix : . blue dot . harde nodulus (bovenpool)
")
165
EXTRAVAGINALE : eerste weken
INTERMITTENTE : "bell-clapper" DIAGNOSTIEK : indien reële twijfel (snelheidsfactor !)
")
166
urine : pyurie echo scrotum (kleurendoppler) isotopenscan -itis :- echo nieren (ectop.ureter + hydronef.) obstructie lagere tractus uitsluiten
 - obstructie lagere tractus uitsluiten.")
167
Hydrocoele = open peritoneovaginaal kanaal
sluit in 1ste levensjaar (- 6 %; prematuren) pijnloze translucente "blauwe" zwelling (wenen) variant : funniculuscyste
 pijnloze translucente blauwe zwelling (wenen) variant : funniculuscyste.")
168
DD liesbreuk bij het kind (zeldzaam) : lateraal
R/ heelkunde : . na 1 jaar . < 1 jaar (non-communicans, cyste) geen punctie : recidief / peritonitis
 geen punctie : recidief / peritonitis.")
169
TUMOR soms acute zwelling na mineur trauma (slechte angiogenesis)
R/ heelkunde +/- chemo overleving YolkSac : > 90 %

170
TUMOR Kiemcel : . Yolk sac . Teratoma . Seminoma
Stroma : . Leydig Sertoli Granulosa cel Bindweefsel (fibroma, leiomyoma) Epidermoid cyste Secundaire tumoren
 Epidermoid cyste. Secundaire tumoren.")
171
Varicocoele v. spermatica ----> v. renalis / VCI
v. pudenda ext. ----> v. saphena longa v. cremasterica ----> v. iliaca ext. v. deferentia ----> v. iliaca int.

172
9 – 17 % (1:2 verminderde sperma-kwaliteit en kwantiteit)
bij 30 % van infertiele mannen unilateraal => infertiel ?

173
°t °C bijnier-metabolieten (catecholamines, steroiden, PG) Hypoxie Bij unilat. Varicocoele toch bilateraal verhoogde flow en °t-stijging (bilat. Effect) Ook antistofproductie tegen links => rechts
 Ook antistofproductie tegen links => rechts.")
174
risicofactor = testiculaire hypotrofie ...
wait & see : cave : . Irreversiebele hypotrofie . oligo-terato-astheno-spermie (OTA) relatie OTA en seminoma : 5:1000
 relatie OTA en seminoma : 5:1000.")
175
R/ varicocoele : Heelkunde
Palomo Ivanissevitch Goldstein laparoscopie retrograde embolisatie antegrade sclerosering (MIT)
")
176
varicocoele : beware ! cave acuut rechts geen ontzwellen bij neerliggen retroperitoneale tumor / renaal cel carcinoma (trombose VCI of v. renalis)
")
177
SCROTUM "KRIMPING " CRYPTORCHIDIE RETRACTIELE TESTIS

178
RETRACTIELE TESTIS + cremaster reflex koude omgeving angstig kind
in-uit-fenomeen normaal scrotum

179
CRYPTORCHIDIE 3 % (x 10 bij prematuren) 10 % bilateraal (?)
< 3 m (tot 1 j) : 75 % spontane descensus (95 % bij prematuren) indaling door - tractie gubernaculum (8ste maand) - stijgen intra-abd. druk endocrinol.-neurol.
 : 75 % spontane descensus. (95 % bij prematuren) indaling door - tractie gubernaculum (8ste maand) - stijgen intra-abd. druk - endocrinol.-neurol.")
180
Signs and symptoms An undescended testicle is not located within the scrotum. The condition may be associated with other abnormalities of the genitourinary system (e.g., hypospadias).
.")
181
Oorzaken Vader of broer + => hogere kans
Low birth weight (< 2500 g) Maternal exposure to estrogen during the first trimester Multiple birth (e.g., twin, triplet) Premature birth (before 37 weeks gestation) Small size for gestational age
 Maternal exposure to estrogen during the first trimester. Multiple birth (e.g., twin, triplet) Premature birth (before 37 weeks gestation) Small size for gestational age.")
182
Verwikkelingen van Cryptorchidie
seminoma (x 10) (20 % contralat.) torsio ( 50 % + Ca) open peritoneovaginaal kanaal (90 %) infertiliteit (bilateraal : 70 %) trauma bij sport
 (20 % contralat.) torsio ( 50 % + Ca) open peritoneovaginaal kanaal (90 %) infertiliteit (bilateraal : 70 %) trauma bij sport.")
183
Behandeling van cryptorchidie
unilateraal : R/ heelkunde bilateraal : hormonale poging human chlorionic gonadotropin hormone (hCG: IU) may be combined with gonadotropin- releasing hormone (GnRH) therapy, but has not been approved in the United States (Kryptocur: 3x/d 400 mu) (succes %) (ook D/)
 may be combined with gonadotropin- releasing hormone (GnRH) therapy, but has not been approved in the United States (Kryptocur: 3x/d 400 mu) (succes %) (ook D/)")
185
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle varicocoele hypospadias phimosis

186
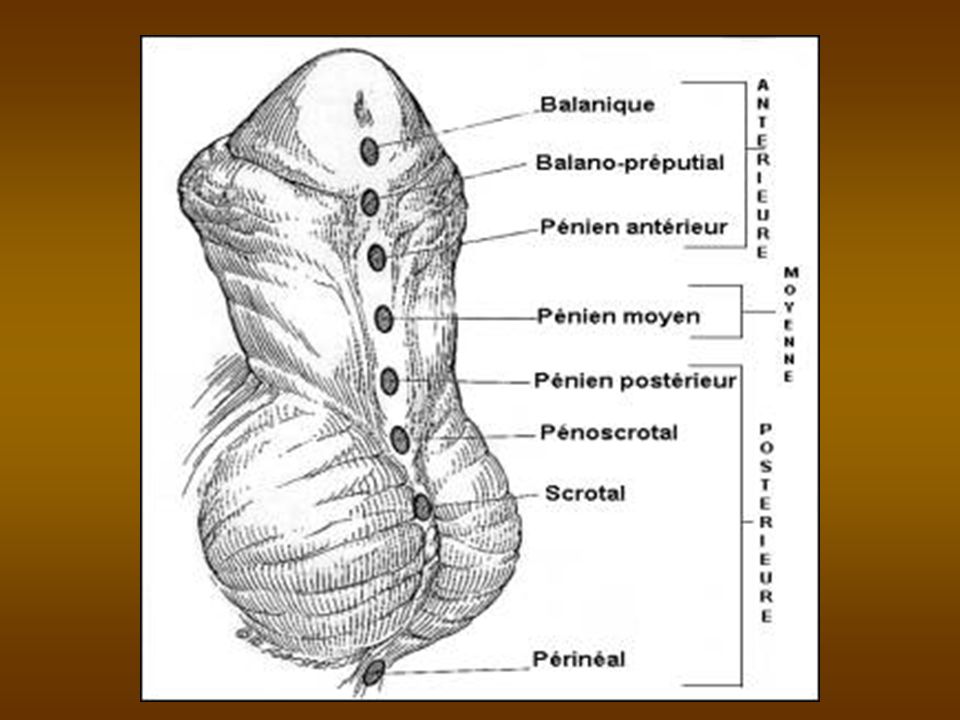
HYPOSPADIAS = slecht ontwikkeld corpus spongiosum
(”incomplete development of the urethra in utero between 8 and 20 weeks of gestation”) te korte urethra kromming naar onder bij erectie (chordae)
 te korte urethra. kromming naar onder bij erectie (chordae) ")
187
HYPOSPADIAS VOORKOMEN * 1 op 500 geboortes
* niet erfelijk (? – vide infra) (meer bij Joden en Italianen)
 (meer bij Joden en Italianen) ")
188
Hypospadias : Causes Genetic factors are suggested by an increase in the condition in twins compared to a single birth. Human chorionic gonadotropin (hCG) is a hormone produced in early pregnancy that stimulates the production of estrogen and progesterone. In the case of twins, the production of hCG may not be sufficient to prevent incomplete urethral development. There is also a 20% chance that an infant born with hypospadias has a family member with the condition. Endocrinological factors include low levels of androgens (e.g., testosterone, androsterone) and the infant’s cells’ inability to use these substances effectively may also result in hypospadias. Androgens are substances that stimulate the development of male characteristics. Maternal exposure to increased levels of progesterone, common during in vitro fertilization (IVF), increases the risk for hypospadias in the infant. Environmental exposure to estrogen during urethral development may also be a risk factor. Exposure can result when the mother ingests pesticides on fruits and vegetables and milk from pregnant cows.
 is a hormone produced in early pregnancy that stimulates the production of estrogen and progesterone. In the case of twins, the production of hCG may not be sufficient to prevent incomplete urethral development. There is also a 20% chance that an infant born with hypospadias has a family member with the condition. Endocrinological factors include low levels of androgens (e.g., testosterone, androsterone) and the infant’s cells’ inability to use these substances effectively may also result in hypospadias. Androgens are substances that stimulate the development of male characteristics. Maternal exposure to increased levels of progesterone, common during in vitro fertilization (IVF), increases the risk for hypospadias in the infant. Environmental exposure to estrogen during urethral development may also be a risk factor. Exposure can result when the mother ingests pesticides on fruits and vegetables and milk from pregnant cows.")
189
HYPOSPADIAS VORMEN * Glandulair (65 %) * Peniel (15 %)
* Scrotaal (20 %)
 ")
192
Hypospadias : Symptoms
Voiding problems Ejaculation problems Sexual problems: the farther the opening is from the tip of the glans, the more likely curvature in the penis (chordee) is present.
 is present.")
194
Hypospadias : Complications
severe hypospadias undescended testicles inguinal hernias upper urinary tract anomalies vesicoureteral reflux

195
Hypospadias : Treatment Goals
Allow the patient to urinate standing Correct curvature of the penis (chordee) Present a cosmetically acceptable appearance Preserve fertility
 Present a cosmetically acceptable appearance. Preserve fertility.")
196
HYPOSPADIAS : THERAPIE
Lichte Vormen (corona) * niets doen * besnijden?
 * niets doen * besnijden ")
197
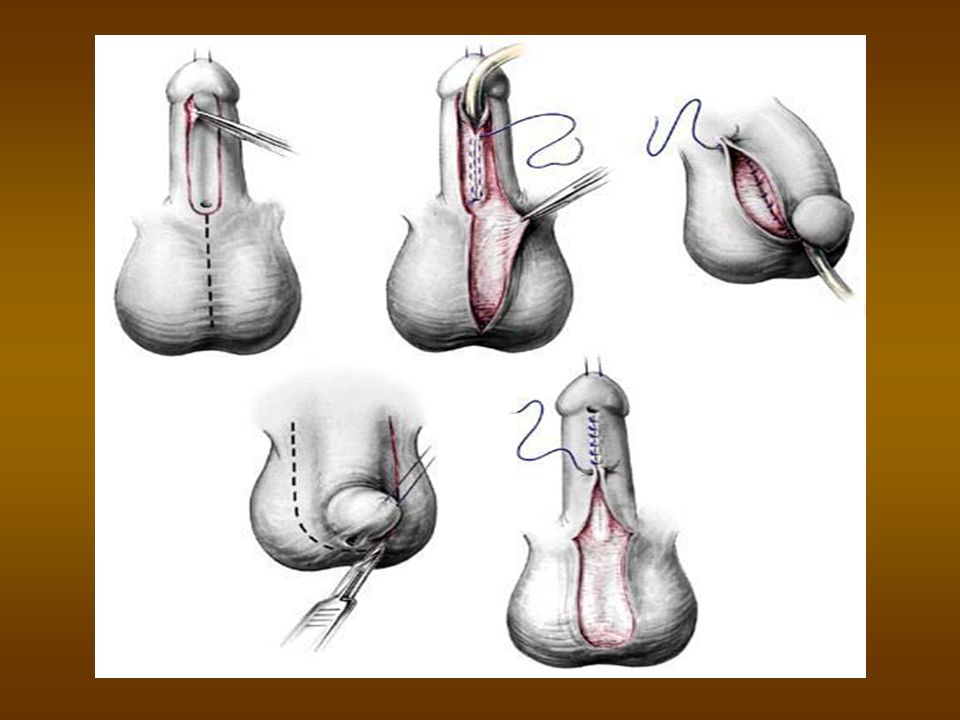
HYPOSPADIAS : THERAPIE
Ernstige vormen * resectie van de chordee * constructie van een neo-urethra - gesteelde flap (penis of scrotum) - vrije flap (penis, wang) Tussen 6 – 18 maanden leeftijd.
 - vrije flap (penis, wang) Tussen 6 – 18 maanden leeftijd. ")
200
CONGENITALE PENISKROMMING
Congenitale verharding in de tunica albuginea van de corpora carvernosa geeft bij erectie kromming naar de kant van de verharding

201
CONGENITALE PENISKROMMING : THERAPIE
Lichte Vormen : NESBITT (inkeping aan de contralaterale zijde) Ernstige Vormen : excisie en inplanten van een non- allergisch materiaal (Lyodura, Lyoplant)
 Ernstige Vormen : excisie en inplanten van een non- allergisch materiaal (Lyodura, Lyoplant) ")
203
INDEX UTI antenatal hydronephrosis ureteropelvic junction obstruction
vesicoureteral reflux nocturnal enuresis cryptorchid testicle Varicocoele hypospadias phimosis

204
FIMOSIS Echte fimosis : te nauwe ring
Valse fimosis : verklevingen tussen voorhuid en glans

205
FIMOSIS : VERWIKKELINGEN
Infectie Mictiestoornissen Sexuele problemen Parafimosis Peniscarcinoma

206
FIMOSIS : THERAPIE Wanneer ? 4 à 5 jaar (tenzij verwikkelingen)
")
207
What is a normal foreskin ?
The skin over the tip of penis normally folds on itself as a sleeve and attaches to the head of penis. This extra skin is called foreskin. In newborn babies the under surface of the foreskin is fused to the head of penis. In 95% of newborn babies the foreskin can not be pulled back. This is referred to as ‘physiological phimosis’ or ‘non retractile foreskin’. However as they get older it separates slowly; by years of age, usually the foreskin can be pulled back. (90 % at 3 Y => examine !)
")
208
Problems of the persisting non-retractile foreskin?
accumulation of white discharge called ‘smegma’ foreskin balloons during urination straining and only dribbling when passing urine Balanitis or UTI Scarring of the skin at the tip Paraphimosis

209
Treatment of Complications
Balano-posthitis : meestal zuiver lokaal Parafimosis : * manuele reductie * incisie ring

210
Is it advisable to practice retraction to make it better?
Caveat overdo =>soreness and bleeding Excessive retraction with damage =>scarring => real phimosis Boys older than 5 years of age can attempt self retraction at bath. It is essential to put it back after retraction, as skin left retracted can result in swelling called ‘paraphimosis’.

211
Use of the Foreskin glans stays moist => improves sexual sensitivity increasesd skin mobility => provides increased stimulation of the stretch receptors in the penile skin reduced premature ejaculation by protecting the corona of the glans penis from direct stimulation

212
FIMOSIS : THERAPIE Hoe ? * Circumcisio * Voorhuidplastie
1 maand Hydrocortisone 0.05 – 0. %, 2x/d (?)
")
213
Circumcision : “an old religion”
some researchers believe that circumcision was practiced as early as 6,000 years ago on the west coast of Africa bas-relief from a tomb in Sakkara (Egypt; about 2200 BC portrayed in an Egyptian tomb wall carving from around 2400 B.C., yet its orgins and ritual meanings remain obscure. (The Tomb of Nyhetep-Ptah at Giza and the Tomb of Ankhmahor at Saqqara)
")
214
Circumcision : “an old religion”
In ancient days, circumcision or even more extensive mutilation of the external genitalia was carried out on defeated enemies, captives, or slaves as a sign of subjugation. Circumcision was also a puberty or premarital rite, or as an absolution against the feared toxic influences of vaginal (hymenal) blood.
 blood.")
215
Circumcision : “an old religion”
distinct meaning with Abraham: (Genesis 17:12-13) sign and seal of the covenant between God and God's chosen people (According to dictate, the practice was to be universal among all male members of the community; whether freemen or slaves. Furthermore, the rite was to be performed on the eighth day of life.)
 sign and seal of the covenant between God and God s chosen people. (According to dictate, the practice was to be universal among all male members of the community; whether freemen or slaves. Furthermore, the rite was to be performed on the eighth day of life.)")
216
Circumcision : Beyond religion
1870: Routine circumcision as a preventative or cure for masturbation was proposed in Victorian times in America. Masturbation (and / or inflammated foreskin) was thought to be the cause of a number of diseases. Circumcision in America, England and the other countries received a strong boost during each of the World Wars, because it was claimed that the procedure was necessary for soldiers for "hygienic reasons". Some soldiers who refused to be circumcised, were disciplined and/or received dishonourable discharges.
 was thought to be the cause of a number of diseases. Circumcision in America, England and the other countries received a strong boost during each of the World Wars, because it was claimed that the procedure was necessary for soldiers for hygienic reasons . Some soldiers who refused to be circumcised, were disciplined and/or received dishonourable discharges.")
217
Comstock Act = Cockstorm Act ?
Circumcision became an omnibus procedure, supposedly effective against dozens of disorders which were widely feared yet poorly understood, circumcision lent itself naturally to sexual diagnoses, which in turn helped complete the transition to routine care for male infants. Late Victorian America was of course notoriously ill at ease with human sexuality. The infamous Comstock Act of 1873 captured an attitude toward sex, awkward and censorious, which was widespread within the middle and upper classes. For a culture nervous about sex, manifestations of infant and child sexuality seemed especially disturbing, contradictions of children's pristine purity. Since the Enlightenment, doctors in Western Europe and America had identified masturbation as a cause of illnesses. In the course of the nineteenth century it was linked to madness, idiocy, epilepsy, and from these to a multitude of other psychological, behavioral, and pathological conditions. "The most serious forms of disorder attributable to this cause are spinal paralysis, locomotor-ataxia, and convulsions," declared a physician at Virginia's South-Western Asylum, "masturbatory insanity”. For ages the Catholic Church had taught that masturbation, because it existed apart from marriage and procreation, was a mortal sin. But the medical theory that masturbation caused disease presented a more immediate threat. Fittingly in the age of Darwin, biology joined God as the punisher of transgression.

218
Americans gave a new twist to John Wesley's famous saying that cleanliness is next to godliness. Increasingly they identified personal cleanliness with good morals, sound health, and upright character. So the Victorian moralist William A. Alcott admonished his readers "that he who neglects his person and dress will be found lower in the scale of morals, other things being equal, than he who pays a due regard to cleanliness." The same argument could be applied broadly. During the later Victorian period, an age obsessed with racial and social hierarchies, there was an allure to ranking civilizations, peoples, and social groups from clean to dirty. Used increasingly by the middle class as a caliper of moral judgment and evidence of material prosperity, "cleanliness indicated control, spiritual refinement, breeding; the unclean were vulgar, coarse, animalistic. Cleanliness, in other words, became an essential criterion of social respectability. Dirt was seen as a moral, and thus a social, hazard whose dangers people would strive assiduously to avoid.

219
Here is an example of what another sexaphobic American doctor had to say about masturbation in 1903:
"It (self abuse) lays the foundation for consumption, paralysis and heart disease. It weakens the memory, makes a boy careless, negligent and listless. It even makes many lose their minds; others, when grown, commit suicide.... Don't think it does no harm to your boy because he does not suffer now, for the effects of this vice come on so slowly that the victim is often very near death before you realize that he has done himself harm. It is worthy of note that many eminent physicians now advocate the custom of circumcision..." (Mary R. Melendy, MD, The Ideal Woman - For Maidens, Wives and Mothers, 1903)
 lays the foundation for consumption, paralysis and heart disease. It weakens the memory, makes a boy careless, negligent and listless. It even makes many lose their minds; others, when grown, commit suicide.... Don t think it does no harm to your boy because he does not suffer now, for the effects of this vice come on so slowly that the victim is often very near death before you realize that he has done himself harm. It is worthy of note that many eminent physicians now advocate the custom of circumcision... (Mary R. Melendy, MD, The Ideal Woman - For Maidens, Wives and Mothers, 1903)")
220
Circumcision : Beyond religion
Circumcision as a safeguard against malignancies was an idea with considerable appeal, for, like their descendants a century later, Victorians were horrified by cancer. The awful public ordeal of General Ulysses S. Grant, who died from what his doctors called "an epithelioma" of the soft palate, transfixed the public and the medical community alike. Post-mortem analysis convinced Grant's physicians that his disease had been caused by irritation, in his case irritation in the mouth and throat from years of smoking cigars. Epithelioma, one of his doctors announced, "as a rule starts from local irritation, and unlike other forms of cancer, is not dependent upon hereditary disposition to the disease." Penile cancers were said to develop according to similar principles. Thus, in a world bereft of effective therapies, the finding that in many cases of penile cancer it had been demonstrated "conclusively that the prepuce is the inciting cause as well as the initial point of attack" became an influential argument to operate before disease struck." Venereal infections, owing to their virulent contagiousness and social stigma, were feared nearly as much as cancer. Syphilis in particular raged out of control, seeming to approach epidemic proportions. During the 1880s and 1890s medical researchers made great strides in understanding the pathology of syphilis, and later gonorrhea.

221
Circumcision prevents cancer and syphilis:
epidemiological study of American Jews in 1890, confirming low rates of morbidity, including penile epithelioma, syphilis as well as infectious diseases like diphtheria and tuberculosis, within Jewish communities, even among the poorest classes => Together with (wonderful timed) antiseptic and anesthetic surgical improvements, this led to nation-wide circumcision.
 antiseptic and anesthetic surgical improvements, this led to nation-wide circumcision.")
222
"Circumcision," performed on babies, wrote a New York doctor, "is no more of an operation than vaccination." And as the Jews had long since discovered, babies needed no chloroform or cocaine. "Infants only a few years old may be held down by two assistants and the operation done without any anesthetic, Samuel Newman advised. For his own part, Newman preferred to bind his young patients "to a board after the Indian fashion of strapping the papoose... to hold the child firmly in place until the operation is ended."

223
Medical circumcision thus assumed its own place in the fin-de-siècle search for rank and social order. It signified precisely that aversion to dirt - and not just dirt, but vulgarity, nasty habits, and diseases - which symbolically set one on a higher plane. Undoubtedly this was the enduring source of its appeal to patients and parents. Outside Judaism, circumcision was exclusively the province of doctors and patients with enough money to pay for an elective procedure. Physicians privately suggested it to parents immediately after the birth of a son. Circumcision, they professed, represented state-of-the-art medical knowledge and surgical practice. The operation itself was simple, eminently safe; moreover, it immediately reduced the infant's chances of becoming infected with the deadly diseases of childhood. With each passing year maternity care and childbirth for the middle and upper classes was shifting from a domestic event managed by midwives, relatives, and friends into a medical event managed by physicians. Midwives rarely performed circumcisions, so having one's foreskin removed was necessarily a byproduct of having been delivered by a physician. It was a token of the medicalization of childbirth; literally a symbol of the rising authority of the medical profession over the laity.

224
Considered in terms of the march of medical science, circumcision is an anomaly. But as a synecdoche for the history of clinical practice - above all of surgery - it is remarkably, not to say disturbingly, comprehensible. The visible hands that treat patients are not the hands of scientists, but of practitioners whose conventions, habits, and modes of practice are molded first by watching their teachers, then their peers. This is the process of practical medical education, and also of cultural transmission.

226
Motivations for Uncircumcision
No matter what reasons have been given to substantiate routine male circumcision throughout the centuries, countless circumcised males have been unhappy about what was done to them—so much so that some have relentlessly sought, by whatever means were available to them at the time, to undo the effects of the circumcision they did not choose for themselves.

227
Motivations for Uncircumcision
How the West was won … "I think that I could have accepted a deformity that was an accident of nature, but I can't accept that someone did that to me." (John A. Erickson. Making America Safe for Foreskins)
")
228
Motivations for Uncircumcision
Under Antiochus IV (168 BC) Hellenistic ideals such as public nakedness at athletic games or in public baths, emerged in Judea and forced Jews to stretch their foreskins with a special weight, the Pondus Judaeus, to cover the glans (I. Maccabees 1) Similar efforts are reported in the Talmud during the time of Hadrian (132 AD). Evidence from mummified remains predating the Ankhmahor relief indicates that the practice had been established centuries earlier.
 Hellenistic ideals such as public nakedness at athletic games or in public baths, emerged in Judea and forced Jews to stretch their foreskins with a special weight, the Pondus Judaeus, to cover the glans (I. Maccabees 1) Similar efforts are reported in the Talmud during the time of Hadrian (132 AD). Evidence from mummified remains predating the Ankhmahor relief indicates that the practice had been established centuries earlier.")
229
Jewish athletes of the time were able to accomplish this feat because their circumcisions had removed only the typically protruding tip of the infant foreskin, leaving the inner lining of the infant foreskin attached to the glans—thus leaving the mature male with a "miniforeskin" that could rather easily be drawn forward over the glans. Not until about 140 AD, after the Bar Kokba uprising, was the more radical procedure of "stripping bare the glans" added to the Jewish circumcision rite so that the sign of the covenant could not be undone.

230
Motivations for Uncircumcision
levying of special "temple tax“ selective military call-ups of circumcised youths persecution of Jews under the Nazi regime

231
Motivations for Uncircumcision
THE GOLDEN SIXTIES … Why was it, asked the editors of the Journal of the American Medical Association in 1963, that an operation so well accepted by practitioners for its power to "'relieve' phimosis, to 'prevent' infection, to be 'prophylaxis' against carcinoma" had attracted no interest from scientists in the medical research establishment? Castigating circumcision as "the rape of the phallus," a physician at the University of Maryland blamed its popularity on women. "Perhaps not least of the reasons why American mothers seem to endorse the operation with such enthusiasm," he wrote, "is the fact that it is one way an intensely matriarchal society can permanently influence the physical characteristics of its males." Return of Hippocrates : “Primum non nocere”

232
Ironically, but predictably in the context of the history of medical arguments for circumcision, some doctors have conjectured that removing the foreskin may protect men from the most dreaded epidemic of the post-modern world: the human immunodeficiency virus (HIV). Using retrospective data (the epidemiological equivalent of empiricism) from a venereal disease clinic in Kenya, for example, researchers observed that there were higher rates of HIV infection in the home communities of uncircumcised than circumcised men. Ignoring racial, ethnic, and sociocultural variables - the chief factors dictating whether or not an African boy is circumcised in the first place - they hypothesized that circumcision might serve to inhibit the transmission of the AIDS virus. One wonders whether this theory will endure. But within a medical community desperate to find some weapon against AIDS, its appeal is understandable. Even a physician who is a sober skeptic of the methodologies behind such studies allows that they "do suggest that HIV may be more infective during heterosexual intercourse if the mate partner is uncircumcised and has a mucosal or cutaneous ulcer." AIDS, the nemesis of modern science and medicine, remains a mystery. By some equally mysterious process, it is surmised, circumcision may help.
 from a venereal disease clinic in Kenya, for example, researchers observed that there were higher rates of HIV infection in the home communities of uncircumcised than circumcised men. Ignoring racial, ethnic, and sociocultural variables - the chief factors dictating whether or not an African boy is circumcised in the first place - they hypothesized that circumcision might serve to inhibit the transmission of the AIDS virus. One wonders whether this theory will endure. But within a medical community desperate to find some weapon against AIDS, its appeal is understandable. Even a physician who is a sober skeptic of the methodologies behind such studies allows that they do suggest that HIV may be more infective during heterosexual intercourse if the mate partner is uncircumcised and has a mucosal or cutaneous ulcer. AIDS, the nemesis of modern science and medicine, remains a mystery. By some equally mysterious process, it is surmised, circumcision may help..")
233
Het “Voorhuid-Verlangen”
“Why would any man who's never had one want one?"

234
Motivations for Uncircumcision
- Sixties < Seventies : * increased keratinization * psychologic (I’m different) * victim (I did not have the choice) => decreased sexual pleasure NOCIRC (National Organization of Circumcision Information Resource Centers) NOHARMM (National Organization to Halt the Abuse and Routine Mutilation of Males) NORM (National Organization of Restoring Man) DOC (Doctors Opposing Circumcision) NRC (Nurses for the Rights of the Child) Homosexuals => heterosexuals Many nations that adopted routine infant male circumcision as a "health measure" early in the 20th century have moved away from the practice.
 * victim (I did not have the choice) => decreased sexual pleasure. NOCIRC (National Organization of Circumcision Information Resource Centers) NOHARMM (National Organization to Halt the Abuse. and Routine Mutilation of Males) NORM (National Organization of Restoring Man) DOC (Doctors Opposing Circumcision) NRC (Nurses for the Rights of the Child) Homosexuals => heterosexuals. Many nations that adopted routine infant male circumcision as a health measure early. in the 20th century have moved away from the practice.")
235
In 1949, the important work of Gairdner appeared in Britain, which led to the virtual cessation of medically-motivated circumcision in that country. Australia and New Zealand now also have very low rates (5% or less). The largest problem remains in the United States, where the procedure has become culturally entrenched. The American public largely still believes circumcision to be a useful procedure, even though the rest of the world does perfectly well without it. It is worth noting that in 1996 the Canadian Paediatric Society issued a statement depreciating the value of circumcision in rather strong terms. Most Canadian provinces have dropped insurance coverage for circumcision, and the rest are expected to follow in the next year or so. Circumcision never became an issue in continental Europe and in most of Asia, where the vast majority of men are intact. Religious circumcision is popular in some African, Muslim and Middle Eastern countries.

236
Porn Flakes (Kellogg, Graham and the Crusade for Moral Fiber)
"All kinds of stimulating and heating substances; high-seasoned food; rich dishes; the free use of flesh; and even the excess of aliment; all, more or less -- and some to a very great degree -- increase the concupiscent excitability and sensibility of the genital organs..." -- Sylvester Graham "A remedy [for masturbation] which is almost always successful in small boys is circumcision...The operation should be performed by a surgeon without administering an anesthetic, as the brief pain attending the operation will have a salutary effect upon the mind...In females, the author has found the application of pure carbolic acid to the clitoris an excellent means of allaying the abnormal excitement. " -- Dr. John Harvey Kellogg

237
International Symposium on Circumcision (ISC), 1989
We recognize the inherent right of all human beings to an intact body. Without religious or racial prejudice, we affirm this basic human right. We recognize the foreskin, clitoris and labia are normal, functional body parts. Parents and/or guardians do not have the right to consent to the surgical removal or modification of their children's normal genitalia. Physicians and other health-care providers have a responsibility to refuse to remove or mutilate normal body parts. The only persons who may consent to medically unnecessary procedures upon themselves are the individuals who have reached the age of consent (adulthood), and then only after being fully informed about the risks and benefits of the procedure. We categorically state that circumcision has unrecognized victims.
, and then only after being fully informed about the risks and benefits of the procedure. We categorically state that circumcision has unrecognized victims.")
238
Human right ? Informed consent is not enough …
If it ain't broken, don't fix it

239
MYTHS AND FACTS

240
MYTH: A circumcised penis is cleaner.
Cleansing the intact penis is similar to cleansing intact labia and is simply a matter of common sense. After the age of reason, one hopes that a boy who has already learned to tie his shoes can be cajoled into washing behind his ears and directed to clean his penis. It is painless, takes only a few seconds, and when it takes any longer is probably associated with a smile.--Leonard J. Marino, MD The AAP itself refuted this myth by saying, "...good personal hygiene would offer all the advantages of routine circumcision without the attendant surgical risk".

241
MYTH: Circumcision is minor surgery.
"Minor surgery is one that is performed on someone else," says Stanford University Medical School Professor, Dr. Eugene Robin. Circumcision, like all surgery, has inherent risks, which include hemorrhage, infection, mutilation, and death. Circumcision is not a minor procedure and there are many unrecognized victims. Dr. Robin recommends, "If it ain't broke, don't fix it!".

242
MYTH: Circumcision prevents penile cancer.
Penile cancer, which has been documented in both circumcised and intact men, is a rare disease of elderly men and one of the least common malignancies. It represents 0.5% of all cancers in men and occurs at "...a rate of less than one case per 100,000 per year". The low incidence of penile cancer in the United States is not due to circumcision because "...the population of American men born before 1940, now in the group at risk for this cancer, is a group of predominantly UNCIRCUMCISED men". Research indicates that good hygiene prevents penile cancer and "It is an incontestable fact...there are more deaths from circumcision each year than from cancer of the penis".

243
MYTH: Women with circumcised partners have a lower incidence of cervical cancer.
Inaccurate studies of the 1950s Jewish women have a relatively low rate of cervical cancer Moslem women have a much higher rate. According to the most recent AAP report, "...evidence linking uncircumcised men to cervical carcinoma is inconclusive. The strongest predisposing factors in cervical cancer are a history of intercourse at an early age and multiple sexual partners".

244
Cancer of the cervix in women is due to the Human Papilloma Virus
Cancer of the cervix in women is due to the Human Papilloma Virus. It thrives under and on the foreskin from where it can be transmitted during intercourse. An article in the British Medical Journal in April 2002 suggested that at least 20% of cancer of the cervix would be avoided if all men were circumcised. Surely that alone makes it worth doing?

245
MYTH: Circumcision will decrease the risk of sexually transmitted diseases, including AIDS.
There is an epidemic of sexually transmitted diseases, including AIDS, in the United States, where the majority of sexually active men are circumcised. It is not the foreskin that causes these diseases, and circumcision will not prevent them. It is relatively more important to alter exposure to infectious agents than male susceptibility to them. It is education about safe sex, not amputation of healthy body parts of newborns, that is sane preventative medicine for sexually transmitted diseases.

246
Another British Medical Journal article in May 2000 suggested that circumcised men are 8 times less likely to contract the HIV virus. (It is very important here to say that the risk is still far too high and that condoms and safe sex must be used - this applies also to preventing cancer of the cervix in women who have several partners).
..")
247
Age of male circumcision and risk of prevalent HIV infection in rural Uganda. Kelly R, Kiwanuka N, Gray RH. Department of Population Dynamics, Johns Hopkins University, School of Hygiene and Public Health, Baltimore OBJECTIVE: To assess whether circumcision performed on postpubertal men affords the same level of protection from HIV-1 acquisition as circumcisions earlier in childhood. CONCLUSIONS: Prepubertal circumcision is associated with reduced HIV risk, whereas circumcision after age 20 years is not significantly protective against HIV-1 infection. Age at circumcision and reasons for circumcision need to be considered in future studies of circumcision and HIV risk.

248
MYTH: Circumcision prevents urinary tract infection.
Many studies reflecting an increase in UTIs among intact boys are "retrospective," may have "methodologic flaws," and "may have been influenced by selection bias". Since one fourth of my male infant patients are not circumcised, and if the frequency of UTI in the uncircumcised is as high as it is said to be, I should be seeing many UTIs in male infants.

249
MYTH: Circumcision prevents foreskin infections.
Yes, it does, in both males and females, and removing all the teeth would prevent cavities. Where does this argument end? Infections are caused by invading organisms and can be treated effectively with antibiotics. Fear of infection is no reason to routinely amputate a tonsil, an appendix, or a foreskin.

250
MYTH: Circumcision prevents phimosis & complications.
Using the surgical treatment of circumcision to prevent phimosis is a little like preventing headaches by decapitation. It works but it is hardly a prudent form of treatment.--Eugene Robin, MD. Smegma is probably the most maligned body substance. It is a normal, natural body product no more harmful than ear wax. It is definitely not a carcinogen...Adult smegma serves as a protective, lubricating function for the glans, just as adult smegma in women protects the clitoris". When scar tissue has formed at the preputial opening secondary to premature retraction or ammoniacal burns, there are surgical techniques (Y-V-plasties and Z-plasty), which can be employed to make the foreskin retractable without amputating it. If phimosis has been caused by a rare pathologic condition such as balanitis serotica obliterans, only the afflicted area need be removed. However, this is generally a less acceptable intervention from estetical point of view. HERE IT IS BETTER TO PERFORM A CIRCUMCISION.
, which can be employed to make the foreskin retractable without amputating it. If phimosis has been caused by a rare pathologic condition such as balanitis serotica obliterans, only the afflicted area need be removed. However, this is generally a less acceptable intervention from estetical point of view. HERE IT IS BETTER TO PERFORM A CIRCUMCISION.")
251
MYTH: A boy should look like his dad.
Ironically, this argument was never used when medical circumcision was initiated just a hundred years ago. Nor has it been used by Western feminists working to stop female circumcision in Africa. A simple explanation is all that is needed for children to understand that there are individual differences, and to help them feel good about themselves. A response something like this usually suffices: "People thought circumcision was important for health reasons when your dad (or brother) was born, but now we know better. Your body is perfect just the way it is. You did not need to be circumcised."
 was born, but now we know better. Your body is perfect just the way it is. You did not need to be circumcised.")
252
MYTH: It's better to circumcise babies because they won't remember the experience.
Quite the contrary. Overwhelming evidence indicates that experiences during the preverbal period affect the human being throughout life. An infant does retain significant memory traces of traumatic events. When a child is subjected to intolerable, overwhelming pain, it conceptualizes mother as both participatory and responsible regardless of mother's intent.

253
MYTH: Better to do it now because it would hurt more later.
This first erroneously assumes that a postnewborn circumcision will be necessary. The question of an uncircumcised child requiring later circumcision is used as a scare tactic--only in the United States. The question is not foreskin problems, but the attitude of the American medical profession in pushing what most physicians throughout the world consider unnecessary surgery. Worldwide, foreskin problems are treated medically, rarely surgically. Even if a circumcision were required later in life, the male would be able to understand the health problem, give an informed consent, and have the benefits of anesthesia and pain medication. Researchers Anand and Hickey report that "...neonates were found to be more sensitive to pain than older infants".

254
MYTH: Circumcision improves sexual staying power.
Following circumcision, changes occur to the sensitive mucous membrane of the glans penis. Due to this scarification process, circumcision does render the penis less sensitive. However, premature ejaculation continues to be the most common sexual complaint of American men, most of whom are circumcised, so that this rationale seems, at best, dubious.

255
MYTH: Christians should be circumcised like Jesus.
Circumcision became a controversy in the early Church because the first Christians were Jews. These Christians debated whether or not the Christian gentiles needed to be circumcised in order to be saved. Peter proclaimed that Christians were saved only through the grace of Jesus Christ. Paul later reaffirmed the concept: "For in Jesus Christ neither circumcision availeth anything nor uncircumcision; but faith which worketh by love".

256
MYTH: Jews don't question circumcision.
Reexamination of circumcision (brit milah) is occurring within the Jewish community itself. For Orthodox Jews, who accept brit milah solely as a religious (not a health) practice, the medical discussion is irrelevant. But for all other Jews, who take some comfort in the health attributes, a profound soul-searching may be anticipated. The answer will not be found in the epithet "anti-Semite". Jewish writings of the last decade illustrate this process: "A Mother Questions Brit Milah", "Letter to Our Son's Grandparents: Why We Decided Against Circumcision", "A Baby-Naming Ceremony, Rochester Society for Humanistic Judaism", and "Jesse's Circumcision". Health care providers who are aware of resources will be able to provide information to Jewish parents who are grappling with this difficult issue. The Alternative Brit Support Group is one such resource.
 is occurring within the Jewish community itself. For Orthodox Jews, who accept brit milah solely as a religious (not a health) practice, the medical discussion is irrelevant. But for all other Jews, who take some comfort in the health attributes, a profound soul-searching may be anticipated. The answer will not be found in the epithet anti-Semite . Jewish writings of the last decade illustrate this process: A Mother Questions Brit Milah , Letter to Our Son s Grandparents: Why We Decided Against Circumcision , A Baby-Naming Ceremony, Rochester Society for Humanistic Judaism , and Jesse s Circumcision . Health care providers who are aware of resources will be able to provide information to Jewish parents who are grappling with this difficult issue. The Alternative Brit Support Group is one such resource.")
257
MYTH: Parents have the right to decide whether or not to circumcise their son(s).
Body ownership rights are now being introduced as an issue in circumcision lawsuits that claim that every human being has an inherent, inalienable right to his own intact body.

258
MYTH: All circumcised men are happy that they were circumcised.
Support groups such as RECAP (RECover a Penis) [now called NORM] and an information network, UNCIRC (Uncircumcising Information and Resources Center), are rapidly uniting men who perceive themselves as victims of a sexual assault inflicted upon them during their earliest days of life and against which they were unable to defend themselves. Knowing that men who have realized their loss would prefer to have their normal bodies intact, and in light of the fact that conclusive evidence for circumcision as an effective health measure has never been established, health care professionals are ethically and morally obligated to put their scalpels down.
 [now called NORM] and an information network, UNCIRC (Uncircumcising Information and Resources Center), are rapidly uniting men who perceive themselves as victims of a sexual assault inflicted upon them during their earliest days of life and against which they were unable to defend themselves. Knowing that men who have realized their loss would prefer to have their normal bodies intact, and in light of the fact that conclusive evidence for circumcision as an effective health measure has never been established, health care professionals are ethically and morally obligated to put their scalpels down.")
260
Foreskin Restoration Foreskin restoration, also known as epispasm or decircumcision Celsus (25 BC-50 AD) was the first to give a detailed description of two surgical techniques for uncircumcision in his De medicina libri octo. Subsequent works, for example by Galen ( AD) and Paulus Aeginata in the seventh century, only contained a repetition of these methods without presenting any new aspects
 was the first to give a detailed description of two surgical techniques for uncircumcision in his De medicina libri octo. Subsequent works, for example by Galen ( AD) and Paulus Aeginata in the seventh century, only contained a repetition of these methods without presenting any new aspects.")
261
Foreskin Restoration Ambroise Paré gave a new impetus in the sixteenth century, suggesting the insertion of a catheter into the distal urethra to guarantee free passage of urine during postoperative healing. In this past century, Johann Friedrich Dieffenbach was the first to dedicate a whole chapter to the problem of "posthioplastice" in a modern textbook of plastic surgery. "Aryan doctors“ Nowadays, reports on surgical foreskin restoration are still rare.

263
A CLOSING REMARK: UNCIRCUMCISION AND THE FINE ARTS
From 1501 to 1504 Michelangelo Buonarroti created the statue of David. This representative of the Jewish people is shown with his penis not circumcised. Was Michelangelo just submitting to the aesthetic taste of his time, thereby making use of artistic liberty, as he had done before? Or did he fear any discredit of the Church or his customers by presenting such an obvious sign of Judaism as a circumcised penis? Some authors even postulated that Michelangelo had in mind to attach the face and weapons of David to the statue of Goliath.

Similar presentations