Download presentation
Presentation is loading. Please wait.

1
Health Services Annual Training
August 19, @ Educational Service Center 8:30 am - 12:00 pm

2
Today's Agenda Why are you here? Then and Now... Today’s plan
10 minute breaks After section 4 After Section 8 Noon Lunch Training Content Resources

3
Health Service Staff Model & Student Health Concerns
7 District Nurses 10 Schools + Homelink & ELC 8,200 students (1,171 average per Nurse) 281 Life Threatening Conditions 138 Anaphylaxis/Severe Allergies & 23 Diabetes Insulin D. 808 Asthma & 72 Seizure Conditions Overall ,925 students with Health Concerns Only employees that have been delegated by the School RN are allowed to work in the Health Center. These designated employees must also be: - Certified in First Aid/CPR - Trained by the School RN - Receive documented annual reviews of health room policies and procedures by the School RN
 281 Life Threatening Conditions. 138 Anaphylaxis/Severe Allergies & 23 Diabetes Insulin D. 808 Asthma & 72 Seizure Conditions. Overall ,925 students with Health Concerns. Only employees that have been delegated by the School RN are allowed to work in the Health Center. These designated employees must also be: - Certified in First Aid/CPR - Trained by the School RN - Receive documented annual reviews of health room policies and procedures by the School RN.")
4
Health Room & School Nurse Delegation
Health Room Assistant Office Professional Paraeducator - General Clerical Support Appropriate Delegation & Adequate Training

5
Delegated Staffing: Job Description Health Room Role
Office Professional Register new students and maintain student records including attendance, discipline and health information. Oversee health room and provide basic services in the absence of a nurse. Know and follow health, safety and emergency procedures of the district Paraeducator - General Clerical Support Assist students seeking care in the health room Provide general RN support, set appointments for parents to meet with RN, make arrangements for School Bell Health Room Assistant Provide health room management and assists in the implementation of the District health services programs. Assists students, staff and teachers with health-related issues.

6
Safe Schools Participants will:
1. Understand their training assignments with safe schools online and expectation for completion.

7
Safe Schools Online 1). Health Room Assistant Training by RN
Goal: To be completed by first day in position and then annually. Safe Schools Online Cources: Blood borne Pathogen Exposure Prevention, Health Emergencies Overview, HealthEmergencies: Asthma Awareness, Diabetes Education, Hemophilia, Life Threatening Allergies, Seizures, Coking & the Heimlich Maneuver, Medication Administration Basics, HIV Aids, AED Training, Heat Illness Prevention, Concussion. *First Aid Certified (every 2 years) 2). Health Room Para Educator and Secretary Annual August Training Goal: To be completed annually at the beginning of each new school year. Safe Schools Online Cources: Blood borne Pathogen Exposure Prevention, Health Emergencies Overview, Health Emergencies: Asthma Awareness, Diabetes Education, Hemophilia, Life Threatening Allergies, Seizures, Coking & the Heimlich Maneuver, Medication Administration Basics, HIV Aids, AED Training, Heat Illness Prevention, Concussion.
 2). Health Room Para Educator and Secretary Annual August Training Goal: To be completed annually at the beginning of each new school year. Safe Schools Online Cources: Blood borne Pathogen Exposure Prevention, Health Emergencies Overview, Health Emergencies: Asthma Awareness, Diabetes Education, Hemophilia, Life Threatening Allergies, Seizures, Coking & the Heimlich Maneuver, Medication Administration Basics, HIV Aids, AED Training, Heat Illness Prevention, Concussion.")
8
Safe Schools Online 3). General health related Training for All School Building Staff, New Certificated Hires, New Classified Hires, New Subs Certificated/Classified. Goal: To be completed by early September, Annually Safe Schools Online Courses: Blood borne Pathogen Exposure Prevention, Health Emergencies Overview 25 mins (Asthma Awareness, Diabetes Education, Life Threatening Allergies, Seizures) Individualized staff specific training for individual student with HCP/ECP Goal: As needed/promptly, ongoing RN provides one-on-one or small group setting training. Provides condition information and/or ECP
. General health related Training for All School Building Staff, New Certificated Hires, New Classified Hires, New Subs Certificated/Classified. Goal: To be completed by early September, Annually. Safe Schools Online Courses: Blood borne Pathogen Exposure Prevention, Health Emergencies Overview 25 mins (Asthma Awareness, Diabetes Education, Life Threatening Allergies, Seizures) Individualized staff specific training for individual student with. HCP/ECP Goal: As needed/promptly, ongoing. RN provides one-on-one or small group setting training. Provides condition information and/or ECP.")
9
Delegation Participants will:
1. Understand their role and limitations with school nurse delegation. 2. Understand when to seek clarification and guidance.

10
Delegation Defined Delegation is defined by the American Nurses’ Association as “the transfer of responsibility for the performance of an activity from one individual to another, while maintaining the accountability for the outcome.” The Nursing Care Quality Assurance Commission (NCQAC) has the legal authority (RCW and RCW ) to regulate nursing practice in order to safeguard the health and safety of citizens in Washington.
 has the legal authority (RCW and RCW ) to regulate nursing practice in order to safeguard the health and safety of citizens in Washington.")
11
Nurse Delegation A registered nurse may delegate tasks of nursing to another individual where the registered nurse determines that it is in the best interest of the patient. 1) The delegating nurse shall: a) Determine the competency of the individual to perform the task; b) Evaluate the competency of the individual to perform the tasks; c) Supervise the actions of the person performing the tasks; and d) Delegate only those tasks that are within the registered nurse’s scope of practice.
 The delegating nurse shall: a) Determine the competency of the individual to perform the task; b) Evaluate the competency of the individual to perform the tasks; c) Supervise the actions of the person performing the tasks; and. d) Delegate only those tasks that are within the registered nurse’s scope of practice.")
12
Nurse Delegation No person may coerce a nurse into compromising patient safety by requiring the nurse to delegate if the nurse determines that it is inappropriate to do so. Nurses shall not be subject to any employer reprisal or disciplinary action by the nursing care quality assurance commission for refusing to delegate tasks or refusing to provide required training for delegation if the nurse determines delegation may compromise patient safety.

13
Nurse Delegation Nurse delegation models the nursing process:
Assess – the student and the school employee’s competency Plan – documentation of the training and nursing care Implement – supervision requirements Evaluate – changes in student needs, changes in school personnel, activities, change the plan or continue

14
Nurse Delegation For school nurses, NCQAC (WAC ) Standards of Nursing Conduct or Practice discusses delegation of nursing tasks to non-licensed personnel (WAC ), and provides direction on how tasks may be delegated to a non- licensed individual by a licensed registered nurse. The delegating school nurse will be responsible for ongoing training and competency evaluations of the non-licensed personnel to safeguard the health and welfare of the students in their care. Even when unlicensed school personnel perform the task, the nurse who delegates the task, will retain responsibility for the outcome. Supervision of the unlicensed school personnel does not require the delegating nurse to be present in the same building, however the delegating school nurse should be available by phone for consultation.
 Standards of Nursing Conduct or Practice discusses delegation of nursing tasks to non-licensed personnel (WAC ), and provides direction on how tasks may be delegated to a non- licensed individual by a licensed registered nurse. The delegating school nurse will be responsible for ongoing training and competency evaluations of the non-licensed personnel to safeguard the health and welfare of the students in their care. Even when unlicensed school personnel perform the task, the nurse who delegates the task, will retain responsibility for the outcome. Supervision of the unlicensed school personnel does not require the delegating nurse to be present in the same building, however the delegating school nurse should be available by phone for consultation.")
15
Medication Delegation
House Bill 2247 allows registered school nurses to delegate the administration of the following medications: Oral medications Eye drops Ear drops Topical ointments Additionally, administration of an epinephrine autoinjector (Epi Pen) may be delegated by a licensed school nurse Recent changes in legislation may expand medications which may be delegated, however, the school board will need to review these legislative rulings and respond with policies
 may be delegated by a licensed school nurse. Recent changes in legislation may expand medications which may be delegated, however, the school board will need to review these legislative rulings and respond with policies.")
16
Nurse Delegation When accepting the delegation to perform medication administration in a school setting, the unlicensed school personnel performs this function under the supervision of the delegating licensed professional nurse. Unlicensed school personnel should only accept delegation that he/she knows is within his/her skill set or knowledge and should always contact the school nurse if unclear about administration of medication. Unlicensed staff have a responsibility to follow school district policy and procedures and report to the nurse immediately if they have any reason to believe they have made a medication error.

17
Nurse Delegation School district, school district employee, agent, or parent- designated adult who, acting in good faith and in substantial compliance with the student’s individual health plan and the instructions of the student’s licensed health care professional, provides assistance or services under RCW 28A shall not be liable in any criminal action or for civil damages in his or her individual or marital or governmental or corporate or other capacities as a result of the services provided under RCW 28A to students with diabetes.

18
Nurse Delegation The American Nurses Association (ANA) Code of Ethics states, “The Nurse is responsible and accountable for individual nursing practice and determines the appropriate delegation of tasks consistent with the nurse’s obligation to provide optimum patient care.” The National Council of State Boards of Nursing (NCSBN) states the delegate must be, “accountable for accepting the delegation and for his/her own actions in carrying out the task.”
 Code of Ethics states, The Nurse is responsible and accountable for individual nursing practice and determines the appropriate delegation of tasks consistent with the nurse’s obligation to provide optimum patient care. The National Council of State Boards of Nursing (NCSBN) states the delegate must be, accountable for accepting the delegation and for his/her own actions in carrying out the task.")
19
Medication Administration
Participants will: 1. Gain a basic knowledge of the Washington State WAC and of the LSSD policy on medication administration. 2. Gain a basic knowledge of medication administration, medication errors, classification, safety, and documentation. Always refer to individual student care plan

20
Medication Administration
Schools will administer health services per WAC A01155, including medication administration, to students who require this service during the school day. Therefore, school districts should have in place, policies and procedures that address how medications and other health services should be delivered. Lake Stevens School District policies for medication administration are included in the consent forms for Administration for Oral Medication and on our HCP forms.

21
Medication Administration
Prescribed medication must be sent to school in the original labeled container and the label should include: Name of student Expiration date of medication Name of medication, dosage and strength of medication Route of medication Name and address of pharmacy Name of the prescribing health care provider Date the prescription was dispensed.

22
Medication Administration
Student self medication is allowed under in certain situations, with a written health care providers authorization. Prescribing HCP shall include: The student demonstrated proper technique and is capable of administering the prescribed med. The name and purpose of the medication The prescribed dosage of medication The times at which or circumstances under which the medication may be given The time period for which the medication is prescribed The side effects and further instructions if order is for more than 15 days.

23
Medication Safety Medication safety:
The first dose of a medication should be given at home and not at school. Prescribed medication should be brought to school by parent or guardian and picked up by the same. Prescribed medication should be counted and the number of pills documented on the Medication Administration form and signed by 2 adults. Medication shall only be administered according to the health care provider’s instructions on the Medication Authorization form and should match the information on the prescription label No change in prescription can be made without authorization from prescribing HCP.

24
Storage and Disposal of Medication
Except for emergency medications (EpiPens and inhalers and antihistamines) all medications should be kept in a secure, locked container or cabinet accessible only to responsible authorized school personnel. Medications requiring refrigeration shall be kept in separate refrigerator in a supervised area. Temperature of that refrigerator will be checked on a regular basis Disposal of medications may be made at the Lake Stevens Police department office. Document disposal date.
 all medications should be kept in a secure, locked container or cabinet accessible only to responsible authorized school personnel. Medications requiring refrigeration shall be kept in separate refrigerator in a supervised area. Temperature of that refrigerator will be checked on a regular basis. Disposal of medications may be made at the Lake Stevens Police department office. Document disposal date.")
25
Medication Errors Medication Errors:
A medication error occurs when on the “6 rights of medication administration” has been violated, ie: Administering the wrong medication Administering the wrong dosage of medication Administering the medication at the wrong time Administering medication in the wrong way Administering medication to the wrong student Failing to document that medication was given or inaccurate documentation of medication given. Medication errors may result in adverse reactions to the student. These reactions could range from a rash to life threatening.

26
Medication Errors (con’t)
When a medication error occurs, follow these guidelines: Keep the student in the health room or office If the student has returned to class, have them escorted by an adult back to health room Observe the student’s status and document what you see Identify the incorrect dose or type of medication taken Notify the supervising school nurse or principal if medication was given by non-licensed personnel. Complete a Medication Administration Incident Report form. Call Parent/Guardian to inform of the incident.

27
The 6 Rights of Medication Administration
Right student Right medication Right dose Right time Right documentation Right route (eye drops, oral med, ear drops)
")
28
Classification of Medications
Prescription medications: have been ordered for treatment by a health care provider Controlled/scheduled meds: are medications that are potentially addictive and are regulated under the Controlled/scheduled Substance Act of 1970 Non-controlled/scheduled medication:require an order from a HCP. Over-the-counter (OTC) medications: OTC medications are administered to students according to district policy. OTC meds require a completed authorization form by parent/guardian and the student’s HCP.
 medications: OTC medications are administered to students according to district policy. OTC meds require a completed authorization form by parent/guardian and the student’s HCP.")
29
Field Trip Procedures-Medication
Notification and preparation for administering medications during a field trip should begin well in advance of the day of the field trip(at least 2 weeks). The medication should not be repackaged for field trips by school personnel and student medication bottle should have a pharmacy prescription label attached.
. The medication should not be repackaged for field trips by school personnel and student medication bottle should have a pharmacy prescription label attached.")
30
Medication Handouts Administration of Medication Policy Letter
Medication Dosage Log Medication Error Report Form Common Medication Abbreviations Glossary of Medical Terms Brand & Generic Names for Common Medications Common Medications Medication Administration Checlist (i.e. Oral, Liquid, Eye Drops, Oinment, Ear Drops, Topical Ointment, Inhalers, EpiPen)
")
31
Diabetes Participants will: 1. Gain a basic understanding of diabetes.
2. Identify signs and symptoms of low and high blood sugar. 3. Understand their role in treatment and emergency response. Always refer to individual student care plan

32
Diabetes Management Training For School Personnel Is Essential
For the immediate safety of students with diabetes For the long-term health of students with diabetes To ensure that students with diabetes are ready to learn and participate fully in school activities To minimize the possibility that diabetes-related emergencies will disrupt classroom activities

33
Diabetes Diabetes results from the failure of the pancreas to make insulin. Insulin is a hormone that is necessary for the body to convert sugar or glucose into energy. Without insulin, sugar accumulates in the blood causing symptoms.

34
Type 1 Diabetes Most children with diabetes have Type 1 Diabetes.
Pancreas makes too little or no insulin. Treatment consists of administering multiple doses of insulin, monitoring blood sugar levels throughout the day, eating nutritious meals and snacks, and following a regular exercise program.

35
Symptoms of Type 1 Diabetes
The symptoms of type 1 diabetes are due to an increase in the level of glucose in the blood. These symptoms may be mistaken for the flu. If left undiagnosed, the child with type 1 diabetes can lapse into a life- threatening condition known as diabetic ketoacidosis (DKA). Signs of DKA include vomiting, sleepiness, fruity breath, difficulty breathing, and if untreated, coma and death. Symptoms: • Increased thirst and urination • Weight loss • Blurred vision • Feeling tired all the time Risk Factors: • Genetics • Environment
. Signs of DKA include vomiting, sleepiness, fruity breath, difficulty breathing, and if untreated, coma and death. Symptoms: • Increased thirst. and urination. • Weight loss. • Blurred vision. • Feeling tired all. the time. Risk Factors: • Genetics. • Environment.")
36
Type 2 Diabetes Cells are insulin resistant and do not use insulin well. Children with Type 2 Diabetes often do not take insulin but may take a diabetes pill such as Metformin. Blood sugar monitoring, careful attention to a healthy diet, and daily exercise are important to controlling Type 2 Diabetes.

37
Risk Factors: Symptoms: Feeling tired all the time
Type 2 diabetes is the most common form of the disease. It can develop at any age, even during childhood. Type 2 diabetes is a progressive disease and usually begins with insulin resistance where muscle, liver, and fat cells do not use insulin effectively. The pancreas produces more insulin but eventually loses its ability to produce enough insulin to control the glucose levels. More children and adolescents in the United States have become overweight and sedentary in their activity level resulting in an increase of Type 2 diabetes occurring in this younger population. Risk Factors: Being overweight Having a family member who has type 2 diabetes Being African American, Hispanic/Latino, American Indian, Alaska Native, Asian American, or Pacific Islander including Native Hawaiian Symptoms: Feeling tired all the time Increased thirst and urination Weight loss Blurred vision Frequent infections Slow-healing wounds

38
Prevalence of Diabetes in Children is Increasing
200,000 or 1 in every 400 children and adolescents in the United States has Diabetes. According to recent estimates, about 19,000 youths are diagnosed with type 1 and type 2 diabetes each year.

39
Goals of Diabetic Management in Children
To promote normal childhood and adolescent growth and development. To promote healthy, emotional well- being. To maintain a balance between insulin, food and exercise.

40
Good Blood Glucose Control is a Balancing Act 24/7
Diabetes Research Research has shown that maintaining good control of blood sugar levels can prevent long-term complications of diabetes. Good Blood Glucose Control is a Balancing Act 24/7 INSULIN EXERCISE FOOD The goal of effective diabetic management is to keep the blood glucose levels in the “target range” which is determined by the student’s health care provider.

41
Diabetes management involves checking blood glucose levels throughout the day, following an individualized meal plan, getting regular physical activity, and administering insulin to try to maintain blood glucose levels in the target range and to prevent hypoglycemia or hyperglycemia. Hyperglycemia Hypoglycemia

42
Checking Blood Glucose Levels
Regular glucose monitoring is essential in good diabetic management. Blood glucose levels are most often done by poking the end of the finger with a lancet via a poking device and placing a drop of blood on a test strip which is inserted into a glucose meter where the meter displays the blood glucose level.

43
BLOOD GLUCOSE TESTING Students usually check their blood glucose:
Helpful information: Students should be allowed access to their diabetic testing equipment and supplies at all times Students experiencing hypoglycemia (low blood sugar) may need assistance in testing their blood glucose levels If low blood sugar is suspected, testing should be done in the tip of the finger Hands should be thoroughly washed and dried before testing Sharps and contaminated supplies must be disposed of according to district policy and students IHP Students usually check their blood glucose: As outlined in their Individual Health Plan (IHP) Before and after eating snacks and meals Before and after physical activity When they have symptoms of low or high blood glucose levels
 may need assistance in testing their blood glucose levels. If low blood sugar is suspected, testing should be done in the tip of the finger. Hands should be thoroughly washed and dried before testing. Sharps and contaminated supplies must be disposed of according to district policy and students IHP. Students usually check their blood glucose: As outlined in their Individual Health Plan (IHP) Before and after eating. snacks and meals. Before and after physical. activity. When they have symptoms of low or high blood glucose levels.")
44
HYPOGLYCEMIA Hypoglycemia, which is not always preventable, is the greatest immediate danger to students with diabetes Low blood sugar can develop within minutes and requires immediate attention Hypoglycemia usually can be treated easily and effectively. If it is not treated promptly, however, hypoglycemia can lead to loss of consciousness and seizures and can be life threatening Hypoglycemia means LOW blood sugar and is defined as a blood sugar less than 60 mg/d

45
Causes of Hypoglycemia
Too much insulin Missing or delaying meals or snacks Not eating enough food (carbohydrates) Getting extra, intense, or unplanned physical activity Being ill, particularly with gastrointestinal illness Hypoglycemia is most likely to occur before lunch, end of the school day or after PE/recess
 Getting extra, intense, or unplanned physical activity. Being ill, particularly with gastrointestinal illness. Hypoglycemia is most likely to occur before lunch, end of the school day or after PE/recess.")
46
Hypoglycemia Symptoms
Hypoglycemia can impair a student’s cognitive abilities and adversely affect academic performance. Sometimes, its symptoms are mistaken for misbehavior.

47
“I’m the Blood Sugar Fairy.
If you can see me, yours is too low.”

48
Mild to Moderate Hypoglycemia
Shaky or jittery Sweaty Hungry Pale Headache Blurry vision Sleepy Dizzy Confused Disoriented Uncoordinated Irritable or nervous Argumentative Combative Changed personality Changed behavior Inability to concentrate Weak Lethargic When hypoglycemia is suspected, always treat immediately as outlined in student’s Emergency Care Plan (ECP) Never leave a student unattended who is suspected of having hypoglycemia Never allow another student to escort a student suspected of having hypoglycemia Do not delay treatment, when in doubt always treat for hypoglycemia as symptoms may progress rapidly
 Never leave a student unattended who is suspected of having hypoglycemia. Never allow another student to escort a student suspected of having hypoglycemia. Do not delay treatment, when in doubt always treat for hypoglycemia as symptoms may progress rapidly.")
49
Treatment for Mild to Moderate Hypoglycemia: Requires immediate action
Give the student a quick-acting glucose (sugar) equivalent to 15 gm of carbohydrate: 3-4 glucose tabs 4 oz fruit juice 6 oz regular soda (1/2 can) 1 tube glucose gel Wait minutes and recheck blood glucose (BG) Repeat treatment if BG is below target range as indicated on student’s ECP Follow with snack of complex carbohydrate and protein if longer than 30 minutes until next meal. Treatment should follow guidelines outlined in student’s Emergency Care Plan (ECP) Notify school nurse at first sign of hypoglycemia Check blood sugar to determine low blood sugar Student safety is priority, when in doubt treat for hypoglycemia then continue procedures outlined in student’s ECP
 equivalent to 15 gm of carbohydrate: 3-4 glucose tabs. 4 oz fruit juice. 6 oz regular soda (1/2 can) 1 tube glucose gel. Wait minutes and recheck blood glucose (BG) Repeat treatment if BG is below target range as indicated on student’s ECP. Follow with snack of complex carbohydrate and protein if longer than 30 minutes until next meal. Treatment should follow guidelines outlined in student’s Emergency Care Plan (ECP) Notify school nurse at first sign of hypoglycemia. Check blood sugar to determine low blood sugar. Student safety is priority, when in doubt treat for hypoglycemia then continue procedures outlined in student’s ECP.")
50
Severe Hypoglycemia: Urgent Response necessary to treat life-threatening symptoms
Contact school nurse or initiate 911 if nurse if not immediately available Position student on side School RN to administer Glucagon per HCP orders Do not attempt to put anything in student’s mouth Notify parent Symptoms: Inability to eat or drink Unconsciousness Unresponsiveness Seizure activity or convulsions

51
Glucagon Call 911 when Glucagon is administered
Glucagon is hormone that raises blood sugar levels and is administered as an injection for the treatment of severe hypoglycemia Glucagon can only be administered by the school nurse or qualified Parent Designated Adult (PDA), glucagon cannot be delegated to non-licensed personnel Glucagon may cause nausea or vomiting once the student regains consciousness, student should be placed in a side-lying position to prevent choking Call 911 when Glucagon is administered Call 911 immediately if Glucagon is not prescribed or included in student’s ECP or if school nurse is not immediately available
, glucagon cannot be delegated to non-licensed personnel. Glucagon may cause nausea or vomiting once the student regains consciousness, student should be placed in a side-lying position to prevent choking. Call 911 when Glucagon is administered. Call 911 immediately if Glucagon is not prescribed or included in student’s ECP or if school nurse is not immediately available.")
52
Hyperglycemia Hyperglycemia means HIGH blood sugar and is defined as a blood sugar greater than 250 mg/dl Elevation in blood sugars in children are usually minimally above the target range and are short in duration, whereas older children may experience frequent spikes throughout the day in blood sugars that are high (above 250 mg/dl) and last longer in duration Short-term effects of hyperglycemia impact student’s cognition and academic performance Long-term effects of hyperglycemia result in serious health complications such as heart disease, kidney failure, stroke, blindness, and amputation
 and last longer in duration. Short-term effects of hyperglycemia impact student’s cognition and academic performance. Long-term effects of hyperglycemia result in serious health complications such as heart disease, kidney failure, stroke, blindness, and amputation.")
53
Causes of Hyperglycemia
Too little insulin or other glucose-lowering medications Too little food intake that has not been covered by insulin Decreased physical activity Illness, infection, injury, or severe physical or emotional stress The onset of hyperglycemia may occur over several hours or days

54
Hyperglycemia Symptoms
Increased thirst and/or dry mouth Frequent or increased urination Change in appetite Nausea Blurry vision Fatigue

55
Treatment for Hyperglycemia
Contact school nurse at first sign of hyperglycemia Check blood glucose levels to determine if blood sugar is above target range Encourage student to drink water or non-sugar beverage Allow for free and unrestricted access to water and restroom Modify physical activity in presence of ketones and according to student’s ECP Authorized staff to verify pump is connected and working properly if student wearing insulin pump Treatment should follow student’s Emergency Care Plan and may include: Insulin administration as prescribed Urine ketone testing Additional blood sugar monitoring Pump troubleshooting Non-licensed Personnel are limited to tasks delegated by the licensed school nurse in accordance to state nursing laws

56
Diabetic Ketoacidosis (DKA)
Diabetic ketoacidosis develops over hours to days and is associated with hyperglycemia, a buildup of ketones (ketosis) in the blood, and dehydration Caused by prolonged inefficient delivery of insulin, pump malfunction in delivery of insulin, illness, or prolonged physical or emotional stress Signs include severe abdominal pain with vomiting, dry mouth and extreme thirst, fruity breath, heavy breathing and shortness of breath, chest pain, increasing sleepiness or lethargy, and decreased level of consciousness Contact school nurse or 911 if nurse is not immediately available
 in the blood, and dehydration. Caused by prolonged inefficient delivery of insulin, pump malfunction in delivery of insulin, illness, or prolonged physical or emotional stress. Signs include severe abdominal pain with vomiting, dry mouth and extreme thirst, fruity breath, heavy breathing and shortness of breath, chest pain, increasing sleepiness or lethargy, and decreased level of consciousness. Contact school nurse or 911 if nurse is not immediately available.")
57
Insulin Insulin has three characteristics
Insulin is classified in four types by how it works: Rapid-acting Short-acting Intermediate-acting Long-acting Insulin has three characteristics Onset of effect – the length of time insulin reaches the bloodstream and starts lower blood glucose levels Peak time of effect – time insulin is at its maximum effect in lower blood glucose levels Duration of effect - number of hours insulin actively lowers blood glucose levels Improvements in the types of insulin and delivery systems help keep blood glucose levels within the target range, however, this means more frequent blood glucose monitoring and greater need for student assistance in diabetic management

58
Insulin Administration
Schedule for blood sugar testing, insulin administration, and level of student independence is detailed in the student’s Individual Health Plan (IHP) according to physician orders. This may include a plan to take insulin to cover meals and/or snacks, the need for additional or corrective dosages of insulin to treat hyperglycemia, and a plan to cover a rise in blood glucose levels VIDEO LINK:
 according to physician orders. This may include a plan to take insulin to cover meals and/or snacks, the need for additional or corrective dosages of insulin to treat hyperglycemia, and a plan to cover a rise in blood glucose levels. VIDEO LINK: v=SmSWCGJEUG8&feature=share&list=PL3DE9DDE8EB2A2E56.")
59
Insulin Delivery Three most common ways to administer insulin:
Insulin syringe – syringe is used to draw up prescribed amount of insulin out of vial Insulin pen – pen holds a cartridge of insulin, needle tip is screwed onto tip of pen, desired insulin dosage is dialed up Insulin pump – small computerized device which delivers a set amount of insulin 24 hours a day directly into the student’s skin

60
Insulin-to-carb ratio for meals
Carbohydrate (carb) counting is the most popular meal planning approach for children and youth - the number of grams of carbohydrate, or choices of carbohydrate, the student eats is calculated (one carb choice equals 15 grams of carbohydrate) Insulin-to-carb ratio - determines the number of units of insulin needed to cover the number of grams of carbs to be eaten The blood glucose correction factor (insulin sensitivity factor)—determines the amount of insulin needed to lower blood glucose to target level. This additional insulin may be needed if blood sugar is elevated above target level prior to meal or snack
 counting is the most popular meal planning approach for children and youth - the number of grams of carbohydrate, or choices of carbohydrate, the student eats is calculated (one carb choice equals 15 grams of carbohydrate) Insulin-to-carb ratio - determines the number of units of insulin needed to cover the number of grams of carbs to be eaten. The blood glucose correction factor (insulin sensitivity factor)—determines the amount of insulin needed to lower blood glucose to target level. This additional insulin may be needed if blood sugar is elevated above target level prior to meal or snack.")
61
Example of HCP order Insulin-to- carb ratio - 1:10 Correction ratio -
1:50 Sensitivity – 50 mg/dl Target BS - 120 mg/dl

62
Parent Designated Adult (PDA)
A Parent Designated Adult (PDA) is a volunteer, who may be a school district employee who receives additional training from a healthcare professional or expert in diabetic care selected by the parent and who provides care for the child consistent with the individual health plan. Written documentation of intent to be a PDA along with ongoing training documentation required to be submitted to district Must attend district training for direct care (IHP) Additional training requirements if PDA is a school employee School nurse is not responsible for the training, supervision, or actions of a PDA
 is a volunteer, who may be a school district employee who receives additional training from a healthcare professional or expert in diabetic care selected by the parent and who provides care for the child consistent with the individual health plan. Written documentation of intent to be a PDA along with ongoing training documentation required to be submitted to district. Must attend district training for direct care (IHP) Additional training requirements if PDA is a school employee. School nurse is not responsible for the training, supervision, or actions of a PDA.")
63
Personnel Guidelines for Care of Students with Diabetes in School
Verify number on insulin pen for student independent in management of self- injecting Verify number on glucose meter for student independent in the management of his/her self-monitoring Ketone urine testing per physician order Treatment of mild and moderate hypoglycemia, initiation of 911 for severe hypoglycemia Administration of snacks as needed Delegation of responsibilities to unlicensed staff by the licensed staff R.N. is in accordance with statute, regulation, Nursing Care Quality Assurance Commission guidelines, nurse practice act , and best practice. All other responsibilities and tasks require nursing judgment and cannot be delegated.

64
Diabetes affects the entire family
Night Visits The minutes tick by I watch the clock, can't sleep It strikes midnight and into your room I creep. Not for a tuck in or even a drink, but to test your blood sugar while you sleep. Your sweet little face, your "Barrie" held tight, these awful visits in the night. I hate this diabetes it won't go away! Please God let her numbers be good today. One test down, thousands to go, I need to be strong for her I love her so. Written by Pam Bushway in 2005 for her 6 year-old child

65
THE LAW AND DIABETES Diabetes is considered a disability under federal law. Under Section 504 of the Rehabilitation Act of 1973, it is illegal to discriminate against a person with a disability. Children with diabetes must have full access to all activities, services, or benefits provided by public schools. Any school receiving federal funds must accommodate the special healthcare needs of students with disabilities in order to provide them with “free appropriate public education.” These accommodations are developed with parent consent and may be reflected in the student’s Individual Health Plan (IHP)/504 Plan or as part of the student’s individualized education program (IEP) if student qualifies for special education services.
/504 Plan or as part of the student’s individualized education program (IEP) if student qualifies for special education services.")
66
Common accommodations for students with Diabetes
Eligibility and accommodations are determined through district process, either by the Guidance Team or team of members coordinating 504 plans or by coordinated efforts of the school nurse through the Professional Education Group for students qualifying for specialized education. The parent is involved in the team process in developing appropriate accommodations. Free access to testing equipment and supplies with ability to test and treat as needed without restriction according to DMMP and IHP Free and liberal access to food Free and liberal access to water or non-sugar drinks, as well as access to restroom Meals must never be withheld for nonpayment of fees or disciplinary action Access to fully participate in physical education and team sports in accordance to DMMP and ECP Participation in school-sponsored field trips and extracurricular activities without restriction, including supervision by school personnel at outlined in DMMP and IHP Extra time to complete tests or work without penalty when related to high or low blood glucose levels Extra time to complete missed work without penalty when due to absences related to diabetic care

67
Washington State Law, SHB 2834, now requires that the necessary order, medications, equipment, and nursing plan must be in place before a student with a life-threatening condition may attend school. Registrars, Head Secretaries and Office Staff play a key role in identifying students with life-threatening health conditions before they begin their first day of school. Any student indicating a life-threatening health condition on the enrollment health history form must meet with the school nurse to coordinate a treatment plan before the student may attend school.

68
The statue adds the requirement that every student with diabetes has an Individualized Health Plan
School district, school district employee, agent, or parent- designated adult who, acting in good faith and in substantial compliance with the student’s individual health plan and the instructions of the student’s licensed health care professional, provides assistance or services under RCW 28A shall not be liable in any criminal action or for civil damages in his or her individual or marital or governmental or corporate or other capacities as a result of the services provided under RCW 28A to students with diabetes. Diabetic Medical Management Plan (DMMP) includes the health care provider orders for all aspects of student’s routine and care The school nurse uses the DMMP for developing the student’s Individual Health Plan (IHP) which details the specific care for the student as outlined by the physician. In many cases, the IHP and 504 are the same document The Emergency Care Plan (ECP) is created by the school nurse from the IHP and describes emergency treatment for the treatment of hypoglycemia and hyperglycemia for the student
 includes the health care provider orders for all aspects of student’s routine and care. The school nurse uses the DMMP for developing the student’s Individual Health Plan (IHP) which details the specific care for the student as outlined by the physician. In many cases, the IHP and 504 are the same document. The Emergency Care Plan (ECP) is created by the school nurse from the IHP and describes emergency treatment for the treatment of hypoglycemia and hyperglycemia for the student.")
69
Example of required medical documentation required for school attendance (Seattle Children’s DMMP with HCP orders)
")
70
Seattle Children’s DMMP – Parent form
Information from the DMMP, along with parent and student input is essential for the school nurse in developing student’s IHP and ECP Students who fail to provide the required physician orders and emergency medication are subject to exclusion from school (SHB 2834)
")
71
IHP in Skyward IHP in Skyward

72
Emergency Care Plan (ECP)
")
73
Useful Tips Become familiar with students in your building who have life- threatening conditions – look up their pictures on Skyward Never leave a student with diabetes unattended in the health room Become familiar with the IHP and ECP of students in your building who have life-threatening health conditions, know where emergency medication is stored according to Perform only those duties which you have been delegated Consult the school nurse in your building for concerns or questions, contact a district nurse if the nurse assigned to your building is unavailable

74
Diabetes Q/A

75
Seizure Participants will:
1. Identify signs and symptoms of types of seizures. 2. Understand how to respond to a student having a seizure and the appropriate emergency procedures. Always refer to individual student care plan

97
Seizure Medication

98
Seizure: Scenario 1 How do you respond?
Called to classroom for a student who appears to be having a grand mal (tonic- clonic) seizure. Student does not have a known seizure disorder. How do you respond?
 seizure. Student does not have a known seizure disorder. How do you respond")
99
Seizure: Scenario 1 Questions? Response:
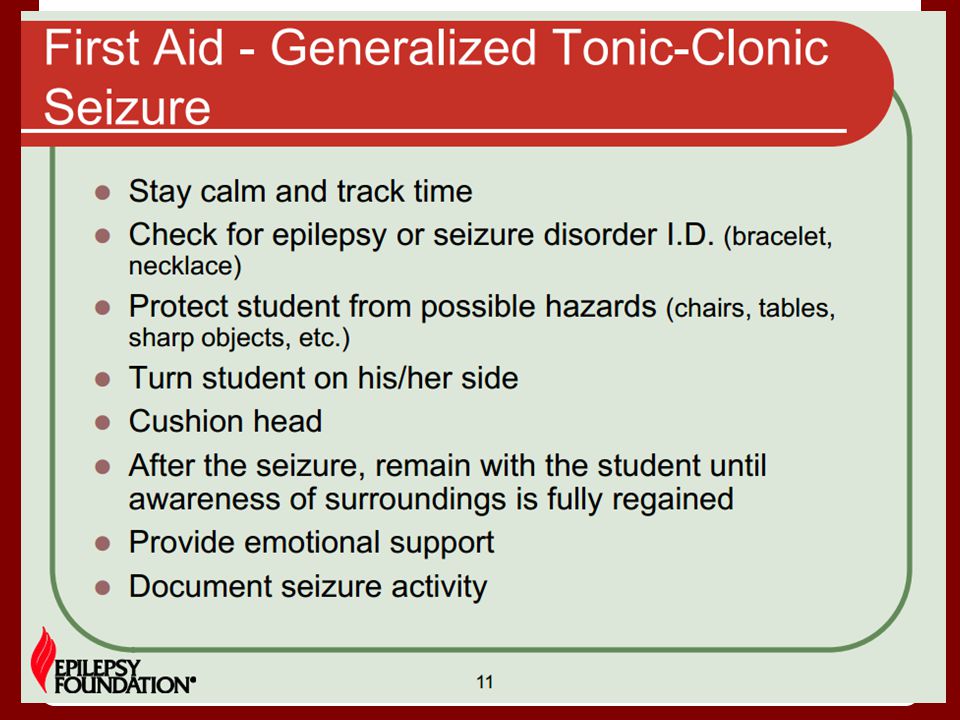
Call this is a first time seizure for a student without a seizure disorder diagnosis. Ensure student's safety. Protect student's head. Assist student to side lying position. Time the seizure. Questions?

100
Seizure: Scenario 2 How do you respond?
Called to a classroom for student with a known seizure disorder who is having grand mal (tonic- clonic) seizure. How do you respond?
 seizure. How do you respond")
101
Seizure: Scenario 2 Questions? Response: Ensure student's safety.
Protect student's head. Assist student to side lying position. Time the seizure. If the seizure lasts longer then 5 minutes call 911. Stay with the student until they regain consciousness. Provide emotional support. Allow student to rest. Notify parents. Document seizure. Questions?

102
Always refer to individual student care plan
Cardiac Participants will understand that: 1. Cardiac arrest can happen to anyone (e.g., student, parent, co-worker, visitor, etc.). 2. Cardiac arrest is not always associated with sports. 3. Sometimes the person doesn't know they have symptoms or won’t admit them if they do. 4. Cardiac arrest can happen at anytime without warning. Always refer to individual student care plan
. 2. Cardiac arrest is not always associated with sports. 3. Sometimes the person doesn t know they have symptoms or won’t admit them if they do. 4. Cardiac arrest can happen at anytime without warning. Always refer to individual student care plan.")
103
Understanding Sudden Cardiac Arrest
Project ADAM... Understanding Sudden Cardiac Arrest The mission of Project ADAM is to serve children and adolescents through education and deployment of life- saving programs that help prevent sudden cardiac arrest. Project ADAM helps schools across the nation implement public access defibrillation programs through support and education.

104
Understanding Sudden Cardiac Arrest
Project ADAM... Understanding Sudden Cardiac Arrest

105
CPR/AED Participants will:
1. Recognize the symptoms of cardiac arrest. 2. Know how to check the person’s airway, breathing, and circulation. 3. Know when to start CPR and call 911.

106
CPR/AED It is your responsibility to keep your CPR/AED & First Aid certification up to date - renew every 2 years. Know where your AEDs are in your building. WHEN IN DOUBT CALL 911

107
Asthma Participants will: 1. Identify signs and symptoms of asthma.
2. Understand how to administer inhaler and/or with spacer. 3. Identify an asthma emergency and how to respond. Always refer to individual student care plan

108
Source: National Asthma Education and Prevention Program (NAEPP)
")
109
Source: National Asthma Education and Prevention Program (NAEPP)
")
110
Source: National Asthma Education and Prevention Program (NAEPP)
")
111
Source: National Asthma Education and Prevention Program (NAEPP)
")
112
Source: National Asthma Education and Prevention Program (NAEPP)
")
113
Source: National Asthma Education and Prevention Program (NAEPP)
")
114
Source: National Asthma Education and Prevention Program (NAEPP)
")
115
Source: National Asthma Education and Prevention Program (NAEPP)
")
116
Source: National Asthma Education and Prevention Program (NAEPP)
")
117
Source: National Asthma Education and Prevention Program (NAEPP)
")
118
Source: National Asthma Education and Prevention Program (NAEPP)
")
119
Source: National Asthma Education and Prevention Program (NAEPP)
")
120
Source: National Asthma Education and Prevention Program (NAEPP)
")
121
Source: National Asthma Education and Prevention Program (NAEPP)
")
122
Source: National Asthma Education and Prevention Program (NAEPP)
")
123
Source: National Asthma Education and Prevention Program (NAEPP)
")
124
Source: National Asthma Education and Prevention Program (NAEPP)
")
125
Source: National Asthma Education and Prevention Program (NAEPP)
")
126
Asthma Emergency Plan Call 911 if you see ANY ONE of the following
emergency signs: *Trouble walking or talking without stopping to breathe * Child is hunched over *Child is struggling to breathe *Lips or fingernails are gray or blue *Cough

127
Asthma Emergency Plan continued
*Tightness in chest, or tickle in throat * Shortness of breath * Wheeze *Unable to catch their breath-Gasping, *Rapid breaths *Nostrils flaring *Feelings of fear or confusion After calling 911, call the office and tell them to contact a parent or guardian.*

128
Source: National Asthma Education and Prevention Program (NAEPP)
")
129
Asthma: Scenario 1 How do you respond?
Student walks into Health Room. Student says they feel "tight" and would like to use their inhaler. They do not appear to be in distress and are able to speak to you. Student says they last used their inhaler before school. It is now 1pm. How do you respond?

130
Asthma: Scenario 1 Questions? Response:
Student has a medication order and an inhaler in the Health Room. Verify time of last inhaler administration - Call parents if needed. Following appropriate medication administration protocol - administer inhaler. Document medication administration and health office visit. If you did not need to call parents to verify when inhaler was last used - notify parents of inhaler use, as appropriate. Questions?

131
Asthma: Scenario 2 How do you respond?
Called to cafeteria for a student who is having an asthma attack, they are unable to walk to the Health Office. Student unable to talk/ speak because of poor air movement. Lips blue. How do you respond?

132
Asthma: Scenario 2 Questions? Response:
Call It is better to have too much help then not enough. Student has an inhaler in the Health Room. Stay with the student. Have another staff member obtain the inhaler. Administer the inhaler, using appropriate medication administration protocol. If the student improves - GREAT! Call parents. Medics will evaluate the student on their arrival and make appropriate determination. If student does not improve - Medics will assume responsibility for student's care. Questions?

133
Anaphylaxis & Life Threatening Food Allergies
Participants will: 1. Identify signs and symptoms of an allergic reaction and anaphylaxis 2. Be able to initiate treatment for an allergic reaction Always refer to individual student care plan

134
Anaphylaxis Prevent a Severe Food Allergy
Reaction:Follow the FAST Formula FACTS about Food Allergies *Food allergy reactions can be triggered by a tiny trace of allergen *A food allergy reaction can cause death within minutes *Children with asthma are at the highest risk of dying *know every child's emergency treatment plan AVOID the Allergen *Read food ingredient labels *Clean tables, desks and other surfaces *Wash hands often *check ingredients of art supplies and personal care products

135
Anaphylaxis SIGNS and Symptoms
*Itching of the mouth, swelling of lips and/or tongue *Tightness of the throat and hoarseness *Shortness of breath, coughing, wheezing *Vomiting, diarrhea, cramps *Weak pulse, dizziness, fainting *Symptoms vary and can change quickly TREAT immediately * Give epinephrine-do not delay! *Call and request that a paramedic respond *Call emergency contacts

136
Anaphylaxis

137
Anaphylaxis

138
Anaphylaxis

139
Anaphylaxis

140
Anaphylaxis

141
Anaphylaxis

142
Anaphylaxis

143
Anaphylaxis

144
Anaphylaxis

145
Anaphylaxis

146
Anaphylaxis

147
Anaphylaxis

148
Anaphylaxis

149
Anaphylaxis

150
Anaphylaxis

151
Anaphylaxis

152
Anaphylaxis

153
Anaphylaxis

154
Anaphylaxis

155
Anaphylaxis

156
Anaphylaxis

157
Anaphylaxis

158
Anaphylaxis: Administering Epi-Pen

159
Anaphylaxis: Administering Epi-Pen
Auvi-Q

160
Anaphylaxis: Scenario
Student comes to Health Room complaining of tingling, scratchy throat, hacking cough, upset stomach/ nausea, saying they don't feel right after eating lunch at school. They say they traded their chips for their friend's cookies How do you respond?

161
Anaphylaxis: Scenario
Response: Student has a known allergy to peanuts. They have an epi-pen at school and school care plan on file. Administer epi-pen per medication administration policy. Call 911. Call parents. Remain with student until medics arrive. When medics arrive they will assume care for the student. Questions?

162
911 Emergency Procedures Participants will:
1. Understand procedures and roles when calling 911.

163
Calling 911 / Procedures When to call? Who calls?
Who is immediately notified? Who else in the district is called? What paperwork to fill out?

164
When to call 911 Call 911 for medical emergencies:
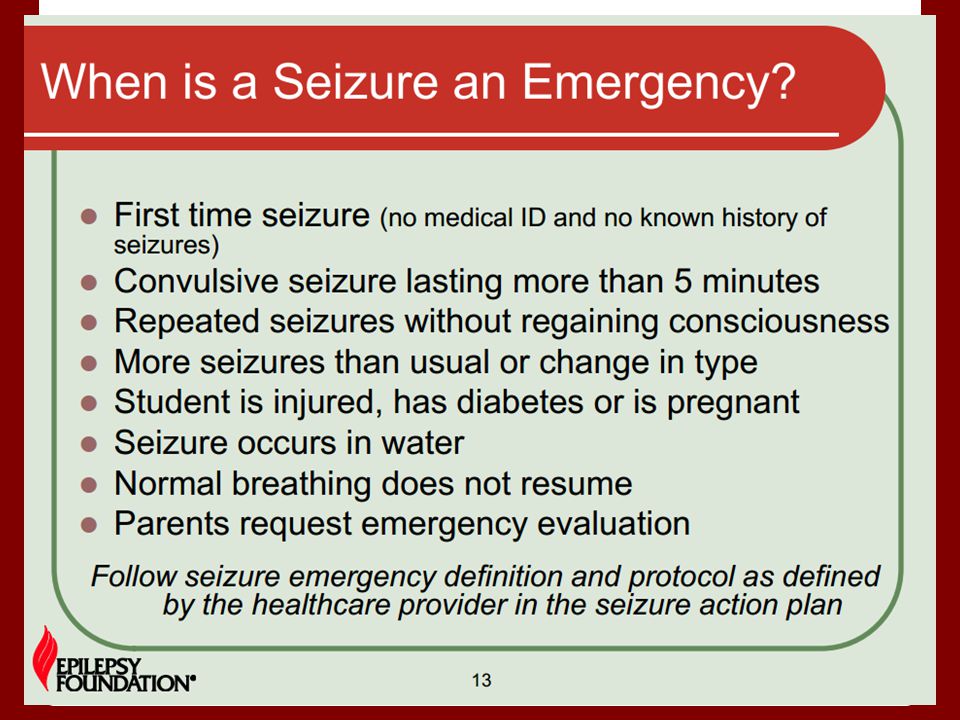
Severe allergic reaction (anaphylaxis) Choking or severe difficulty breathing Shock Deep wound or part of the body that was crushed Bleeding that is difficult to control Back and neck injuries or broken bones Severe head injury Unconsciousness Seizure - if longer than three to five minutes, if there is a second seizure, or if the student has never had a seizure before Serious burns Spill or release of hazardous chemicals Several students injured or ill at the same time
 Choking or severe difficulty breathing. Shock. Deep wound or part of the body that was crushed. Bleeding that is difficult to control. Back and neck injuries or broken bones. Severe head injury. Unconsciousness. Seizure - if longer than three to five minutes, if there is a second seizure, or if the student has never had a seizure before. Serious burns. Spill or release of hazardous chemicals. Several students injured or ill at the same time.")
165
Calling 911 / Procedures CALL AID CAR WHEN:
A student’s health could be compromised. When in doubt, call anyway. It is better to have too much help than not enough. A student is experiencing breathing difficulties, severe bleeding, seizures, severe bee sting reactions, possible broken bones, and/or is unconscious. PROCEDURE WHEN CALLING AN AID CAR: Someone should stay with student at all times while at school. Do not move student. Provide safe environment. Cover with blanket if needed. Clear area of all other students. A designated person in office calls: 911 School RN (if not in building) Parents Teacher Principal Information needed for 911 team: Copy of locator card. Check Health Concerns list for additional health problems that the student may have. Once the AID care arrives, the 911 team is responsible for the student. DO NOT sign any forms or waivers provided by the 911 team.
 Parents. Teacher. Principal. Information needed for 911 team: Copy of locator card. Check Health Concerns list for additional health problems that the student may have. Once the AID care arrives, the 911 team is responsible for the student. DO NOT sign any forms or waivers provided by the 911 team.")
166
Calling 911 / Procedures IMPORTANT REMINDERS:
DO NOT accompany student in AID car. Do not make any treatment decisions at the hospital or doctor’s office. DOCUMENT: Fill out the Incident Report Form Fill out 911 Emergency Medical Notification Checklist FOLLOW UP Call ESC switchboard to report 911 call Complete accident report and send original to Teresa Main at ESC Keep copy at building

167
Incident & Emergency Procedures
Participants will: 1. Become familiar with district procedures and forms.

168
How to Respond Know where this resource is in your health room.
Source: WA DOH

169
Head Bumps EVERY head bump.... Needs a head bump form filled out,
no matter how minor it seems. 2. Call Parent/Guardian

170
Concussion L ink from Carrie M.
Concussion in sporting event and impact for schools.

171
Concussion

172
Incident: Student/ Non-Employee Injury
Revised 7/2013 Incident: Student/ Non-Employee Injury In google drive for all LSSD Staff

173
Confidentiality Skyward & Participants will:
1. Will understand their role using the health module in Skyward. 2. Will understand the obligation to maintain student health information confidential.

174
Skyward: Health Room/Documentation
Multiple windows - have one for health and one for office work. Automatically dates, times and signs who entered what information. You are responsible for what you write - so don't let others write under your log in. Write enough so that you know what happened. TOAD - what they told you, what you saw (observed), what action you took, disposition (where'd they go) Reminder for communication best practice: - RN needs to know about incident reports, head bumps and any critical student/staff concerns. - Call parent/guardian with important information about their student
, what action you took, disposition (where d they go) Reminder for communication best practice: - RN needs to know about incident reports, head bumps. and any critical student/staff concerns. - Call parent/guardian with important information about. their student.")
175
Confidentiality All unlicensed health care providers, such as health room aides or pupil transportation staff who assist the health care provider in the delivery of health care to students, must be informed of the confidentiality requirements of the Federal Family Education Rights and Privacy Act (FERPA) and state requirements under chapter RCW, Medical Records - Health Care Information Access and Disclosure. Health care information about a student cannot be disclosed without signed consent of parent, guardian, or student except in selected situations identified by the licensed health care provider (such as the nurse). Everything that happens in the health room, stays in the health room!!!!
 and state requirements under chapter RCW, Medical Records - Health Care Information Access and Disclosure. Health care information about a student cannot be disclosed without signed consent of parent, guardian, or student except in selected situations identified by the licensed health care provider (such as the nurse). Everything that happens in the health room, stays in the health room!!!!")
176
Lice Participants will: 1. Recognize head lice.
2. Understand head lice district procedures. 3. Identify information available to assist parents with treatment.

178
Head Lice Procedures Each fall, there will be an elementary school-wide lice screening by designated employees. New students will be screened prior to starting school. Students are screened throughout the year on teacher/parent referrals.

179
Head Lice Procedures Students with nits/head lice are sent home for treatment. Students are checked by school personnel prior to readmission to school. Students are only readmitted to school if free of live lice.

180
Head Lice Procedures Students are re-examined one week after re-admission. At the school nurse’s discretion, classrooms will be re-screened by designated personnel as needed throughout the school year. Classrooms will receive a general letter regarding head lice as deemed necessary by the school nurse.

181
Head Lice Recognition

182
Thank you for joining us today and your commitment to keep kids safe.

Similar presentations



























 has developed standardized medication training, each district.>")








