Download presentation
Presentation is loading. Please wait.

1
CERVICAL CANCER... Diagnosis & Treatment

3
CERVICAL CANCER... The most common malignancy in gynecological oncology Incidence: 7.8/100,000 Mortality: 2.7/100,000 Diagnosis: biopsy Main modality of treatment: surgery and radiation Goal of treatment: cure, except stage 4b

4
Special Case 38 yrs, G3/P1, nurse
C/O: postcoital bleeding for 2 months Menstruation regular with 30 days cycle and 5 days duration. Abnormal discharge with bad smell. LMP: 12 days ago Pap smear: squamous cell cancer PV: Vulva : Normal, Vaginal: yellowish discharge with bloody stained, Cervix: growth with ulceration and contact bleeding. Uterus: N/S, mobile. Parametrium: thickening not to pelvic sidewall on both side

5
CERVICAL CANCER….. How can we make a diagnosis?
How can we evaluate the patient? How can we manage the patient? How should we explain to the patient? Can we prevent cervical cancer?

6
How can we make a diagnosis?
SYMPTOMS Abnormal vaginal bleeding postcoital bleeding* contact bleeding Abnormal vaginal discharge Asymptomatic, just abnormal pap smear

7
SYMPTOMS The classic symptom is intermittent, painless metrorragia or spotting only postcoitally or after douching. Probably the first symptom of early cancer of the cervix is a thin, watery, blood-tinged vaginal discharge that frequently goes unrecognized by the patients. As the maligancy enlarges, the bleeding episodes become heavier and more frequent, and they last longer.

8
SYMPTOMS Late symptom or indicators of more advanced disease include the development of pain referred to the flank or leg. Many patients c/o dysuria, hematuria or rectal bleeding or obstipation resulting from bladder or rectal invasion. Distant metastasis and persistent edema of one or both lower extremities as a result of lymphatic and venous blockage by extensive pelvic wall disease are late manifestation of primary disease and frequent manifestations of recurrent disease.

9
How can we make a diagnosis?
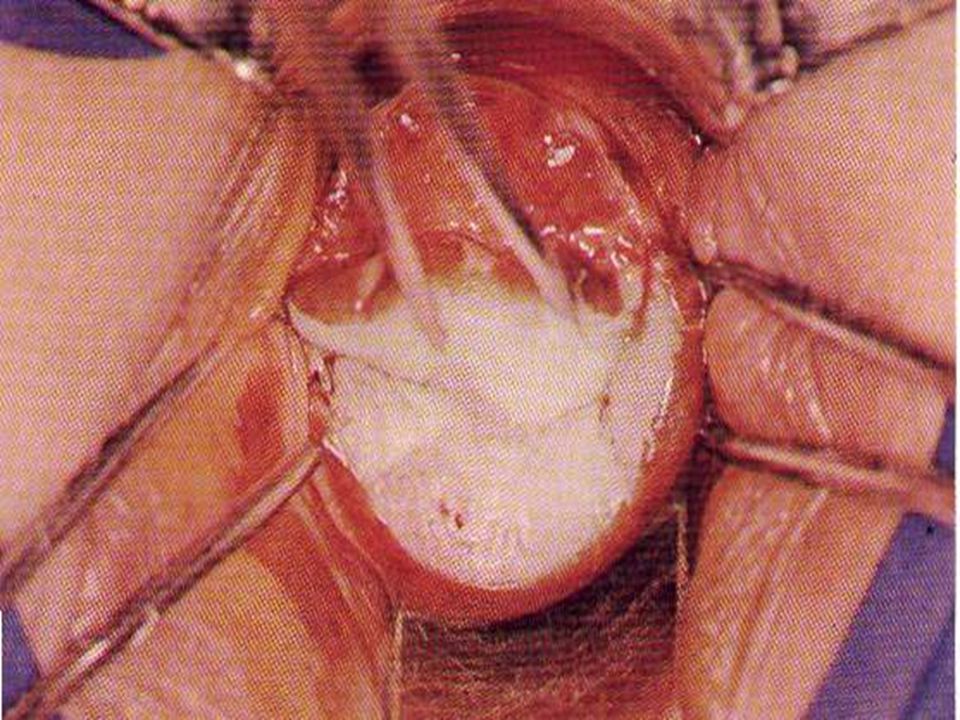
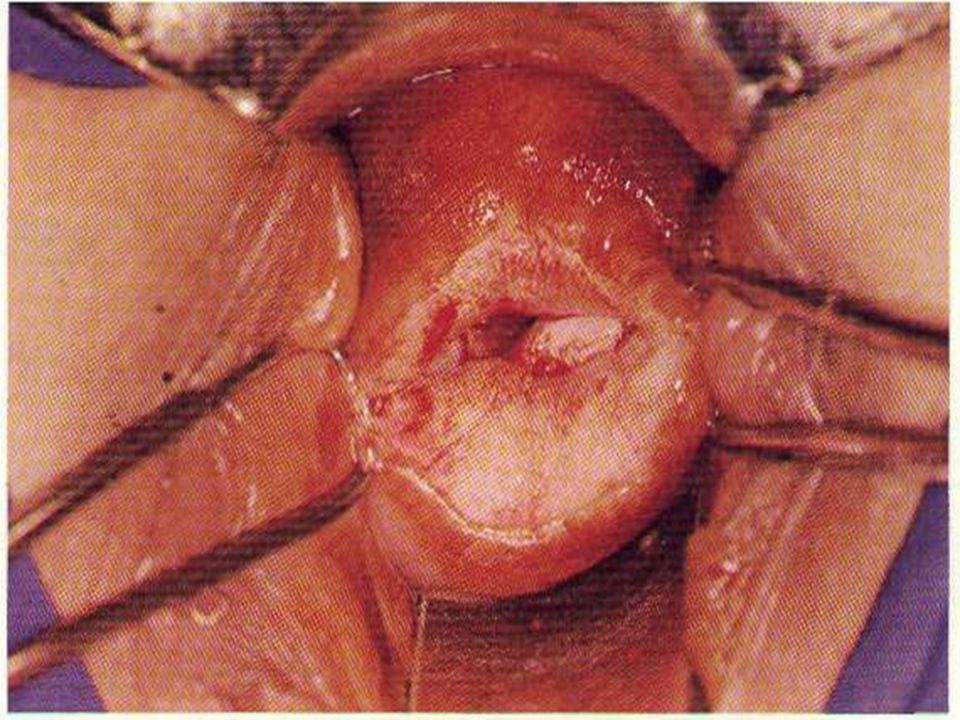
SIGNS Vagina: mucous, fornix Cervix: erosion growth ulceration barrel-shaped Uterus: size, mobility Paramet: thickening

10
Gross appearence Three categories of gross lesions have traditionally been described. The most common is the exophytic lesion, which usually arises on the ectocervix and ofter grows to form a large, friable,polypoid mass, arises on the endocervical canal, creating barrel-shaped lesion. Little visible ulceration or exophytic mass like a stone-hard cervix that regresses slowly with radiation therapy. Ulcerative tumor,usually erodes a portion of the cervix or replacing the cervix , erodes a portion of the upper vaginal vault with a large crate.

15
How can we make a diagnosis?
CLINICAL TESTS: Pap smear Colposcopy and target biopsy Endocervical curettage (ECC) Cone biopsy Biopsy
 Cone biopsy. Biopsy.")
16
Pap smear Pap smear is the most common and effective screening method.
Exfoliated cervical cells are scraped from the cervix by spatula. The entire T zone must be sampled. Incomplete sampling could produce a false-negative smear. The endocervical canal is also sampled with a swab or cytobrush. Cells are fixed immediately to avoid air-drying cytologic artifacts

17
Pap Smear Show Squamous Cell Carcinoma

18
Colposcopy and directed biopsy
A pap smear is only a screening test. A definitive diagnosis requires inspection of a well-visualized cervix with a colposcope. The cervix is painted with 3% acetic acid solution to enhance surface alterations and vascular changes. The colposcope evaluation is considered adequate or satisfactory if the complete T zone and full extent of the lesions is visualized. Areas of abnormality(e.g., White epithelium, mosaicism, and punctation) are selectively punch biopsied.
 are selectively punch biopsied.")
19
Colposcopy Examination

20
Cone biopsy Indications for cone biopsy
1.The lesion cannot be fully visualized . 2.The ECC is positive 3.There is significant discrepancy between the Pap smear and biopsy. 4.A biopsy reveals microinvasive squamous cell carcinoma 5.A biopsy reveals adenocarcinoma in situ

23
How can we make a diagnosis?
A pap smear is only a screening test! Definitive diagnosis of cervical cancer requires a BIOPSY!

24
How can we evaluate the patient?
Histologic type: Squmous cell carcinoma ( SCC) 80% Adenocacinoma %-15% Others %-10%
 80% Adenocacinoma 10%-15% Others 5%-10%")
25
Routes of spread Into the vaginal mucosa, extending microscopically down beyond visible or palpable disease; Into the myometrium of the low uterine segment and corpus, particularlly with lesions arising from the endocervix. Into the paracervical lymphatics and from there to the most common involved lymph nodes ( the obturator; hypogastric, and external iliac nodes). Direct extending into adjacent structures or parametria, reaching to the obturator fascia and the wall of the true pelvis
. Direct extending into adjacent structures or parametria, reaching to the obturator fascia and the wall of the true pelvis.")
26
How can we evaluate the patient?
Stage: Pelvic examination, Rectovaginal examination, Intravenous pyelography(IVP) Ultrasonography or CT Staging is clinical, but can use IVP and CT Cervical cancer is the only gynecologic malignancy that is not surgically staged
 Ultrasonography or CT. Staging is clinical, but can use IVP and CT. Cervical cancer is the only gynecologic malignancy that is not surgically staged.")
27
Clinical Staging for Cervical Carcinoma
Stage 0 Carcinoma in-situ; Confined to the epithelium only

28
Clinical Staging for Cervical Carcinoma
Stage I Invasion is strictly confined to the cervix Ia: Invasive cancer identified only microscopically . Ia1: Minimal microscopically evident stromal invasion <=3mm in depth and no wider than 7mm. Ia2: Microscopic invasion <=5mm in depth and no wider than 7mm

29
Clinical Staging for Cervical Carcinoma
Stage I Invasion is strictly confined to the cervix IB: All others preclinical lesions and clinical lesions confined to the cervix. Ib1: Clinical lisions no greater than 4 cm. Ib2: Clinical lisions greater than 4 cm.

30
Clinical Staging for Cervical Carcinoma
Stage II Invasion is beyond the cervix but not to the pelvic wall or lower third of the vagina IIA Parametria is not involved IIB Parametria is involved

31
Clinical Staging for Cervical Carcinoma
Stage III Invasion is to the pelvic wall or lower third of vagina IIIA Pelvic wall is not involved IIIB Pelvic wall is involved; hydronephrosis or nonfunctioning of the kidney may occur because of tumor

32
Clinical Staging for Cervical Carcinoma
Stage IV Invasion is beyond to the true pelvis or to the mucosa of the bladder or rectum. IVA Spread is to adjacent organs IVB Spread is to distant organs

33
How can we evaluate the patient?
Age: treatment vary with the patient’s age Marriage statue Reproductive history:menstrual, contraceptive, Gynecologic, Obstetric Social history: sexually activity, social statue Family history: children, partner,parents Past medical history

34
How can we evaluate the patient?
General condition: pulmonary (Chest-x-ray) cardiac function (ECG) liver function renal function Special disorders: bleeding diseases, diabetes mellitus, and infection
 cardiac function (ECG) liver function renal function. Special disorders: bleeding diseases, diabetes mellitus, and infection.")
35
How can we manage the patient?
Management of premalignant lesions: make definitive diagnosis selection of an appropriate mode of therapy carbon dioxide laser cryotherapy electrocautery loop electrodiathermy excision procedure (LEEP) Conization hysterectomy
 5. Conization 6. hysterectomy.")
36
How can we manage the patient?
Cervical Intraepithelial Neoplasia(CIN) For CIN I-II: observation(only for CIN I), carbon dioxide laser cryotherapy electrocautery loop electrdiathermy excision procedure (LEEP)
 For CIN I-II: observation(only for CIN I), carbon dioxide laser cryotherapy electrocautery loop electrdiathermy excision procedure (LEEP)")
37
How can we manage the patient?
Cervical Intraepithelial Neoplasia (CIN) For CIN III or CIS: conization: cold knife carbon dioxide laser diathermy and LEEP simple hysterectomy
 For CIN III or CIS: conization: cold knife carbon dioxide laser diathermy and LEEP simple hysterectomy.")
38
How can we manage the patient?
For invasive cancer: Simple hysterectomy (Ia1) Modified radical hysterectomy (Ia2) Radical hysterectomy and RPND (Ib-IIa) Radiotherapy (any stage, IIb III IV) 5 Chemotherapy
 2 Modified radical hysterectomy (Ia2) 3 Radical hysterectomy and RPND (Ib-IIa) 4 Radiotherapy (any stage, IIb III IV) 5 Chemotherapy.")
39
CERVICAL CANCER... Prognosis: % five-year survival (all stage combined) stage I % stage II % stage III % stage IV %

40
How can we prevent cervical cancer?
Risk factors Education Screening program Treatment of premalignant lesions

41
How can we prevent cervical cancer?
RISK FACTORS: early age of sexual intercourse multiple sexual partners low socioeconomic classes early age of pregnancy high parity cigarette smoking HPV (16,18) immunocompromised host
 immunocompromised host.")
42
How can we prevent cervical cancer?
EDUCATION: Population education Medical staff education

43
How can we prevent cervical cancer?
SCREENING: committee program: onset of screening, duration, end of screening methods for screening pap smear, CCT, thin-rep, HPV typing

44
Case discussion 27 yrs, G0/P0, married for 2 yrs
C/O: one episode of postcoital bleeding for 2 weeks Menstruation regular with 30 days cycle and 5 days duration No abnormal discharge. LMP: 2 weeks ago Pap smear: LSIL with HPV infection, clue cell > 50% PV: Vulva and vaginal: normal Cervix: erosion with contact bleeding,Uterus: N/S, mobile. Parametrium: clear Wants to preserve her reproductive function

45
Treatment strategy for CIN

46
Case discussion 48 yrs, G3/P1, midlife
C/O: postcoital bleeding for 4 months Menstruation irregular with days cycle and 5-20 days duration Abnormal discharge with bad smell. LMP: 2 months ago Pap smear: squamous cell cancer PV: Vulva : Normal, vaginal: right fornix involved by cervical growth. Cervix: growth with ulceration and contact bleeding.Uterus: N/S, mobile. Parametrium: nodular thickening to pelvic sidewall on right Biopsy:SCC. IVP:nonfunctional kidney

47
Treatment strategy for Invasive Cervical Cancer

48
How can we explain to the patient?
What is cervical cancer? How many treatment modes for cervical cancer ? Why we choose surgery or RT for the patient? What is the side-effect of the treatment? What is the prognosis and survival rate?

49
Cervical cancer Cervical cancer is the most common gynecologic malignancy. The most common tumor type is squamous cell carcinoma (80%) A pap smear is only a screening test! Definitive diagnosis of cervical cancer requires a tumor BIOPSY! Radiation and operation are both effective treament . Goal of the treatment: cure, except stage IV

Similar presentations









 Consultant Obstetrician & Gynaecologist Infertility Specialist.>")
 ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY King Abdulaziz University Hospital, Jeddah, Saudi Arabia.>")














