Download presentation
Presentation is loading. Please wait.

1
Carcinoma of the Vulva

2
Incidence of malignant diseases the vulva:
3 - 4% of all gynecologic malignancies. - The incidence increases with age. - Recently there was a rise in the incidence, due to Longevity Increased HPV infections. Increased smoking habits Risk factors for carcinoma of the vulva: 1- Human papillomavirus infection. Genital condylomas: these are detected in 5 % of vulvar cancer. Vulvar intraepithelial neoplasia (VIN) and also CIN. 2- Medical history of: Vulvar dystrophy. Chronic vulvar pruritus. 3- Patients with a history of squamous cell carcinoma of the cervix or vagina. 4- Chronic immunosuppression. 5- Smoking
 and also CIN. 2- Medical history of: Vulvar dystrophy. Chronic vulvar pruritus. 3- Patients with a history of squamous cell carcinoma of the cervix or vagina. 4- Chronic immunosuppression. 5- Smoking.")
3
2 Types / Variants (15%) (85%)
 (85%)")
5
(90%) (2-3%) (5%)
 (2-3%) (5%)")
6
Vulvar Cancer Stages FIGO System
Stage 0 - Carcinoma in situ, VIN 3, severe vulvar dysplasia. Stage I - Tumor 2 cm or less, and confined to the vulva or perineum IA - Less than 1 mm invasion below the surface layer IB - More than 1 mm invasion below the surface layer Stage II - Cancer is confined to the vulva and/or perineum, and larger than 2 cm. Stage III - Cancer has spread to the lower urethra or vagina or anus and / or local lymph nodes on one side. Stage IV A - Cancer has spread to the Upper urethra or bladder or rectum or local lymph nodes on both sides. B - Cancer has spread to the pelvic lymph nodes and/or sites more distant.

7
T N M STAGING T-0 pre-malignant change T-1
A a cancer less than 2.0cm in diameter and less than 1.0mm in depth of invasion B a cancer less than 2.0cm in diameter but greater than 1.0mm in invasion T-2 greater than 2.0 centimeters in diameter T-3 involves vagina, urethra or anus T-4 involves bladder, rectum or pelvic bone N-0 no lymph nodes involved N-1 lymph node metastases to one groin N-2 lymph node metastases to both groins M-1 any distant metastases M-0 no distant metastases

8
Stage I and II Stage III Stage IV

9
Diagnosis The diagnosis often is delayed:
1- Patients do not ask early consultation. They consider the symptoms as a trivial skin condition. 2- Physicians may neglect small skin lesions. Types of complaints: The most common complaint is a palpable vulvar lesion. Chronic pruritus vulvae. Asymptomatic 20% of patients: the lesion is detected during examination for unrelated condition. Later the lesion becomes necrotic cauliflower or hard ulcerated. Bleeding, watery discharge, superinfection and pain may develop. Melanomas: frequently appear as bluish black, pigmented, or papillary lesions.

10
Diagnosis 1) Local examination of the relevant areas: early lesions appears as chronic vulvar dermatitis. 2) Clinical assessment of the lymph nodes is to be performed in the relevant regions. 3) Biopsy: 1- From the suspected lesions: a) Dermal punch biopsy using a local anesthetic: Lesions < 1 cm b) Excisional biopsy under general anesthesia: Lesions > 1 cm: 2- From the lymph nodes in the relevant regions when suspected for metastasis. Differential diagnosis: 1- Venereal diseases: syphilis, chancroid, lymphogranuloma venereum, granuloma inguinale. 2- VIN. An association between invasive and noninvasive lesions is a possibility. 3- Condyloma acuminatum.
 Clinical assessment of the lymph nodes is to be performed in the relevant regions. 3) Biopsy: 1- From the suspected lesions: a) Dermal punch biopsy using a local anesthetic: Lesions < 1 cm. b) Excisional biopsy under general anesthesia: Lesions > 1 cm: 2- From the lymph nodes in the relevant regions when suspected for metastasis. Differential diagnosis: 1- Venereal diseases: syphilis, chancroid, lymphogranuloma venereum, granuloma inguinale. 2- VIN. An association between invasive and noninvasive lesions is a possibility. 3- Condyloma acuminatum.")
13
Prophylaxis…A high index of suspicion
Detection and management of VIN. Proper management of all cases with pruiritus vulvae. All vulval lesions should be diagnosed accurately especially those arising after menopause. All pigmented vulvar lesions should be removed for biopsy.

15
Treatment Options by Stage
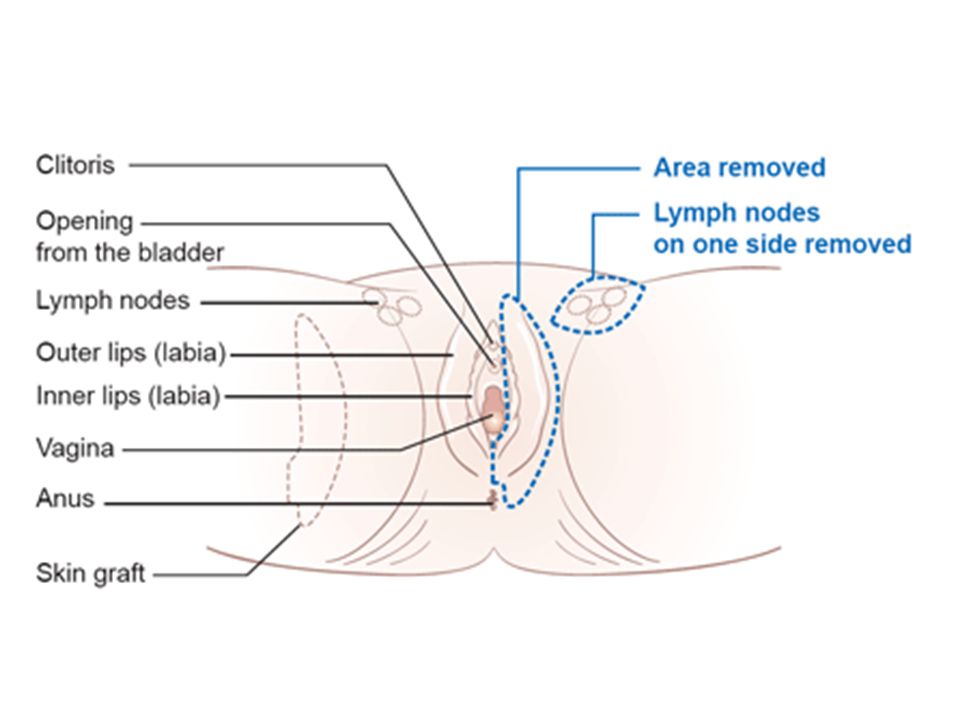
Partial Vulvectomy excision of the tumor, with a 1 cm safe margins. No need for node removal. Ia Ib Modified radical vulvectomy with either of the following: 1) Ipsilateral groin lymph node dissection: in cases of lateralized lesion 2) Bilateral groin node dissection: in cases of centralized lesions Modified radical vulvectomy with bilateral groin node dissection. II - Combined approach: 1- Preoperative external beam radiation therapy. 2- Chemotherapy (e.g. 5-fluorouracil, cisplatin). 3- Radical excision with bilateral inguinal & femoral node dissection. 4- Preoperative RT, then surgical excision of the tumor. - Pelvic exenteration. III Individualized IV
 Ipsilateral groin lymph node dissection: in cases of lateralized lesion. 2) Bilateral groin node dissection: in cases of centralized lesions. Modified radical vulvectomy with bilateral groin node dissection. II. - Combined approach: 1- Preoperative external beam radiation therapy. 2- Chemotherapy (e.g. 5-fluorouracil, cisplatin). 3- Radical excision with bilateral inguinal & femoral node dissection. 4- Preoperative RT, then surgical excision of the tumor. - Pelvic exenteration. III. Individualized. IV.")
16
Vulvectomy: There are several operations in which part of the vulva or all of the vulva is removed: A skinning vulvectomy means only the top layer of skin affected by the cancer is removed. Although this is an option for treating extensive VIN3, this operation is rarely done. Simple vulvectomy, the entire vulva is removed. Radical vulvectomy can be complete or partial. When part of the vulva, including the deep tissue, is removed, the operation is called a partial vulvectomy. In a complete radical vulvectomy, the entire vulva and deep tissues, including the clitoris, are removed. An operation to remove the lymph nodes near the vulva is called a en block dissection. It is important to remove these lymph nodes if they contain cancer.

21
Sentinel Lymph Node

22
Skinning / Simple Vulvectomy

23
Radiotherapy Malignant diseases of the vulva are not commonly managed by RT because of the intolerance of surrounding normal tissues. Chemotherapy as radiation sensitizer can improve response of the malignant tissues. Indications of RT in malignant diseases of the vulva: Preoperative RT in stage III and IV: The lesion shrunk and it limits the need for pelvic exenteration. It also improves surgical respectability of tumors. Postoperative RT: can reduce regional recurrences and inguinal lymph node metastases. Multiple positive groin nodes: It decreases the incidence of recurrence. Positive surgical margins as seen on microscopic examination. Multiple focal recurrences. When the tumor size is > 4 cm

26
Malignant Tumors of the Vagina

27
Incidence High risk factors: 1% of gynecologic malignancies.
It is the 5th in frequency of primary genital malignant diseases. Average age at diagnosis is 65 years old. High risk factors: VaIN Human papillomavirus infection of the cervix or the vulva. Cervical or vulvar cancer. Exposure to diethylstilbestrol (DES) in utero is associated with the development of vaginal adenosis It might progress to clear cell adenocarcinoma of the vagina and cervix in young wome The mean age at diagnosis of this rare malignancy is 19 year.
 in utero is associated with the development of vaginal adenosis. It might progress to clear cell adenocarcinoma of the vagina and cervix in young wome. The mean age at diagnosis of this rare malignancy is 19 year.")
28
Pathological Types: Secondary malignant tumors of the vagina are more common than the primary tumors. The primary lesion may be in the cervix or elsewhere in the body. Primary malignant vaginal tumors: Squamous cell carcinomas: 85% of primary vaginal malignancies. Adenocarcinomas. These occur at younger age group. Clear cell adenocarcinomas secondary to DES exposure. Melanoma. Sarcoma: Sarcoma botryoides (embryonal rhabdomyosarcoma) The peak incidence is in young children at the age of 3 years.
 The peak incidence is in young children at the age of 3 years.")
29
Symptoms of malignant lesions of the vagina:
Abnormal vaginal bleeding: may be postcoital, intermenstrual, or postmenopausal. Watery vaginal discharge. Dyspareunia. Vesicovaginal or rectovaginal fistulae are late manifestations of vaginal cancer. Few patients are asymptomatic; a lesion may be discovered during a routine pelvic examination, or a Pap smear may be abnormal. Signs of malignant lesions of the vagina:: Local examination: the need to inspect the whole vagina entails modification from the routine speculum examination. A polypoid lesion is the commonest macroscopic appearance. A punch biopsy usually yields a diagnosis, but occasionally wide local excision using an anesthetic is necessary. Most lesions occur in the upper 1/3 of the vagina on the posterior wall. Colposcopy, cystoscopy, and proctosigmoidoscopy and bone scan are needed to detect spread.

30
Spread: Direct spread: into the local paravaginal tissues, bladder, or rectum. Lymphatic spread: Lesions in the lower vagina: to the inguinal lymph nodes. Lesions in the upper vagina: to the pelvic lymph nodes. Hematogenous spread: late event. Reach liver, lung, bone.

31
Staging Carcinoma in situ, intraepithelial neolasia Stage 0
Carcinoma limited to the vaginal wall Stage I Involved the subvaginal tissue but not extended to lateral pelvic wall Stage II Extended to pelvic wall Stage III Spread to adjacent organs or direct extension beyond the true pelvis. Stage IV a Spread to distant organs Stage IV b

32
Stage III Stages I & II

33
Treatment: Management of stage 0: Primary localized tumors:
Topical fluorouracil for stage 0: It causes intense burning. Long standing benefits is not proven yet Laser therapy Primary localized tumors: RT: a combination of external beam and brachytherapy. Surgery: it is an alternative treatment for early lesions. Radical hysterectomy with upper vaginectomy. Pelvic exenteration: in vesicovaginal or rectovaginal fistulas.

34
Prognosis: The 5-year survival is as follows: Stage I 65-70%
Stage II 47 % Stage III 30% Stage IV 15-20%

Similar presentations














 Consultant Obstetrician & Gynaecologist Infertility Specialist.>")
 ASSOCIATE PROFESSOR OF GYNECOLOGICAL ONCOLOGY King Abdulaziz University Hospital, Jeddah, Saudi Arabia.>")












