Download presentation
Presentation is loading. Please wait.

1
Heightened Emotional Sensitivity and Transference in BPD
Glen O. Gabbard, M.D. Brown Foundation Chair of Psychoanalysis & Professor of Psychiatry Baylor College of Medicine Training & Supervising Analyst Houston-Galveston Psychoanalytic Institute

2
The Role of the Amygdala
The amygdala increases vigilance The amygdala facilitates an individual’s evaluation of threat or danger BPD patients with histories of childhood trauma have been shown to have hyperreactive amygdalar responses - Herpertz et al., Biol Psych 50: , 2001 EI-I

3
Amygdala Hippocampus Medial Prefrontal Cortex Hypothalamus
Glen O. Gabbard MD March 2001 Medial Prefrontal Cortex Amygdala Hippocampus The hippocampus and orbital prefrontal cortex are seen in a lateral sagital section, the medial PFC, amgygala, hypothalamus, and thalamus are seen in the more medial sagital section. Hypothalamus Orbital Prefrontal Cortex Thalamus

5
Response to Facial Expressions
BPD patients show significantly greater left amygdalar activation to facial expressions compared with normal controls BPD patients attribute negative qualities to neutral faces - Donegan et al 2003 EI-I

6
Amygdala Hyperreactivity (Ekman Faces)
Glen O. Gabbard MD March 2001 Activation map showing regions in the amygdala slice in which activation exceeded the criterion threshold level of P<0.005 for the NC and BPD groups for each of the 4 facial expressions. NC = normal control Donegan et al. Biol Psych 2003;54:1284

8
Amygdala Hyperreactivity
Glen O. Gabbard MD March 2001 Neutral Happy Sad Fearful BPD NC 5 10 15 20 25 30 35 Summed % signal change Left amygdala activation levels for individual subjects within the NC and BPD groups for each of the 4 facial expressions. EI-I - Donegan et al., Biol Psych 2003;54:1284

9
MR Volumetrics: Orbitofrontal Cortex in BPD
Glen O. Gabbard MD March 2001 MR Volumetrics: Orbitofrontal Cortex in BPD L 16 15 14 13 Volume (cm3) Volume (cm3) 12 11 Dual brain pathology in the prefrontal and limbic regions has been hypothesized as central to understanding borderline phenomena. In two studies (Lyoo et all 1998, Tebartz van Elst et al 2003), reductions in medial and orbital frontal lobe volumes have been noted in the brains of borderline patients. Of particular interest, in one of these studies depicted here, is that reduction in the left orbitofrontal volumes correlated significantly with reduction in left amygdala volumes. You can see here in this study of healthy controls (green) versus borderline patients (blue), that left and right orbitofrontal volumes were significantly reduced in comparison to healthy controls. Here, again, left orbitofrontal volumes in borderline patients are less than those of healthy controls. 10 9 8 L R Control BPD = HC = BPD EI-I - van Elst et al., Biol Psych 2003;54:163
 Volume (cm3) Dual brain pathology in the prefrontal and limbic regions has been hypothesized as central to understanding borderline phenomena. In two studies (Lyoo et all 1998, Tebartz van Elst et al 2003), reductions in medial and orbital frontal lobe volumes have been noted in the brains of borderline patients. Of particular interest, in one of these studies depicted here, is that reduction in the left orbitofrontal volumes correlated significantly with reduction in left amygdala volumes. You can see here in this study of healthy controls (green) versus borderline patients (blue), that left and right orbitofrontal volumes were significantly reduced in comparison to healthy controls. Here, again, left orbitofrontal volumes in borderline patients are less than those of healthy controls L. R. Control. BPD. = HC. = BPD. EI-I. - van Elst et al., Biol Psych 2003;54:163.")
10
“Bottom-Up” Regulation of Emotion “BOTTOM-UP” REGULATION
Glen O. Gabbard MD March 2001 AMYGDALA The Prefrontal Cortex: “Top-Down” Regulation The foregoing focus on such subcortical structures as the amygdala only partly addresses the clinical phenomena associated with BPD. The regulatory functions of cortical structures must be taken into account as well. Our emphasis on the amygdala and HPA axis examines borderline object relations from a perspective described in the literature as “bottom up” (reflexive/automatic) regulation (Herpetz et al 2001 need other reference here). REFLEXIVE/AUTOMATIC PROCESSES: “BOTTOM-UP” REGULATION EI-I
 regulation (Herpetz et al 2001 need other reference here). REFLEXIVE/AUTOMATIC. PROCESSES: BOTTOM-UP REGULATION. EI-I.")
11
“TOP-DOWN” REGULATION “BOTTOM-UP” REGULATION
Glen O. Gabbard MD March 2001 PREFRONTAL CORTEX: “TOP-DOWN” REGULATION AMYGDALA Consideration of “top down” regulation by the prefrontal cortex is equally important in understanding the interpersonal difficulties and affective dysregulation seen in patients with borderline personality disorder (Herpetz et al 2001). REFLEXIVE/AUTOMATIC PROCESSES: “BOTTOM-UP” REGULATION
. REFLEXIVE/AUTOMATIC. PROCESSES: BOTTOM-UP REGULATION.")
12
The Frontolimbic Network
The frontolimbic network appears to be central to the emotional dysregulation in BPD This network consists of: anterior cingulate cortex (ACC) orbitofrontal cortex (OFC) dorsolateral prefrontal cortex (DPC) hippocampus amygdala - Schmahl and Bremner, J Psych Res 40: , 2006 EI-I
 orbitofrontal cortex (OFC) dorsolateral prefrontal cortex (DPC) hippocampus. amygdala. - Schmahl and Bremner, J Psych Res 40: , EI-I.")
13
The Frontolimbic Network (cont.)
ACC may be viewed as the brain region mediating emotion. Same brain areas are also involved in dysfunctional serotonergic transmission, associated with impulsive aggression in BPD The subgenual cingulate is involved with emotional control, and studies show that it is deactivated in response to stressful stimuli in BPD ACC dysfunction is probably a key factor in the emotional dysregulation seen in BPD --Schmahl and Herpertz, J Psych Res 41: , 2006 EI-I

15
Frontolimbic Inhibitory Function
BPD patients were asked to push a button for words in standard font but not for italicized words. BPD patients were more impulsive than controls, particularly when the italicized words were negative. In contrast to controls, BPD subjects showed amygdalar reaction and activity in subgenual cingulate and in medial OFC. - Silbersweig et al.: Am J Psych 164: , 2007 EI-I

16
Frontolimbic Inhibitory Function (cont.)
Also in response to negative words, BPD subjects showed activity in the dorsal ACC. Hence even though they were not able to exercise impulse control, they were aware they had to devote other resources to monitoring it. - Silbersweig et al.: Am J Psych 164: , 2007 EI-I

18
Neuroimaging data of adult BPD patients suggest that amygdalar hypersensitivity and emotional dysregulation may be related to specific dysfunctions in the prefrontal cortex and the ACC. -Herpertz et al., Biol Psych 50: , Donegan et al., Biol Psych 54: ,2003 -Schmahl et al., Biol Psych 54: , 2003

19
Heightened Emotional Sensitivity
Misreading of neutral facial expressions is only part of the total picture. Women who are diagnosed as BPD actually can be more accurate in the labeling of fearful facial expressions than controls. - Wagner & Linehan, J Personality Disorders 13: , 1999

20
Heightened Emotional Sensitivity (cont.)
Morphing of facial expressions is needed to accurately assess the capacity of BPD patients to respond to emotional expressions. Faces change gradually and monotonically from neutral to prototypical emotional expressions at maximum intensity. Allows assessment of how intense a facial expression must be before accurately recognized. - Lynch et al, Emotion 4: , 2006 EI-I

21
Morphed Fear Faces – Within Person

22
Heightened Emotional Sensitivity (cont.)
20 BPD subjects and 20 normal controls were compared on the morphing test. BPD patients correctly identified facial affect at an earlier stage than controls. - Lynch et al, Emotion 4: , 2006 EI-I

23
Heightened Emotional Sensitivity (cont.)
BPD subjects were more sensitive than healthy controls in identifying the emotional expressions in general. Their results support the contention that heightened emotional sensitivity might be a core feature of BPD. Findings are consistent with emotional dysregulation as central to BPD—these patients overreact to relatively minor emotional expressions and interpersonal cues. EI-I - Lynch et al, Emotion 4: , 2006

24
How well do BPD patients mentalize?
EI-I

25
Definition Mentalizing is a form of imaginative mental activity, namely, perceiving and interpreting human behavior in terms of mental states (e.g., needs, desires, feelings, beliefs, goals, purposes, and reasons). EI-I
. EI-I.")
26
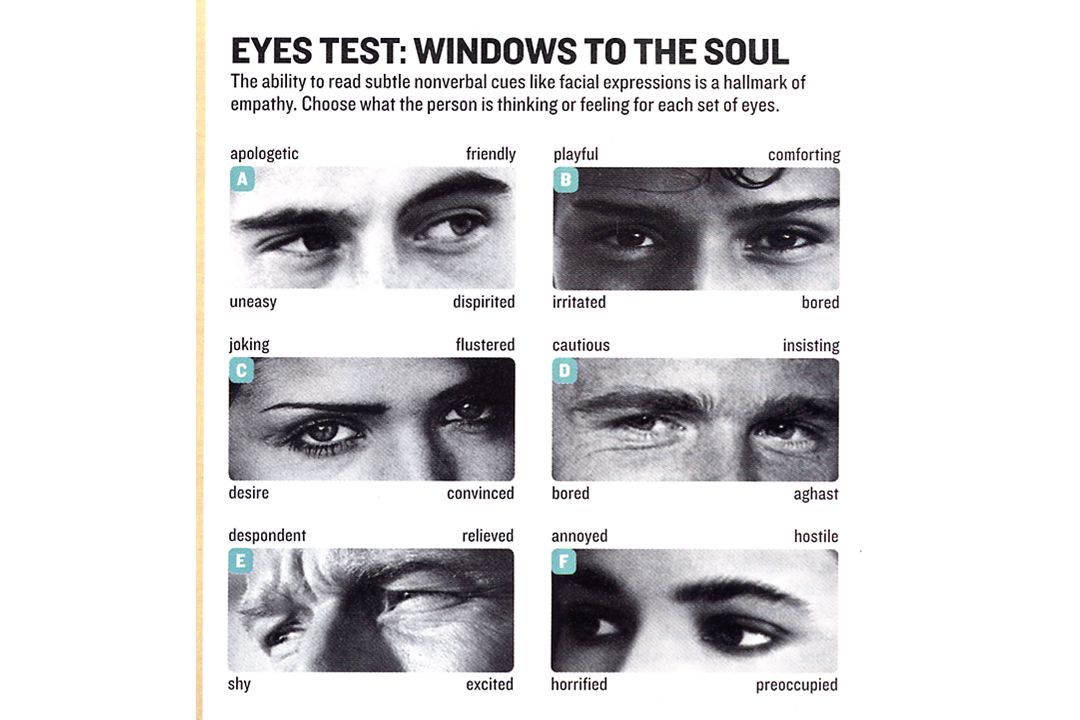
Reading the Mind in the Eyes Test
(RMET) EI-I
 EI-I.")
28
Reading Faces & BPD 30 patients with BPD compared with 25 healthy controls using RMET BPD group performed significantly better than healthy controls. - Fertuck et al, American Psychoanalytic Association, 2009 EI-I

30
Reading Faces & BPD (cont.)
Enhanced performance may be related to greater threat potential perceived in facial stimuli and hypervigilance. Neutral faces may represent the most ambiguous threat, so there is particular vigilance paid to neutral facial expressions. BPD subjects do particularly well compared with controls on neutral faces. - Fertuck et al, American Psychoanalytic Association, 2009 EI-I

31
Reading Faces & BPD (cont.)
Perception of facial expressions is fairly accurate in patients with BPD. BPD patients have adapted to childhood trauma by assessing moment-to-moment shifts in the emotional state of others as a means of surviving. EI-I

32
Reading Faces & BPD (cont.)
The problem area for BPD lies in the interpretation of the emotional expression, not its perception, particularly of neutral or ambiguous states. The main difficulty appears to be assessing whether someone is trustworthy or not—they have difficulty linking trustworthiness with facial expression. EI-I

34
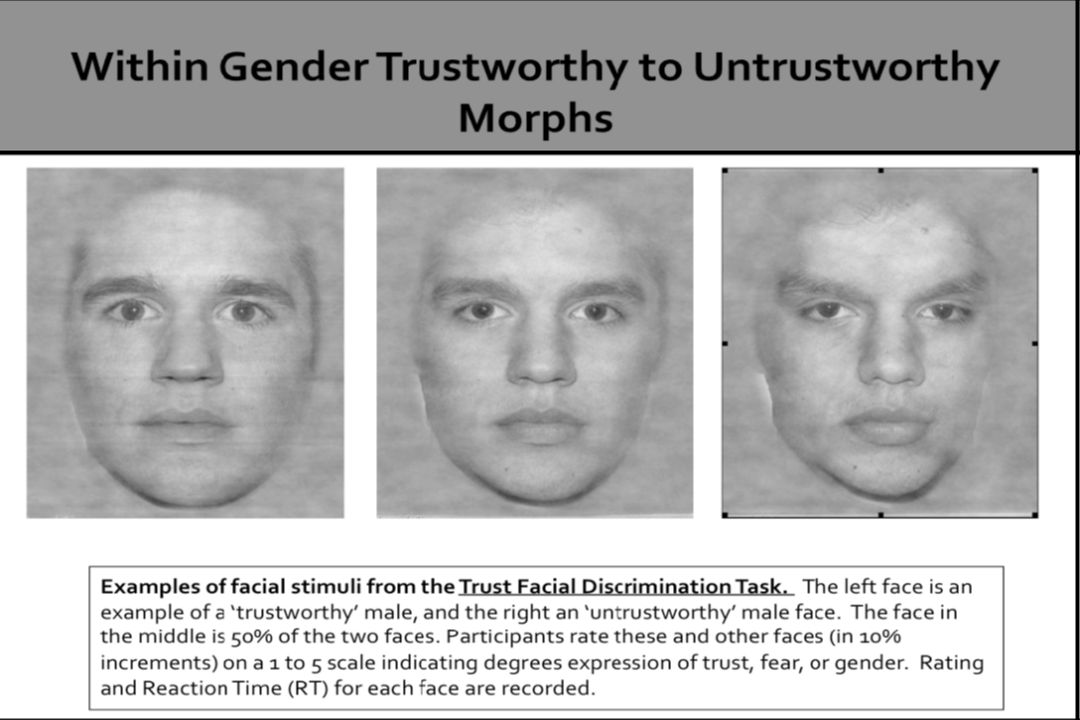
Reading Trustworthiness
BPD group sees faces as less trustworthy than controls In contrast to trust, BPDs and controls read fear similarly BPD group takes longer to judge faces as more trustworthy: also, shows more decision uncertainty - Fertuck 2009 EI-I

35
Paradox in the BPD Field
The so-called “radar” for the therapist’s countertransference reflects the BPD patients’ heightened capacity to read early changes in facial expressions. However, co-existing with this capacity are misinterpretations that are quasi-delusional. EI-I

36
Donegan Subjects on Neutral Faces
“They look like mug shots, like someone who just got arrested” “They look fake, like a façade—they’re hiding something” “They look like they are plotting something—untrustworthy” - Donegan, Biological Psychiatry, 2003 EI-I

37
Paradox in the BPD Field (cont.)
Heightened sensitivity may be both accurate and inaccurate. Accuracy probably varies depending on the state of the attachment relationship, the presence of powerful feelings, and the degree of ambiguity of the facial expression. EI-I

38
Paradox in the BPD Field (cont.)
Mentalizing resides on a continuum from being accurate at some moments to absent at others. Mentalizing is intimately linked to the sense of being understood by an attachment figure, and BPD patients have trouble maintaining mentalization in the context of an intense attachment relationship. The attachment system is hypersensitive in BPD. - Bateman & Fonagy, 2004 EI-I

39
Clinical Implications
Clinician needs to be aware that the patient may be accurately tuning in to a not-yet-conscious feeling state in the therapist. Clinicians must remember that neutral faces represent the most ambiguous threat. It is also possible that the patient may be misinterpreting and overreacting to a small change in facial expression. Therapists must be aware of nonverbal communications to patients. EI-I

40
Emotion Recognition BPD subjects have a bias towards the perception of anger, rejection, or social threat. They see the world and others as dangerous, and themselves as powerless and unacceptable. - Domes et al, J Personality Disorders 23:6-19, 2009 EI-I

41
Emotion Recognition (cont.)
Intact neurocircuitry within the amygdala is essential for intact emotion recognition. Patients with lesions of the amygdaloid complex show impaired recognition of negative facial expressions. - Adolphs et al, Nature 433:68-72, 2005 - Domes et al, J Personality Disorders 23:6-19, 2009 EI-I

42
Emotion Recognition (cont.)
Functional imaging studies have found abnormalities in the prefrontal-amygdalar neurocircuitry mediating affect regulation in BPD subjects. In BPD interference between emotion and cognition has been demonstrated by several studies. Imaging studies suggest that BPD patients show structural and functional alterations in the fronto- limbic network, in particular reduced amygdalar volume and enhanced amygdalar responding to emotional stimuli. Domes et al, J Pers Diorders 23:6-19,2009 EI-I

43
Emotion Recognition (cont.)
Emotional arousal interferes with social or cognitive processing and might contribute to the characteristic alterations in facial emotion recognition. Maternal and romantic love activate an attachment system that may deactivate rational processing of feelings and perceptions of others. - Bateman & Fonagy, 2004 EI-I

44
Indications of Attachment Hyperactivity in Core Symptoms of BPD
Pattern of unstable and intense interpersonal relationships Frantic efforts to avoid abandonment Rapidly escalating tempo, moving from acquaintance to great intimacy - Bateman & Fonagy, 2004 EI-I

45
Pre-Mentalizing Modes of Subjectivity in BPD: Psychic Equivalence Mode
Mind-world isomorphism Mental reality = external reality Intolerance of alternative perspectives—reality is how I see things. EI-I

46
Pre-Mentalizing Modes of Subjectivity in BPD: Psychic Equivalence (cont.)
Perceived loss of attachment figure failure of mentalizing psychic equivalence intensification of unbearable affect self-harm or suicide attempt EI-I

47
Attachment & Mentalizing
Attachment and mentalization are loosely coupled systems existing in a state of partial exclusivity. Mentalization has its roots in the sense of being understood by an attachment figure. BPD is associated with hyperactive attachment systems as a result of early trauma and neglect. Rats placed with neglectful mothers are not calmed by her presence. - Bateman & Fonagy 2004; Nemeroff EI-I

48
Animals with Early Adverse Experience cannot use “social support” to buffer their stress responses
Mother’s presence did not buffer physiological response to stress of Abused infants in comparison to Controls The presence of a social companion buffers the HPA response to stress. (Mat. Sep. monkeys lack this buffering effect-not shown here) 10 14 18 22 26 30 34 0 min 30 min Time After Stress Cortisol (ug/dl) EI-I
 min. 30 min. Time After Stress. Cortisol (ug/dl) EI-I.")
49
Mentalization-Based Therapy?
What is Mentalization-Based Therapy? EI-I

50
An empirically validated therapy for MBT
8 year f/u study shows that it decreases need for inpatient stay, reduces suicidality, improves BPD symptoms and maintains gains compared to controls. -Bateman and Fonagy 1999,2001,2008 EI-I

51
Mentalization-Based Therapy
Designed to stimulate the attachment system while helping patient maintain mentalizing Primary focus is on patient’s current mental state De-emphasizes deep unconscious concerns Recovery of mentalizing is more important than insight EI-I

52
Mentalization-Based Therapy (cont.)
Avoid discussions of past trauma except in the context of reflecting on current perceptions of mental states and change in mental state as victim vs. the current experience Focus on patient’s mind rather than behavior Relate to current event or activity Use of therapist’s mind as model Active engagement with the patient EI-I

53
Mentalization-Based Therapy (cont.)
Identify and praise positive mentalizing Promote curiosity about self and others through an inquisitive stance The mind of the patient is the focus of the treatment, so the therapist is cautious about telling the patient how he feels or thinks EI-I

54
Mentalization-Based Therapy (cont.)
Therapist helps the patient generate multiple perspectives Therapist constructs an image of the patient Patient’s attention is focused on the therapist’s experience when it offers an opportunity to clarify misunderstandings EI-I

55
HOW DOES E M P A T H Y DIFFER FROM MENTALIZATION? EI-I

56
Empathy vs. Mentalizing
Empathy has three components: An affective reaction that involves sharing of another person’s emotional state A cognitive capacity to imagine other people’s perspectives A stable ability to maintain a self-other distinction - Choi-Kain & Gunderson, Am J Psychiatry 165: , 2008 EI-I

57
Empathy vs. Mentalizing
Both involve appreciation of mental states in others Empathy adds the dimensions of sharing in those mental states and having empathic concern for others Empathy is more other-oriented while mentalization is equally self- and other-oriented Empathy involves cognitive skill and experience of affect, but its content is primarily affectively focused - Choi-Kain & Gunderson, Am J Psychiatry 165: , 2008 EI-I

58
Implicit Mentalization
Unconscious, automatic, or procedural operations of an individual’s ability to imagine his own and others’ mental states Taking turns in conversation EI-I

59
Explicit Mentalization
Deliberately makes conscious efforts to know one’s own and others’ internal experiences A therapist actively and consciously works to imagine the mental states of the patient and encourages the patient to do the same EI-I

60
Reflective functioning and BPD
Reflective functioning (RF) is predictive of BPD diagnosis only in subjects with history of abuse Because RF varies depending on context, the assessment of mentalization as a marker of BPD remains problematic. - Choi-Kain & Gunderson, Am J Psychiatry 165: , 2008 EI-I
 is predictive of BPD diagnosis only in subjects with history of abuse. Because RF varies depending on context, the assessment of mentalization as a marker of BPD remains problematic. - Choi-Kain & Gunderson, Am J Psychiatry 165: , EI-I.")
61
Glen O. Gabbard MD March 2001

62
Mirror Neurons & Mentalization
The fundamental mechanism that allows us to understand the actions and emotions of others involves the activation of the mirror neuron system for actions and the activation of viscero-motor centers for the understanding of affect. Action observation causes the automatic activation of the same neural mechanism triggered by action execution or even by the sound produced by the same action. - Gallese et al, Trends in Cognitive Science 8: , 2004 - Koehler et al, Science 97: , 2002 EI-I

63
Mirror Neurons & Mentalization (cont.)
The 2-level system underpinning mentalization is: A frontocorticol system involving cognitive interpretation of visual representations A mirror-neuron system subserving more immediate, direct understanding of the other The anterior insula mediates communication between the limbic system and mirror neurons: we replay observed actions and react emotionally - Wicker et al, Neuron 40: , 2003 EI-I

64
EI-I

65
Mirror Neurons & Mentalization (cont.)
The inhibition of imitative behavior involves cortical areas related to mentalizing. This allows us to differentiate self and other. It is not the mirror system per se that is related to mentalizing, but rather the control of the mirror system. - Fonagy 2009 - Brass & Haggard, Neuroscientist 14: , 2008 EI-I

66
CONCLUSIONS BPD patients are unusually perceptive but tend to misinterpret trustworthiness Mentalizing exists on a continuum and is highly variable in BPD EI-I

67
CONCLUSIONS Therapists must take into account BOTH the possibility of accurate perception of unconscious emotion in the therapist AND the transference-based misinterpretation of those perceptions EI-I

Similar presentations















 Amir Shams Tabrizi.>")
 Amygdala hyperactivity is present in MDD, in both depressed and remitted individuals. (B) This hyperactivity distinguishes an MDE and predicts.>")





 Neuroimaging and attitudes to faces.>")

