Download presentation
Presentation is loading. Please wait.

1
Western Montana Pain Symposium Treating Persistent Pain Does Not Need to Be Painful—Improving Outcomes through Pain Education Nora Stern, PT, MS PT Providence Persistent Pain Project Program Manager Portland, Oregon

2
Conflict of Interest Disclosure Nora Stern, PT, MS, PT Has no real or apparent conflicts of interest to report.

4
Objectives Understand pain as an output of the nervous system Evaluate clinical decision-making reflecting this understanding Understand role of pain education and team based care in treatment of persistent pain

5
What is the purpose of pain? Pain is a protector When you have persistent pain, beyond tissue healing, what is the pain protecting you from?

6
Previous model

7
Current Model– CHAOTIC

8
Pain and the Brain Central Sensitization

9
From Nocioceptive Input to Processing to Output

10
Changes that occur with persistent pain

11
Peripheral Sensitization: Elevation of resting state of neuron

12
Nocioceptive Input Travels Up Spinothalamic Tract to Brain

13
Brain functions

14
Central Nervous System Wetware: - Amino acids, peptides, amines, all play a role in excitation or inhibition Hardware: – Neurons – Glia

15
Brain centers for pain neuromatrix Thalamus and Hypothalamus: stress response, autonomic regulation, motivation Amygdala: fear, fear conditioning, addiction: If you know it’s going to hurt, then it’s going to hurt! Sensory homunculus: tells us where sensation occurs. This can become blurred and “smudged” with changes in movement habits Primary motor cortex: organizes and prepares for movement. Affected by fear of hurting oneself Prefrontal and frontal cortex: makes sense out of the situation. Decides if the danger signal is a real threat Cingulate cortex: concentration and focus, affected by attention to pain Cerebellum: Perception of movement Hippocampus: memory, spatial cognition, fear conditioning

16
Brain functions for pain neuromatrix Thinking: looking for answers Feeling: Fear avoidance, catastrophizing Sensing: sensory homuncular organization, kinesthetic sense Acting/moving: motor planning, anticipating pain with motion

17
Mirror neuron function 25% of our brain’s neurons may have a mirror capacity

18
Output 1. Pain sensation as an output: assigned to the virtual body representation 2. Message to Autonomic Nervous System Neuroendocrine System Neuroimmune System

19
Fight or flight response left turned on

20
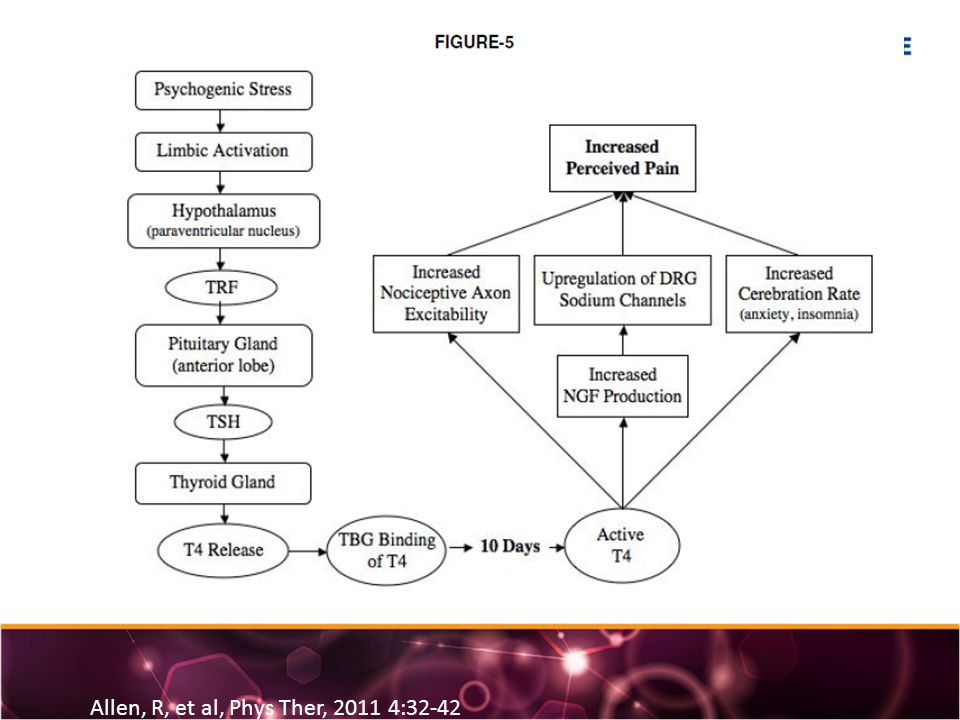
Stress/pain relationship with CRPS Allen, R, et al, Phys Ther, 2011 4:32-42

22
PARADIGM SHIFT PAIN ≠ HARM PAIN IS AN OUTPUT FROM THE BRAIN ALL PAIN IS REAL PAIN NOCICEPTION IS NEITHER NECESSARY NOR SUFFICIENT FOR PAIN adapted from material from G. Lorimer Moseley: Understand and Explain Pain course material 2010

23
Managing and Coping with Chronic Pain Understanding and Treating Persistent Pain Reference: “Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education and Research,” Board of Health Science Policy, Institute of Medicine, of National Academies, Washington 2011 VS.

24
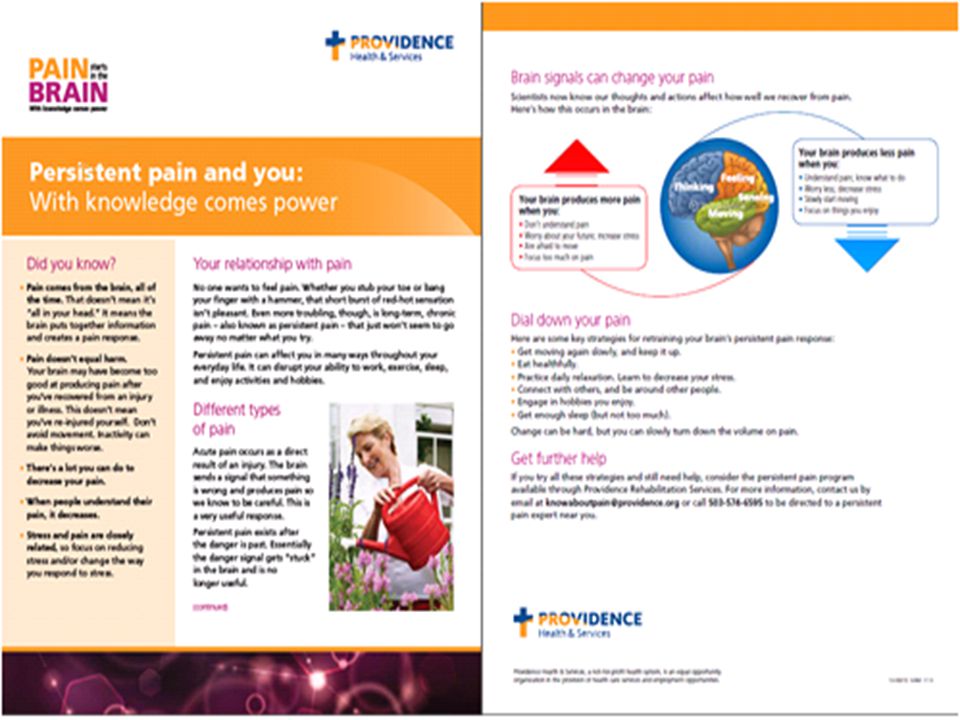
Pain Education: A treatment intervention

25
Pain Education As A Treatment Intervention Decrease in pain rating (Van Oosterwijck et al 2011, Meeus et al, 2010, Ryan et al, 2010, Moseley, 2002, 2003, 2004) Decrease in fear of reinjury (Van Oosterwijck et al 2011, Moseley, 2002, 2003) Decrease in pain catastrophizing (Meeus et al, Moseley 2004) Increase in function (Van Oosterwijck et al 2011, Moseley, 2002, 2003
 Decrease in fear of reinjury (Van Oosterwijck et al 2011, Moseley, 2002, 2003) Decrease in pain catastrophizing (Meeus et al, Moseley 2004) Increase in function (Van Oosterwijck et al 2011, Moseley, 2002, 2003")
26
Pain education as treatment Brain activity: persistent pain patient, baseline S/P 2 weeks practice of abdominal strengthening Brain activity same day, following pain education Moseley, G. L, “Brain activity before and after 1:1 pain education with physiotherapist.” Australian Journal of Physiotherapy 2005 Vol. 51

27
Outcomes After Pain Education in ED Oliviera et al Spine Volume 31 Number 15 2006

28
Persistent Pain Project Patient Outcomes

29
Components of pain education: Providence Oregon Phrasing All providers able to explain pain as an output – Provider training: rehab, primary care – Upcoming: inpatient Written material Video Patient classes

31
Patient access online

32
Providence Pain Video http://providenceoregon.org/video/pain

34
How do we do better? – Speak the same language and explain pain – Address the issues that are causing central sensitization in primary care, behavioral health, rehab, complementary medicine – Team care: medical home – Advocate for adequate coverage for high risk patients

35
Fighting central sensitization One patient at a time

Similar presentations




 Neuropeptides 1) ACh 2) Amino Acids 3) Biogenic Amines.>")





 Colbran Marjerrison.>")









