Download presentation
Presentation is loading. Please wait.

1
Interventions for Clients with Colorectal Cancer

2
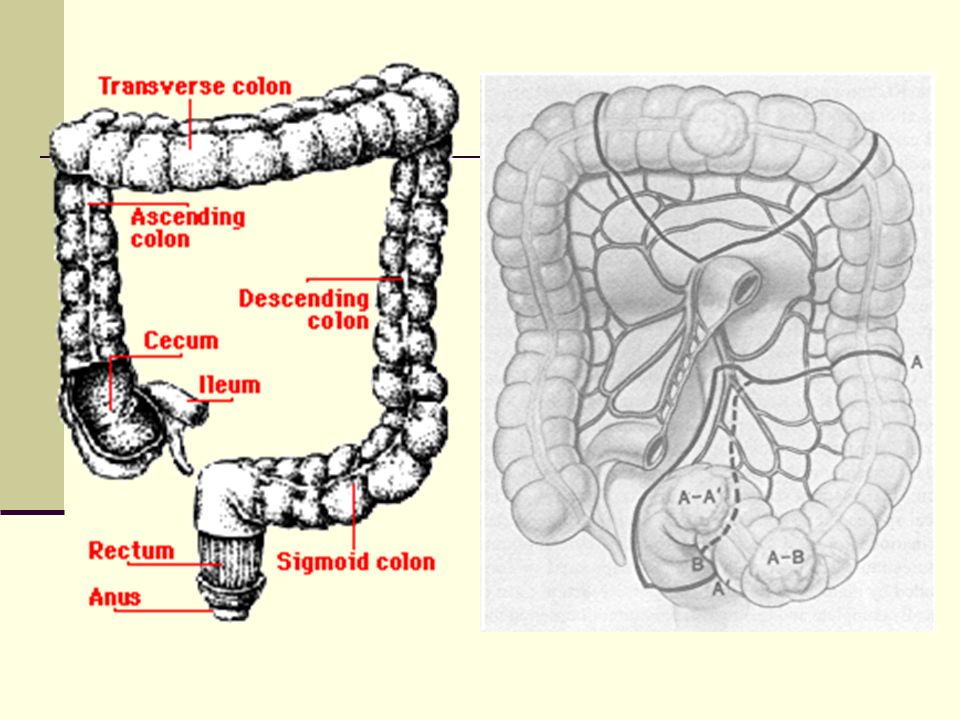
What is the Function of the Colon and Rectum?
The colon and rectum comprise the large intestine (large bowel) The primary function of the large bowel is to turn liquid stool into formed fecal matter
 The primary function of the large bowel is to turn liquid stool into formed fecal matter.")
3
What is Cancer? A group of 100 different diseases
The uncontrolled, abnormal growth of cells Cancer may spread to other parts of the body

4
What is Colorectal Cancer?
Third most common type of cancer and second most frequent cause of cancer-related death A disease in which normal cells in the lining of the colon or rectum begin to change, grow without control, and no longer die Usually begins as a noncancerous polyp that can, over time, become a cancerous tumor

5
Typical sites of incidence and sympoms of colon cancer

6
Colon cancers result from a series of pathologic changes that transform normal colonic
epithelium into invasive carcinoma. Specific genetic events, shown by vertical arrows, accompany this multistep process. The various chemopreventive agents exert their effects at different steps in this pathway, and this is depicted on the basis of the available epidemiologic evidence, the results of studies in animals, and the known mechanisms of action of the agents.

7
What Are the Risk Factors for Colorectal Cancer?
Polyps (a noncancerous or precancerous growth associated with aging) Age Inflammatory bowel disease (IBD) Diet high in saturated fats, such as red meat Personal or family history of cancer Obesity Smoking Other
 Age. Inflammatory bowel disease (IBD) Diet high in saturated fats, such as red meat. Personal or family history of cancer. Obesity. Smoking. Other.")
8
Development of CRC result of interplay between environmental and
genetic factors Central environmental factors: diet and lifestyle 35% of all cancers are attributable to diet 50%-75% of CRC in the US may be preventable through dietary modifications

9
Dietary factors implicated in colorectal carcinogenesis
consumption of red meat animal and saturated fat refined carbohydrates alcohol increased risk

10
Dietary factors implicated in colorectal carcinogenesis
dietary fiber vegetables fruits antioxidant vitamins calcium folate (B Vitamin) decreased risk
 decreased risk.")
13
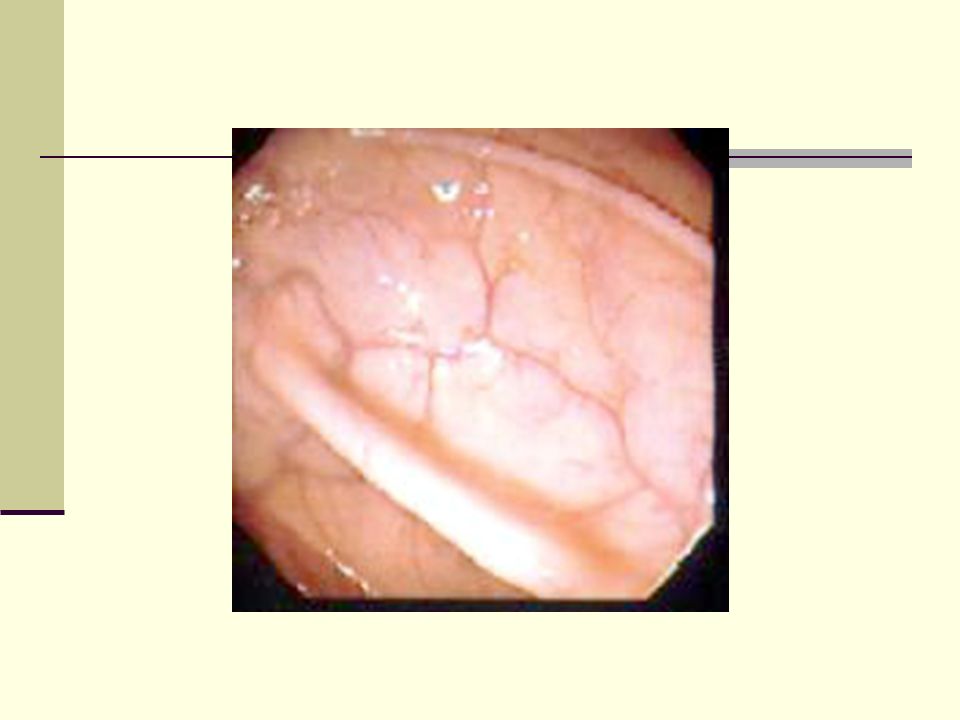
There is a solitary mass attached via a long stalk to the colonic mucosa. It is discreet and does not involve the wall of the colon. The surface is dark red (hemorrhagic). The stool guaiac was positive.
. The stool guaiac was positive..")
14
This is an adenocarcinoma of the cecum which demonstrates an exophytic growth pattern, as the bulk of the mass is within the bowel lumen. The patient had iron deficiency anemia.

15
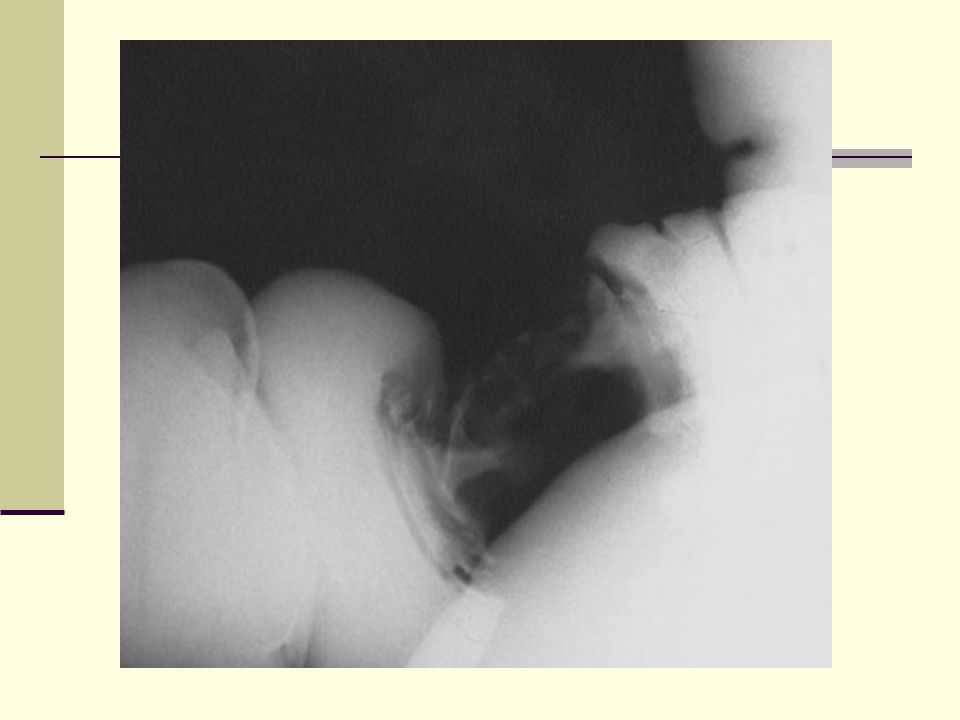
The barium enema techniqu
instills the radiopaque barium sulfate into the colon, producing a contrast with the wall of the colon that highlights any masses present. In this case, the classic "apple core” lesion is present, representing an encircling adenocarcinoma that constricts the lumen.

18
Symptoms associated with CRC
rectal bleeding change in bowel habits obstruction abdominal pain & mass iron-deficiency anemia weight loss loss of appetite night sweats fever

19
Staging of CRC TNM system Primary tumor (T) Regional lymph nodes (N)
Distant metastasis (M) *Note: Tis includes cancer cells confined within the glandular basement membran e (intraepithelial) or lamina propria (intramucosal) with no extension through the muscularis mucosae into the submucosa. **Note: Direct invasion in T4 includes invasion of other segments of the colorectum by way of the serosa; for example, invasion of the sigmoid colon by a carcinoma of the cecum.
 *Note: Tis includes cancer cells confined within the glandular basement membran. e (intraepithelial) or lamina propria (intramucosal) with no extension through the. muscularis mucosae into the submucosa. **Note: Direct invasion in T4 includes invasion of other segments of the colorectum. by way of the serosa; for example, invasion of the sigmoid colon by a carcinoma of the. cecum.")
20
Stage 0 Colorectal Cancer
Known as “cancer in situ,” meaning the cancer is located in the mucosa (moist tissue lining the colon or rectum) Removal of the polyp (polypectomy) is the usual treatment
 Removal of the polyp (polypectomy) is the usual treatment.")
21
Stage I Colorectal Cancer
The cancer has grown through the mucosa and invaded the muscularis (muscular coat) Treatment is surgery to remove the tumor and some surrounding lymph nodes
 Treatment is surgery to remove the tumor and some surrounding lymph nodes.")
22
Stage II Colorectal Cancer
The cancer has grown beyond the muscularis of the colon or rectum but has not spread to the lymph nodes Stage II colon cancer is treated with surgery and, in some cases, chemotherapy after surgery Stage II rectal cancer is treated with surgery, radiation therapy, and chemotherapy

23
Stage III Colorectal Cancer
The cancer has spread to the regional lymph nodes (lymph nodes near the colon and rectum) Stage III colon cancer is treated with surgery and chemotherapy Stage III rectal cancer is treated with surgery, radiation therapy, and chemotherapy
 Stage III colon cancer is treated with surgery and chemotherapy. Stage III rectal cancer is treated with surgery, radiation therapy, and chemotherapy.")
24
Stage IV Colorectal Cancer
The cancer has spread outside of the colon or rectum to other areas of the body Stage IV cancer is treated with chemotherapy. Surgery to remove the colon or rectal tumor may or may not be done Additional surgery to remove metastases may also be done in carefully selected patients

25
Staging of CRC Dukes staging system A Mucosa 80%
B Into or through M. propria 50% C1 Into M. propria, + LN ! 40% C2 Through M. propria, + LN! 12% D distant metastatic spread <5%

26
Sites of metastasis Via blood Via lymphatics Per continuitatem Liver
Lung Brain Bones Lymph nodes Abdominal wall Nerves Vessels

27
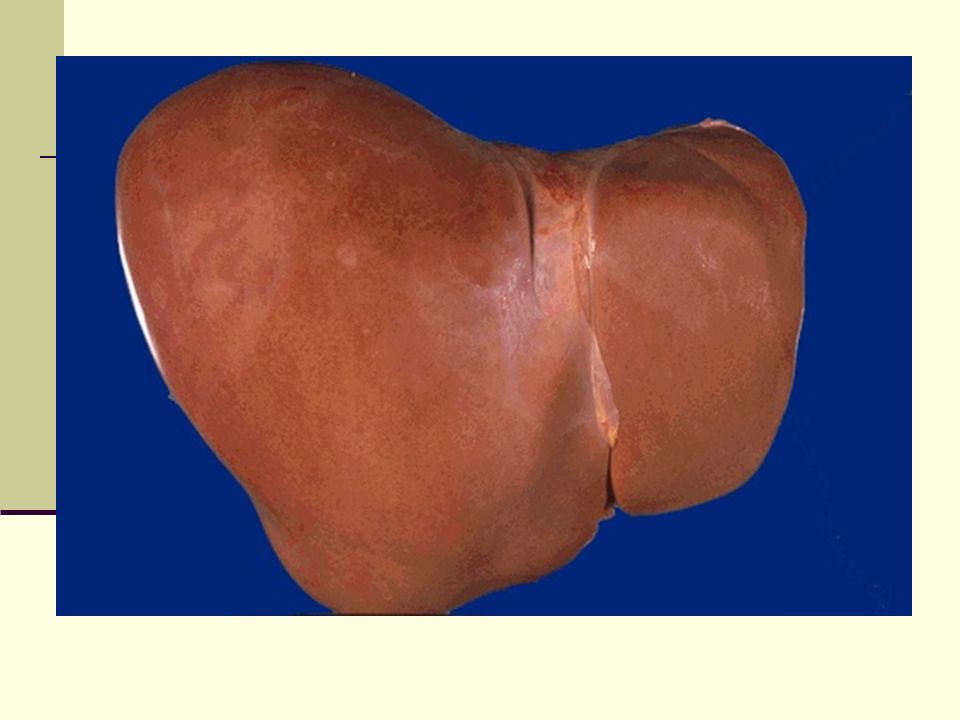
This is an in-situ photograph of the
chest and abdominal contents. As can be seen, the liver is the largest parenchymal organ, lying just below the diaphragm. The right lobe (at the left in the photograph) is larger than The left lobe. The falciform ligament is the rough dividing line between the two lobes.
 is larger than. The left lobe. The falciform ligament is. the rough dividing line between the. two lobes.")
29
The liver is filled with multiple masses of varying size
The liver is filled with multiple masses of varying size. The primary was a colonic adenocarcinoma. Some of the larger metastatic nodules have central necrosis.

30
Coping With the Side Effects of Cancer and its Treatment
Side effects are treatable; talk with the doctor or nurse Fatigue is a common, treatable side effect Pain is treatable; non-narcotic pain relievers are available Antiemetic drugs can reduce or prevent nausea and vomiting

31
Follow-Up Care Doctor’s visits
Serial carcinoembryonic antigen (CEA) measurements are recommended Colonoscopy one year after removal of colorectal cancer Surveillance colonoscopy every three to five years to identify new polyps and/or cancers
 measurements are recommended. Colonoscopy one year after removal of colorectal cancer. Surveillance colonoscopy every three to five years to identify new polyps and/or cancers.")
32
Summary CRC is a leading cause of death Early stages are detectable Screening can prevent CRC

Similar presentations












>")







