Download presentation
Presentation is loading. Please wait.

1
Bordatella Pertussis Adaobi Okobi, M.D.

2
Learning Objectives Epidemiology
Review the clinical features and natural history of pertussis Discuss differential diagnosis Treatment, Complications

3
Introduction Pertussis is a respiratory tract infection caused by Bordatella pertussis transmitted by aerosolized droplets from coughing B. Pertussis is a small, gram negative pleomorphic coccobacillus

4
Epidemiology 30-50 million cases/year worldwide
300,000 deaths/year worldwide 84% of children in the US who died of the disease from were under 6 months Periodic epidemics occur every 3-5 years despite vaccination efforts Increasing incidence of the disease because of waning immunity in the adolescent and adult population as well as fewer people vaccinating their children

5
Epidemiology Data from: the Centers for Disease Control and Prevention

6
Epidemiology Data from: the Centers for Disease Control and Prevention

7
Natural History Incubation period: 7-10 days Three phases Catarrhal
Paroxsymal Convalescent

8
Phase 1: Catarrahal Similar to the “common cold”
Mild cough and runny nose Duration: 1-2 weeks If fever is present it is low-grade Cough worsens instead of improves, unlike typical URIs May be short or absent in infants

9
Phase 2: Paroxsymal Cough is persistent and severe
Long series of coughs which may result in gagging, cyanosis or post-tussive emesis May also be associated with apnea or bradycardia in young infants Coughing may be spontaneous or induced Whooping (noise associated with force inspiration) is uncommon in children Duration: 2-6 weeks *Complications are most likely to occur during this stage
 is uncommon in children. Duration: 2-6 weeks. *Complications are most likely to occur during this stage.")
10
Phase 3: Convalescent Cough gradually decreases over several weeks to months Cough may recur with subsequent URIs for months after the disease has resolved

11
Differential Diagnosis
Mycoplasma pneumoniae Chlamydia spp. Tuberculosis Viral RSV Adenovirus Parainfluenza Influenza Rhinovirus Foreign body aspiration Asthma/Reactive Airway Disease Reflux Aspiration pneumonia Croup Sinusitis TE fistula Congestive heart failure

12
Diagnosis Clinical Case Definition Laboratory Criteria
A cough illness lasting at least 2 weeks with one of the following: paroxysms of coughing, inspiratory "whoop," or posttussive vomiting, without other apparent cause (as reported by a health professional). Clinical case definition is appropriate for endemic or sporadic cases. In outbreak settings, a case may be defined as a cough illness lasting at least 2 weeks (as reported by a health professional). Nasopharyngeal culture Polymerase chain reaction (PCR) Direct fluorescent antibody testing of nasopharyngeal secretions has been shown to have low sensitivity and variable specificity. Serologic testing for pertussis is not widely available nor is it standardized
. Clinical case definition is appropriate for endemic or sporadic cases. In outbreak settings, a case may be defined as a cough illness lasting at least 2 weeks (as reported by a health professional). Nasopharyngeal culture. Polymerase chain reaction (PCR) Direct fluorescent antibody testing of nasopharyngeal secretions has been shown to have low sensitivity and variable specificity. Serologic testing for pertussis is not widely available nor is it standardized.")
13
Specimen Collection

14
Diagnosis Laboratory findings: CXR:
Lymphocytosis >10,000 lymphocytes/microL CXR: May be normal or have peribronchial cuffing, perihilar infiltrates or atelectasis *Confirmed cases should be reported to the Department of Health

15
Complications Vomiting Seizures (1-2%) Encephalopathy (0.3%) Death
Apnea (50%) Infants < 6 months; likely related to vagal stimulation Pneumonia (20%) May be primary or from bacterial superinfection Associated with extreme leukocytosis (>60,000 cells/microL) May have associated pulmonary hypertension Increased risk of mortality Vomiting Seizures (1-2%) Encephalopathy (0.3%) Likely from hypoxia related to coughing Death Most occur in infants < 6 months (1% case fatality rate) with the majority under 2 months
 Infants < 6 months; likely related to vagal stimulation. Pneumonia (20%) May be primary or from bacterial superinfection. Associated with extreme leukocytosis (>60,000 cells/microL) May have associated pulmonary hypertension. Increased risk of mortality. Vomiting. Seizures (1-2%) Encephalopathy (0.3%) Likely from hypoxia related to coughing. Death. Most occur in infants < 6 months (1% case fatality rate) with the majority under 2 months.")
16
Hospitalization Indications for admission: Indications for discharge:
Respiratory distress Evidence of pneumonia Inability to feed Cyanosis or apnea Seizures Indications for discharge: Tolerate coughing without bradycardia or hypoxia Adequate PO intake Caregivers are comfortable with the child Close outpatient follow up can be obtained

17
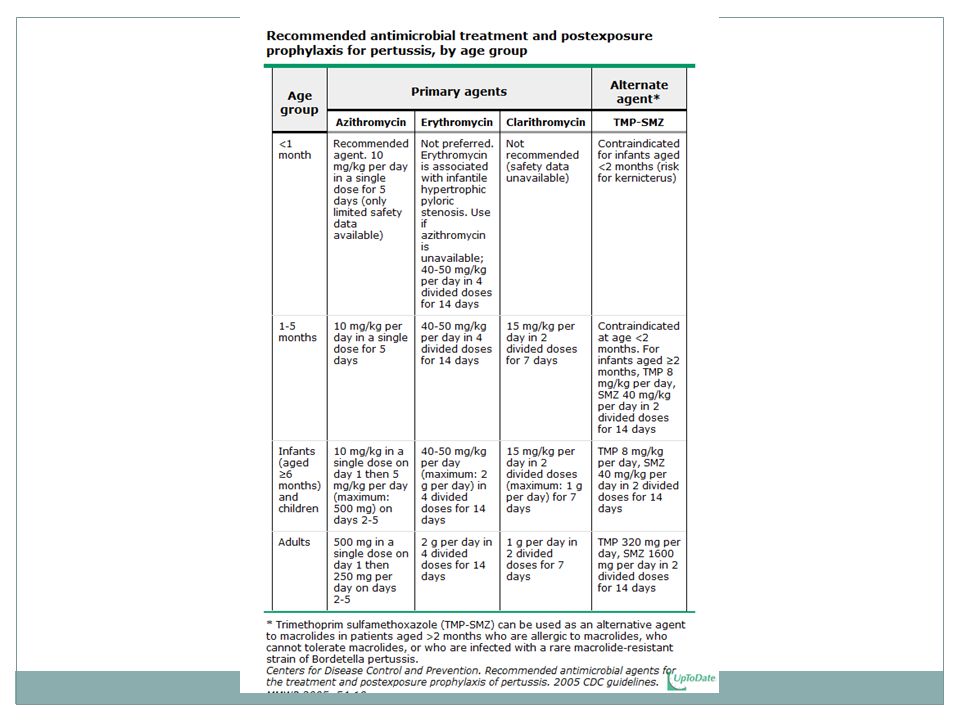
Treatment Treat anyone with symptoms and lab evidence of infection
Droplet precautions (mask within 3 feet) x 5 days after treatment Supportive- Cardiopulmonary monitoring Pulse oximetry Monitor PO intake Antimicrobials- Azithromycin x 5 days Erythromycin x 14 days Clarithromycin x 7 days Bactrim x 14 days Early treament (within 1 week) may decrease severity of symptoms Treatment within 2 weeks of cough decreases spread of infection
 x 5 days after treatment. Supportive- Cardiopulmonary monitoring. Pulse oximetry. Monitor PO intake. Antimicrobials- Azithromycin x 5 days. Erythromycin x 14 days. Clarithromycin x 7 days. Bactrim x 14 days. Early treament (within 1 week) may decrease severity of symptoms. Treatment within 2 weeks of cough decreases spread of infection.")
19
Prophylaxis Antibiotic prophylaxis recommended for all close contacts:
Face to face contact (within 3 feet) Direct contact with respiratory, oral or nasal secretions Sharing the same confined space for > 1 hr
 Direct contact with respiratory, oral or nasal secretions. Sharing the same confined space for > 1 hr.")
20
Take Home Points Pertussis is a very contagious respiratory pathogen
There are 3 phases: catarrhal, paroxsymal, and convalescent Infants under 6 months have the highest mortality rate Complications include apnea, pneumonia, seizures, encephalopathy, and death Treat with macrolides as soon as the diagnosis is suspected and give prophylaxis to any close contacts

Similar presentations











 Management Presentation>")




 DR (MRS) M.B. FETUGA.>")


