Download presentation
Presentation is loading. Please wait.

1
Consultant Radiologist Riyadh Military Hospital
Abdominal trauma Role of CT Dr. Ahmed Refaey Consultant Radiologist Riyadh Military Hospital MBBCh, MS, FRCR

2
Format of the lecture Categorization of abdominal trauma patients
CT technique CT findings Illustrated cases

3
Categories of abdominal trauma patients
Category A - hemodynamically unstable patients Category B - hemodynamically stable patients Category C - patients with hematuria

4
Category A “hemodynamically unstable”
Need rapid clinical evaluation and immediate resuscitation with volume replacement If not responding, they should go immediately to OR without imaging If they respond ( become hemodynamically stable )-- Category B
-- Category B.")
5
Category B “ hemodynamically stable”
High clinical suspicion of intra-abdominal injury ------ CT not U/S Low clinical suspicion of intra-abdominal injury ------ U/S not CT

6
High clinical suspicion of intra-abdominal injury

7
don’t ask for U/S - miss 25% of liver injuries - miss 62 % of splenic injuries - most renal injuries - all pancreatic injuries - all mesenteric injuries - all gut injuries - high proportion of retroperitoneal hematoma

8
Low clinical suspicion of intra-abdominal injury

9
U/S If -ve ------- > release the patient from observation
* If +ve ----- CT

11
Category C “ patient with hematuria”
CT cystograhy

12
Categories of blunt abdominal trauma
Category A - hemodynamically unstable patients * no radiological imaging Category B - hemodynamically stable patients * CT – if high suspicion * US – if low suspicion Category C - patients with hematuria * CT cystography

13
CT technique

14
CT in blunt abdominal trauma with or without oral contrast ?
Oral contrast is unnecessary in CT evaluation in patients with acute blunt abdominal trauma

15
Why no oral contrast ?

16
Extravasation of oral contrast in bowel perforation
0 % - 19 % Pneumopertoneum 50 % * - small perforations may seal quickly and prevent extravasation of contrast and / or air that could then be detected by CT

17
Time delay to diagnosis
Long transit time non opacification of distal loops Aspiration of gastric contrast contents with subsequent pulmonary toxic effects Interference with the diagnosis of contrast blush

18
Oral contrast is unnecessary in CT evaluation in patients with acute blunt abdominal trauma
96. Allen TL, Mueller MT, Bonk RT, et al. Computed tomographic scanning without oral contrast solution for blunt bowel and mesenteric injuries in abdominal trauma. J Trauma 2004; 56(2):
:")
19
No Is pneumoperitoneum diagnostic of bowel injury?
it is not diagnostic of bowel injury, since air transmitted from the chest in pneumothorax is the most common cause of intraperitoneal air in a trauma patient

20
The sensitivity of CT scan with OC for detection of bowel injuries does not significantly differ from CT without OC Clancy TV, Ragozzino MW, Ramshaw D, Churchill MP, Covington DL, Maxwell JG. Oral contrast is not necessary in the evaluation of blunt abdominal trauma by computed tomography. Am J Surg. 1993;166: Sherck J, Shatney C, Sensaki K, Selivanov V. The accuracy of computed tomography in the diagnosis of blunt small-bowel perforation. Am J Surg. 1994;168:

21
Trauma protocol

22
Blunt trauma No oral contrast Venous phase ----- 70 sec
Delayed scan if injury present min

23
CT findings

24
The findings to look for
Hemoperitoneum Contrast blush Laceration Hematomas Contusion Pneumoperitoneum Devascularization of organs Subcapsular hematoma

25
* Laceration : linear shaped hypodense lesion * Hematoma : oval or round hypodense areas * Contusion : vague ,ill-defined hpodense area , that is less perfused

26
Contrast blush An area of high density compared to the nearby
vessel representing active arterial extravasation

29
Illustrated cases

30
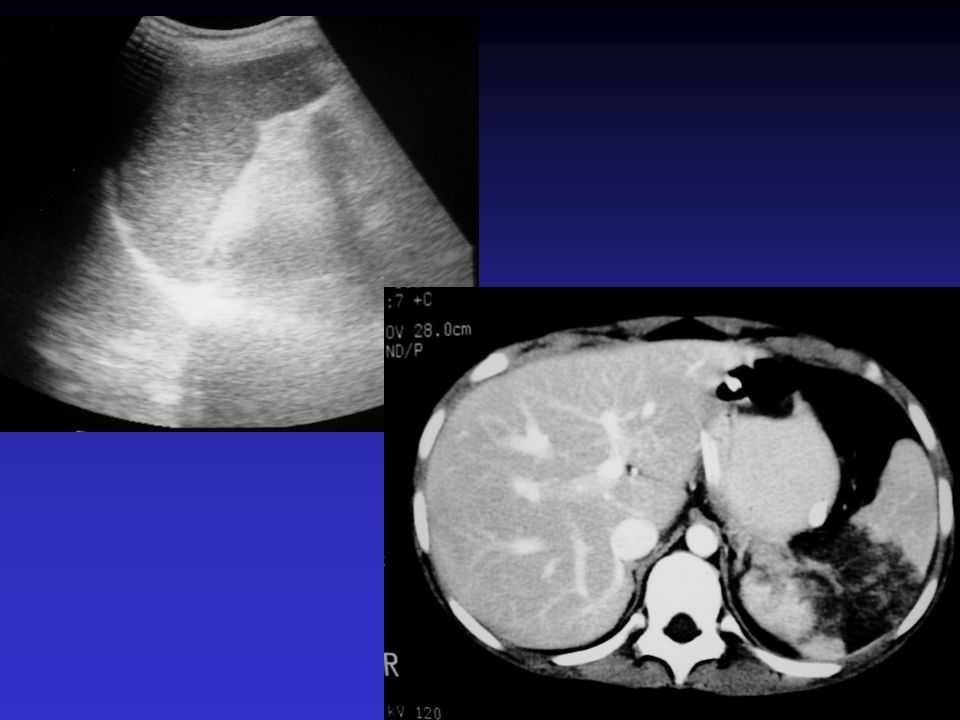
Splenic injuries

31
Splenic laceration hemoperitoneum No contrast blush …managed non-operatively

32
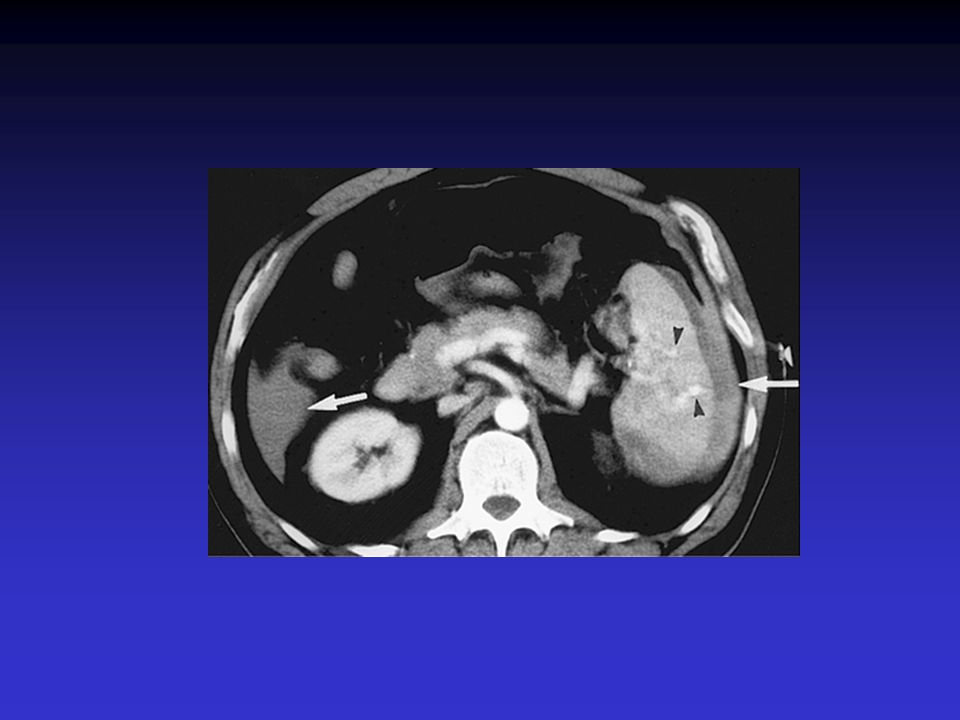
Lacerations Hematoma Hemoperitoneum No contrast blush .. Depending on the clinical condition , the patient will be managed

33
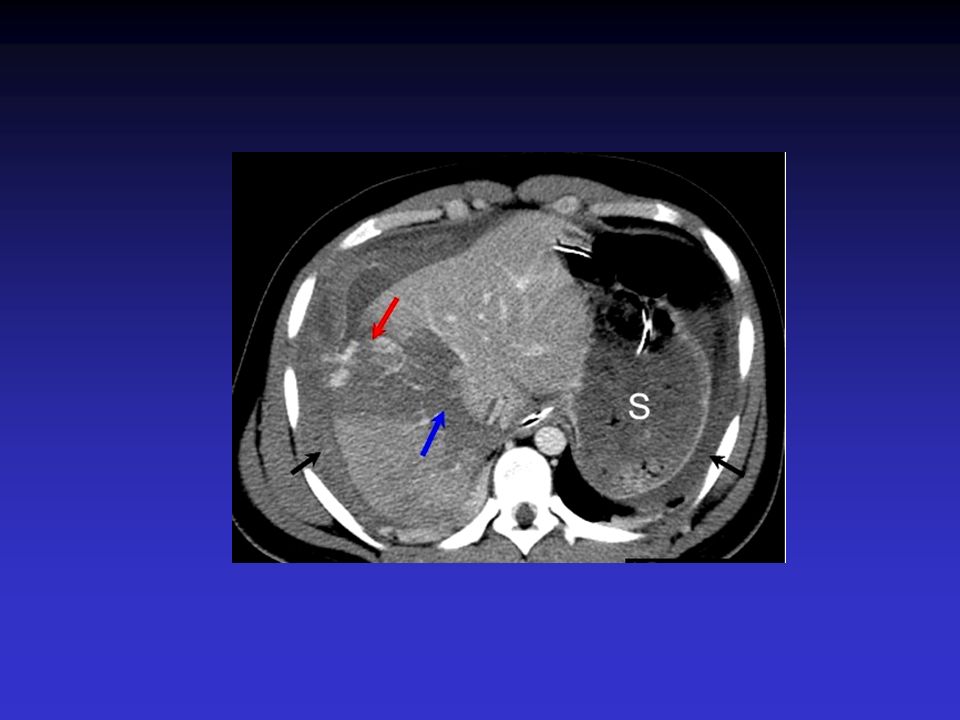
Hemoperitoneum Laceration Hematoma Contrast blush .. Operative management

35
Liver injuries

36
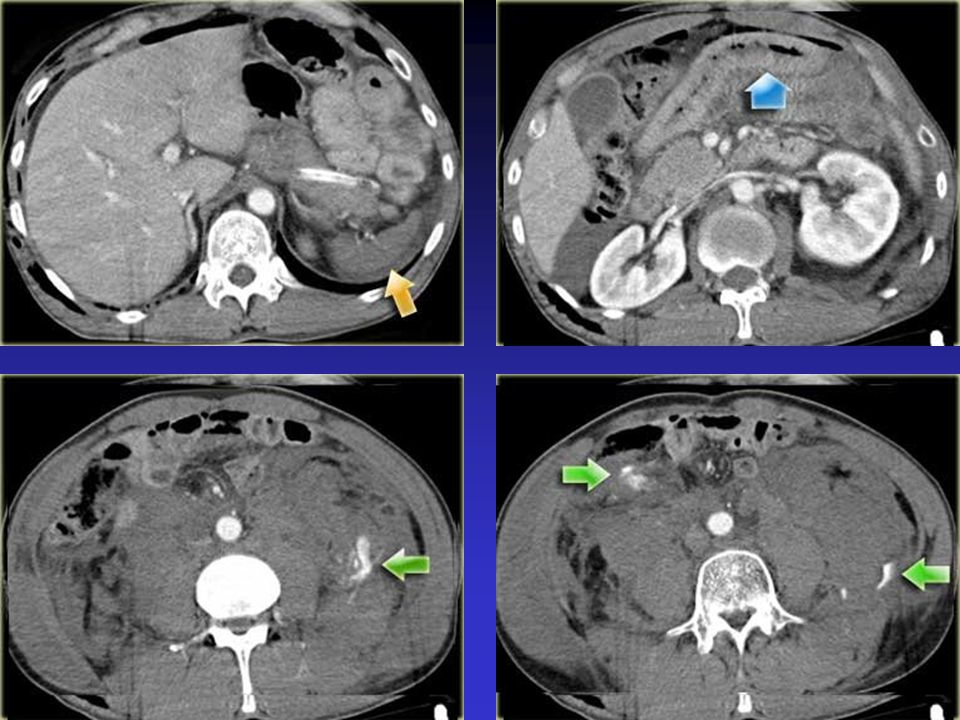
Green arrow: hematoma Blue arrow : contusion Yellow arrow: laceration hemoperitoneum

37
Hematoma hemoperitoneum Contrast blush … managed operatively

38
Does the presence of contrast blush necissetate operative interference ?
No It depends on if it is associated with hemoperitoneum or no

39
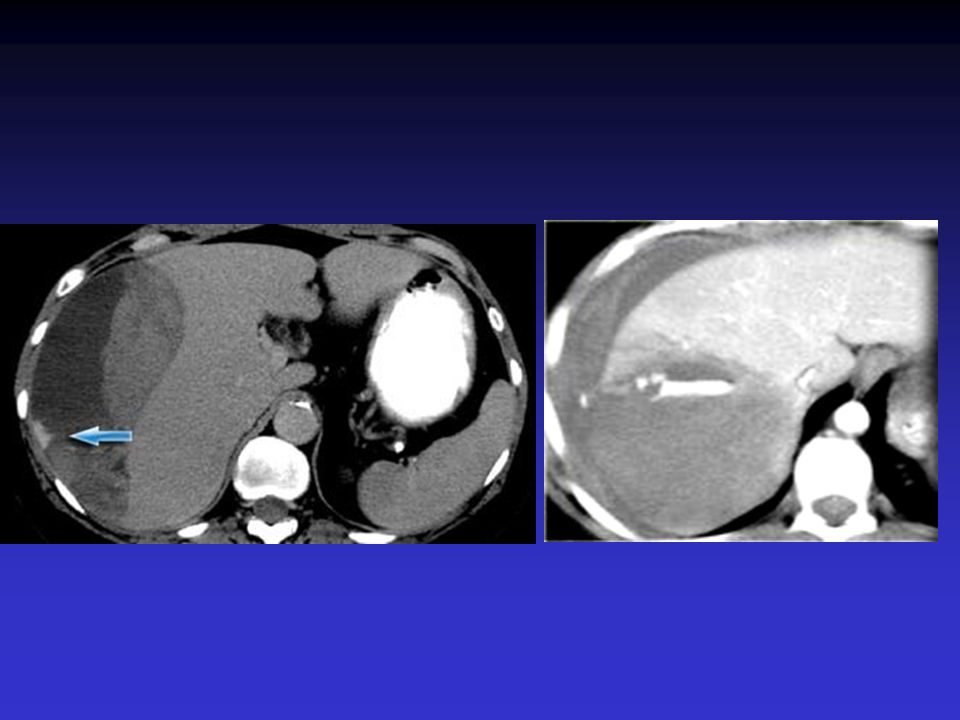
Large subcapsular hematoma
Contrast blush No hemoperitoneum … Managed non-operatively

40
Contrast extravasation is of great importance especially if it is associated with hemoperitoneum

42
Splenic contusion with contrast blush

43
Laceration hematoma

44
Lacerations Hematoma Hemoperitoneum Contrast blush Managed operatively

45
Avulsed Rt hepatic vein
Perforated duodenum

46
Pancreas

47
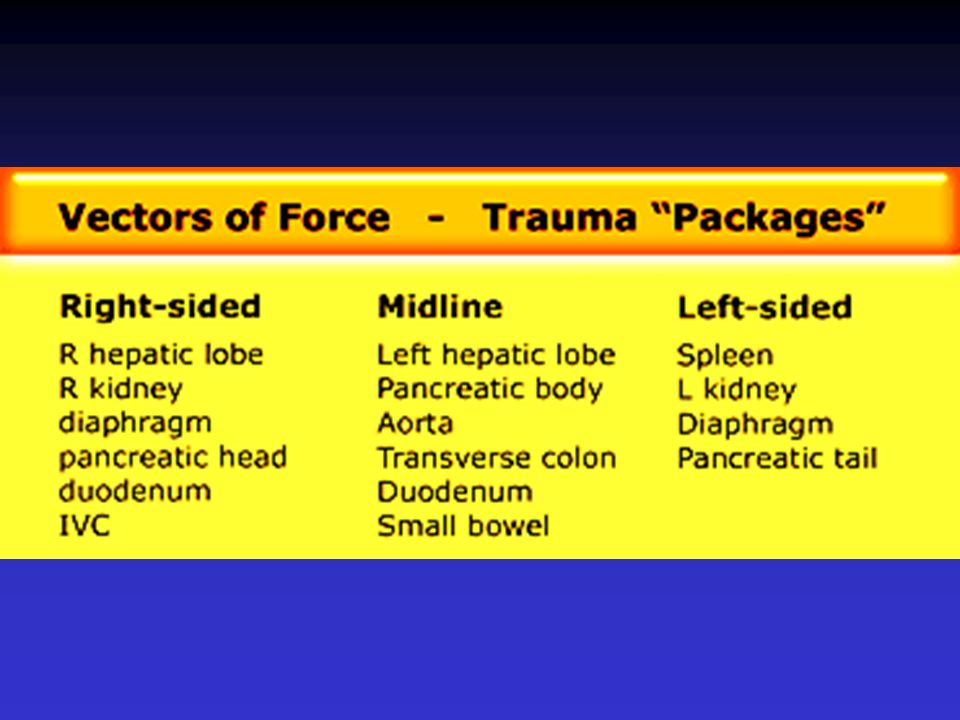
Pancreatic injury Rarely an isolated injury, since the pancreas is protected by the liver, spleen and the bony thorax Usually part of a” package injury “

49
Isolated injury

50
Left sided package injury

51
Rt sided package injury

52
Bowel injury

53
Diagnostic signs of bowel injury
Specific findings - Oral CM extravasation ………. RARE….. 0 – 19 %

54
Most common findings - unexplained intraperitoneal fluid … 84 % - pneumoperitoneum … 50 %

55
Other findings - mesenteric stranding - bowel wall thickening : * diffuse : hypoperfusion * focal : direct trauma

57
Hypovolemia “ shock bowel syndrome “ “ hypoperfusion complex “
Thickened , enhanced small bowel mucosa Enhanced adrenal glands Enhanced pancreas Non enhanced spleen Non enhanced kidneys Small IVC Small aorta and mesenteric arteries

58
However, if the CT is negative for gut injury in the face of a high clinical suspicion, laparoscopy, surgical exploration, or a period of observation plus repeat CT may be used to further evaluate the patient [62-64].
![However, if the CT is negative for gut injury in the face of a high clinical suspicion, laparoscopy, surgical exploration, or a period of observation plus repeat CT may be used to further evaluate the patient [62-64].](http://slideplayer.com/slide/9343328/28/images/58/However%2C+if+the+CT+is+negative+for+gut+injury+in+the+face+of+a+high+clinical+suspicion%2C+laparoscopy%2C+surgical+exploration%2C+or+a+period+of+observation+plus+repeat+CT+may+be+used+to+further+evaluate+the+patient+%5B62-64%5D..jpg "However, if the CT is negative for gut injury in the face of a high clinical suspicion, laparoscopy, surgical exploration, or a period of observation plus repeat CT may be used to further evaluate the patient [62-64].")
59
Thickened , enhanced small bowel mucosa

60
Hypodense spleen Hypodense kidneys Enhanced adrenals

61
Hypodense spleen Small IVC Small bowel mucosal enhancement

63
Management

64
Advantages of CT Decide whether a patient needs
- urgent therapeutic surgury * active hemorrhage * gut perforation - therapeutic angiography + embolization * active vascular hemorrhage - non-surgical management

65
Historically liver injury was managed surgically, but at laparotomy it was found that 70% of the bleedings had already stopped by the time the surgeons got there Patients who went for surgery had more transfusions and more complications than patients who were treated non-operatively

66
Today 80% are managed non-operatively

67
Nowadays there is a trend towards non-operative management of blunt abdominal trauma. More than 50% of splenic injury, 80% of liver injury and virtually all renal injuries are managed non-operatively, because patients proved to have better outcomes on the long term related to visceral salvage.

68
Conclusion

69
Categories of blunt abdominal trauma
Category A - hemodynamically unstable patients * no radiological imaging Category B - hemodynamically stable patients * CT – if high suspicion * US – if low suspicion Category C - patients with hematuria * CT cystography

70
CT protocol No oral contrast Venous phase ----- 70 sec
Delayed scan if injury present min

71
CT is used to evaluate patients with blunt trauma not only initially, but also for follow up, when patients are treated non-operatively.

72
References

73
1. Pachter HL, Knudson MM, Esrig B, et al
1. Pachter HL, Knudson MM, Esrig B, et al. Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996; 40(1):31-38. 2. Croce MA, Fabian TC, Menke PG, et al. Nonoperative management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients. Results of a prospective trial. Ann Surg 1995; 221(6): 3. Garber BG, Yelle JD, Fairfull-Smith R, et al. Management of splenic injuries in a Canadian trauma centre. Can J Surg 1996; 39(6): 4. Shanmuganathan K. Multi-detector row CT imaging of blunt abdominal trauma. Semin Ultrasound CT MR 2004; 25(2): 5. Poletti PA, Mirvis SE, Shanmuganathan K et al. CT criteria for management of blunt liver trauma: correlation with angiographic and surgical findings. Radiology 2000; 216(2): 6. Maull KI. Current status of nonoperative management of liver injuries. World J Surg 2001; 25(11):
: Croce MA, Fabian TC, Menke PG, et al. Nonoperative management of blunt hepatic trauma is the treatment of choice for hemodynamically stable patients. Results of a prospective trial. Ann Surg 1995; 221(6): Garber BG, Yelle JD, Fairfull-Smith R, et al. Management of splenic injuries in a Canadian trauma centre. Can J Surg 1996; 39(6): Shanmuganathan K. Multi-detector row CT imaging of blunt abdominal trauma. Semin Ultrasound CT MR 2004; 25(2): Poletti PA, Mirvis SE, Shanmuganathan K et al. CT criteria for management of blunt liver trauma: correlation with angiographic and surgical findings. Radiology 2000; 216(2): Maull KI. Current status of nonoperative management of liver injuries. World J Surg 2001; 25(11):")
74
7. Delgado Millan MA, Deballon PO
7. Delgado Millan MA, Deballon PO. Computed tomography, angiography, and endoscopic retrograde cholangiopancreatography in the nonoperative management of hepatic and splenic trauma. World J Surg 2001; 25(11): 8. Toutouzas KG, Karaiskakis M, Kaminski A, Velmahos GC. Nonoperative management of blunt renal trauma: a prospective study. Am Surg 2002; 68(12): 9. Smith JK, Kenney PJ. Imaging of renal trauma. Radiol Clin North Am 2003; 41(5): 10. Feliciano DV. Diagnostic modalities in abdominal trauma. Peritoneal lavage, ultrasonography, computed tomography scanning, and arteriography. Surg Clin North Am 1991; 71(2):241-
: Toutouzas KG, Karaiskakis M, Kaminski A, Velmahos GC. Nonoperative management of blunt renal trauma: a prospective study. Am Surg 2002; 68(12): Smith JK, Kenney PJ. Imaging of renal trauma. Radiol Clin North Am 2003; 41(5): Feliciano DV. Diagnostic modalities in abdominal trauma. Peritoneal lavage, ultrasonography, computed tomography scanning, and arteriography. Surg Clin North Am 1991; 71(2):241-")
75
11. Gay SB, Sistrom CL. Computed tomographic evaluation of blunt abdominal trauma. Radiol Clin North Am 1992; 30(2): 12. Wherrett LJ, Boulanger BR, McLellan BA, et al. Hypotension after blunt abdominal trauma: the role of emergent abdominal sonography in surgical triage. J Trauma 1996; 41(5): 13. McGahan JP, Rose J, Coates TL, et al. Use of ultrasonography in the patient with acute abdominal trauma. J Ultrasound Med 1997; 16(10): 14. Healey MA, Simons RK, Winchell RJ, et al. A prospective evaluation of abdominal ultrasound in blunt trauma: is it useful? J Trauma 1996; 40(6): 15. Nordenholz KE, Rubin MA, Gularte GG, Laing HK. Ultrasound in the evaluation and management of blunt abdominal trauma. Ann Emerg Med 1997; 29(3):
: McGahan JP, Rose J, Coates TL, et al. Use of ultrasonography in the patient with acute abdominal trauma. J Ultrasound Med 1997; 16(10): Healey MA, Simons RK, Winchell RJ, et al. A prospective evaluation of abdominal ultrasound in blunt trauma: is it useful J Trauma 1996; 40(6): Nordenholz KE, Rubin MA, Gularte GG, Laing HK. Ultrasound in the evaluation and management of blunt abdominal trauma. Ann Emerg Med 1997; 29(3):")
76
16. Davis KA, Fabian TC, Croce MA, et al
16. Davis KA, Fabian TC, Croce MA, et al. Improved success in nonoperative management of blunt splenic injuries: embolization of splenic artery pseudoaneurysms. J Trauma 1998; 44(6): 17. Hagiwara A, Yukioka T, Ohata S, et al. Nonsurgical management of patients with blunt hepatic injury: efficacy of transcatheter arterial embolization. AJR 1997; 169(4): 18. Cox CS Jr, Geiger JD, Liu DC, Garver K. Pediatric blunt abdominal trauma: role of computed tomography vascular blush. J Pediatr Surg 1997; 32(8):
: Hagiwara A, Yukioka T, Ohata S, et al. Nonsurgical management of patients with blunt hepatic injury: efficacy of transcatheter arterial embolization. AJR 1997; 169(4): Cox CS Jr, Geiger JD, Liu DC, Garver K. Pediatric blunt abdominal trauma: role of computed tomography vascular blush. J Pediatr Surg 1997; 32(8):")
77
Published in 2007 in Radiology assistant

78
Thank you

Similar presentations