Download presentation
Presentation is loading. Please wait.

1
Development of Lung Cancer Staging Steven M. Keller, M.D. Director Thoracic Surgery, Weiler Hospital Professor of Cardiothoracic Surgery Albert Einstein College of Medicine Montefiore Medical Center, New York

2
Cancer Staging - Societies 1929 - League of Nations Health Organization Cancer Commission 1933 - Union Internationale Contre le Cancer (UICC) 1953 - International Commission on Stage Grouping and Presentation of Results (ICPR) at the International Congress of Radiology 1959 - American Joint Committee for Cancer staging and End Results Reporting (AJC) 1980 - name changed to American Joint Committee on Cancer (AJCC)
 International Commission on Stage Grouping and Presentation of Results (ICPR) at the International Congress of Radiology American Joint Committee for Cancer staging and End Results Reporting (AJC) name changed to American Joint Committee on Cancer (AJCC)")
3
Pierre Denoix, MD 1912-1990 L’Institut Gustave Roussy Villejuif, France Originator of TNM Classification

4
Premises of TNM Staging TNM reflects the three significant events in cancer growth –Local Tumor Growth (T) –Spread to Regional Lymph Nodes (N) –Distant Metastases (M)
 –Spread to Regional Lymph Nodes (N) –Distant Metastases (M)")
5
Objectives of the TNM Classification Aid the clinician in planning treatment Give some indication of prognosis Assist in evaluating the results of treatment Facilitate the exchange of information between treatment centers Contribute to continuing investigations of human malignancies

6
History of TNM Staging 1954: UICC TNM Committee formed 1958-1967 UICC TNM Committee proposes classifications for 23 body sites 1976: AJC National Cancer Conference on Classification and Staging 1977: AJC Cancer Staging Manual (1 st Edition) 1990: American College of Surgeons Commission on Cancer mandates use of AJCC- TNM Staging System for all approved Hospitals 2002: AJCC Cancer Staging Manual (6th Edition) 2009: AJCC Cancer Staging Manual (7th Edition)
 1990: American College of Surgeons Commission on Cancer mandates use of AJCC- TNM Staging System for all approved Hospitals 2002: AJCC Cancer Staging Manual (6th Edition) 2009: AJCC Cancer Staging Manual (7th Edition)")
7
Staging Systems Other Than TNM Surveillance Epidemiology and End Results (SEER) 1973 - Established by the National Cancer Institute following the passage of the National Cancer Act of 1971 Goals –Collect complete and accurate data on all cancers diagnosed among residents of geographic areas covered by SEER cancer registries –Periodically report on the cancer burden as it relates to cancer incidence and mortality, and patient survival overall and in selected segments of the population
 Established by the National Cancer Institute following the passage of the National Cancer Act of 1971 Goals –Collect complete and accurate data on all cancers diagnosed among residents of geographic areas covered by SEER cancer registries –Periodically report on the cancer burden as it relates to cancer incidence and mortality, and patient survival overall and in selected segments of the population")
8
Staging Systems Other Than TNM Surveillance Epidemiology and End Results (SEER) Goals –Identify unusual changes and differences in the patterns of occurrence of specific forms of cancer in population subgroups defined by geographic, demographic, and social characteristics –Describe temporal changes in cancer incidence, mortality, extent of disease at diagnosis (stage), therapy, and patient survival as they may relate to the impact of cancer prevention and control interventions. –Monitor the occurrence of possible iatrogenic cancers, i.e., cancers that are caused by cancer therapy

9
SEER Data- Source and Accuracy 18 population based cancer registries 26% U.S. population Reflects 2000 census with regard to: race, ethnicity, income, etc Regular audits and training

10
SEER Summary Stage Developed 1977 Single digit definition Less complex Developed for registrars and epidemiologists who want some information, but did not wish to collect the more detailed Extent of Disease or TNM data Utilizes best data available: clinical, radiologic, pathologic

11
SEER Summary Stage Definitions –In Situ (0) –Localized only (1) –Regional Direct extension only (2) Lymph nodes only (3) Both direct extension and lymph nodes (4) Not otherwise specified (5) –Distant organs or non-regional lymph nodes (7) –Unknown (9)
 –Localized only (1) –Regional Direct extension only (2) Lymph nodes only (3) Both direct extension and lymph nodes (4) Not otherwise specified (5) –Distant organs or non-regional lymph nodes (7) –Unknown (9)")
12
SEER Extent of Disease Developed 1977 to assure consistency over time as other staging systems changed Allow data to collapse into different and previous staging systems Utilizes best data available: clinical, radiologic, pathologic Five field, ten digit system –Tumor size (three digits) –Regional lymph node involvement (one digit) –Number of pathologically reviewed lymph nodes that contain tumor (two digits) –Number of pathologically examined regional lymph nodes (two digits)
 –Regional lymph node involvement (one digit) –Number of pathologically reviewed lymph nodes that contain tumor (two digits) –Number of pathologically examined regional lymph nodes (two digits)")
13
Staging Systems Other Than TNM Collaborative Staging Designed to bring together the TNM, Summary Stage, and Extent of Disease coding structures Initiated in 2004 9 data fields, 16 digits 5 additional site specific data fields Utilizes best data available: clinical, radiologic or pathologic

14
Collaborative Staging Definitions –Tumors size (three digits) –Tumor extension (two digits) –Method by which size and extension determined (one digit) –Regional lymph nodes (two digits) –Method by which regional lymph node involvement determined (one digit) –Number of pathologically reviewed lymph nodes that contained tumor (two digits) –Number of pathologically examined regional lymph nodes (two digits) –Metastases at diagnosis (two digits) –Method by which metastases determined (one digit)
 –Tumor extension (two digits) –Method by which size and extension determined (one digit) –Regional lymph nodes (two digits) –Method by which regional lymph node involvement determined (one digit) –Number of pathologically reviewed lymph nodes that contained tumor (two digits) –Number of pathologically examined regional lymph nodes (two digits) –Metastases at diagnosis (two digits) –Method by which metastases determined (one digit)")
15
Collaborative Staging

16
Lung Cancer Staging/Treatment The Early Years 1933 - ~1974 Surgery only potentially curative modality Cancer spreads in an orderly fashion from primary site to region lymph nodes and then to distant sites

17
Authors initially reported survival with and without tumor in lymph nodes Gradual recognition that the presence of disease in the “mediastinal” nodes had a worse prognosis than metastases in the “hilar” nodes No mention of tumor size, local invasion No mention of which lymph node involved Discussion regarding surgery if mediastinal disease present Lung Cancer Staging/Treatment The Early Years 1933 - ~1974

18
Am J Radiol 1974;120;130-8 Task Force on Lung Cancer of the American Joint Committee on Cancer Staging and End Reporting

19
Am J Radiol 1974;120;130-8 TNM Staging - 1st Edition Definitions and Groupings N descriptor –N0 no regional nodal metastases –N1 metastases to ipsilateral hilar nodes –N2 metastases to mediastinal nodes T descriptor –T 0 no evidence tumor –T X malignant cells but tumor not seen –T1 < 3cm, no visceral pleural involvement, distal to lobar bronchus –T2 > 3cm or involves visceral pleura, proximal to bronchus. > 2 c from carina, no effusion, atelectasis < entire lung –T3 direct extension to adjacent organs, < 2 cm from carina, atelectasis entire lung M descriptor –M0 no distant metastases –M1 distant metastases such as scale, cervical, contralateral hilar nodes, solid organs

20
Am J Radiol 1974;120;130-8 Survival Utilizing Clinical TNM 2,155 patients –996 squamous –521 adenocarcinoma –195 large cell –368 small cell –75 undifferentiated All small cell cases placed in stage 3 T – 5 categories (T0-T3) N – 3 categories (N0-N2) M – 2 categories (M0-M1) Stages – 3 (I-III)
 N – 3 categories (N0-N2) M – 2 categories (M0-M1) Stages – 3 (I-III)")
21
Survival Utilizing Clinical TNM Am J Radiol 1974;120;130-8 *Small cell excluded

22
Chest 1986;89:225S-33 Unified UICC/AJCC TNM Stage 1986 Need for refinement recognized New categories created and grouping altered T – 7 categories (TX-T4) N – 4 categories (N0-N3) M – 2 categories (M0-M1) Stages – 7 (Occult carcinoma - IV)
 N – 4 categories (N0-N3) M – 2 categories (M0-M1) Stages – 7 (Occult carcinoma - IV)")
23
Unified UICC/AJCC TNM Stage 1986 3,753 patients –2,749 MD Anderson –1004 LCSG Chest 1986;89:225S-33

24
Chest 1997;111:1710-7 Unified UICC/AJCC TNM Stage 1997 Need for refinement recognized New categories created and grouping altered T – 7 categories (TX-T4) N – 5 categories (NX-N3) M – 3 categories (MX-M1) Stage groupings – 8 (O - IV)
 N – 5 categories (NX-N3) M – 3 categories (MX-M1) Stage groupings – 8 (O - IV)")
25
Lung Cancer: A Handbook for Staging, Imaging and Lymph Node Classification. Mountain 1999 Unified UICC/AJCC TNM Stage 1997 Survival Clinical Stage 5,319 patients –4351 MD Anderson –968 LCSG

26
Revisions of the TNM Stage Groupings for the Seventh Edition of the TNM Classification 1998 International Association for the Study of Lung Cancer (IASLC) established Lung Cancer Staging Project Supported by the UICC and AJCC Data collected from 45 institutions in 20 countries on four continents Patients treated between 1990-2000 J Thorac Oncol 2006;1:281-6
 established Lung Cancer Staging Project Supported by the UICC and AJCC Data collected from 45 institutions in 20 countries on four continents Patients treated between J Thorac Oncol 2006;1:281-6")
27
Revisions of the TNM Stage Groupings for the Seventh Edition of the TNM Classification Total cases submitted 100,869 Included in analysis 81,015 Non-small cell lung cancer 67,725 Small cell lung cancer 13,290 New categories created and grouping altered T – 11 categories (TX-T4) N – 5 categories (NX-N3) M – 5 categories (MX-M2) Stage groupings – 8 (O - IV) J Thorac Oncol 2007;2:706-14
 N – 5 categories (NX-N3) M – 5 categories (MX-M2) Stage groupings – 8 (O - IV) J Thorac Oncol 2007;2:706-14")
28
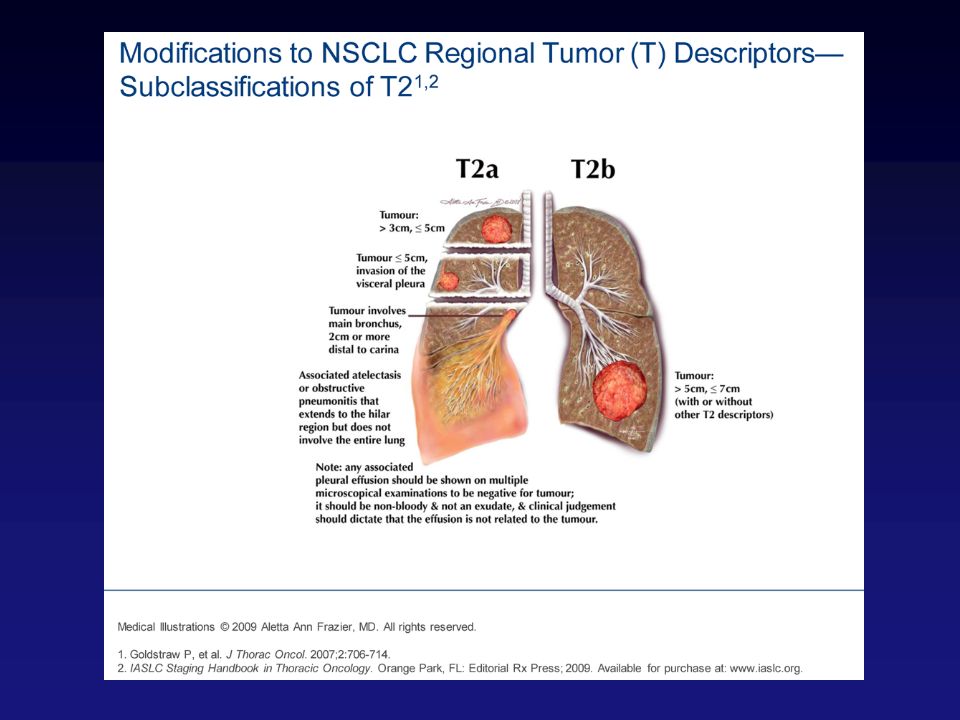
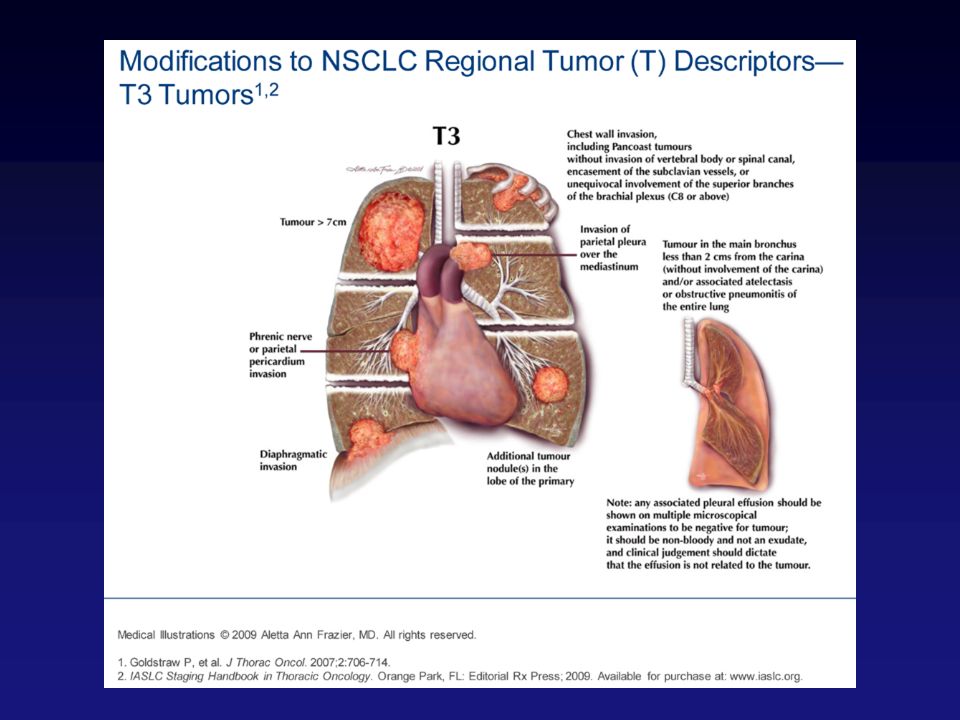
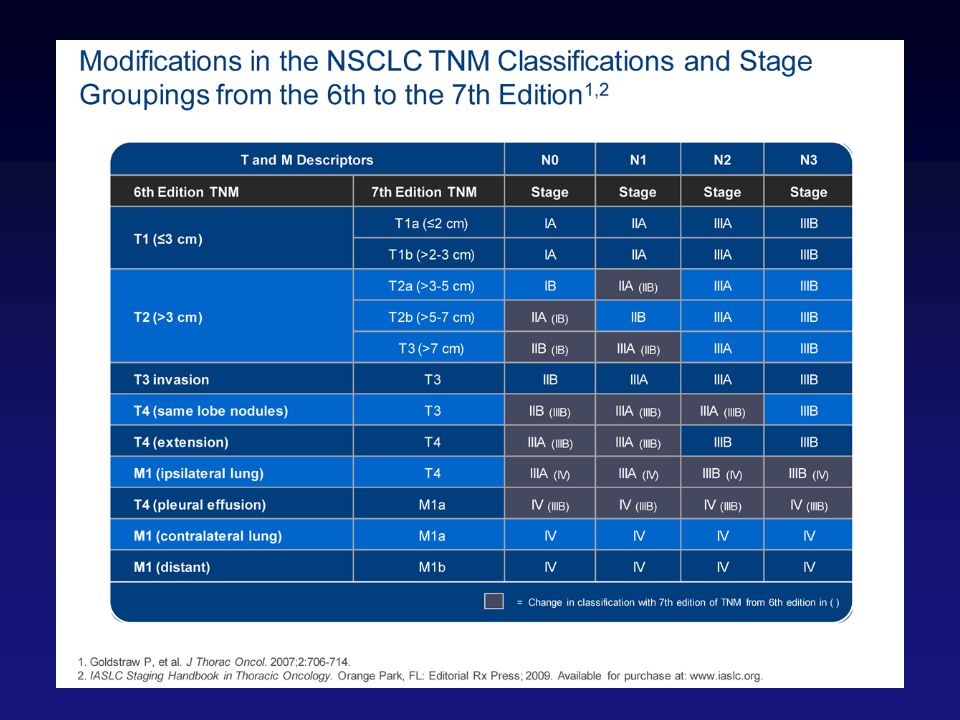
Revisions of the T Descriptor T1 tumors divided into: –T1a (< 2cm in greatest dimension) –T1b (>2cm<3cm in greatest dimension) T2 tumors divided into: –T2a (>3cm<5cm in greatest dimension) –T2b (>5cm<7cm in greatest dimension) Tumors >7cm in greatest dimension added to the T3 category J Thorac Oncol 2007;2:593-602
 –T1b (>2cm<3cm in greatest dimension) T2 tumors divided into: –T2a (>3cm<5cm in greatest dimension) –T2b (>5cm<7cm in greatest dimension) Tumors >7cm in greatest dimension added to the T3 category J Thorac Oncol 2007;2:")
29
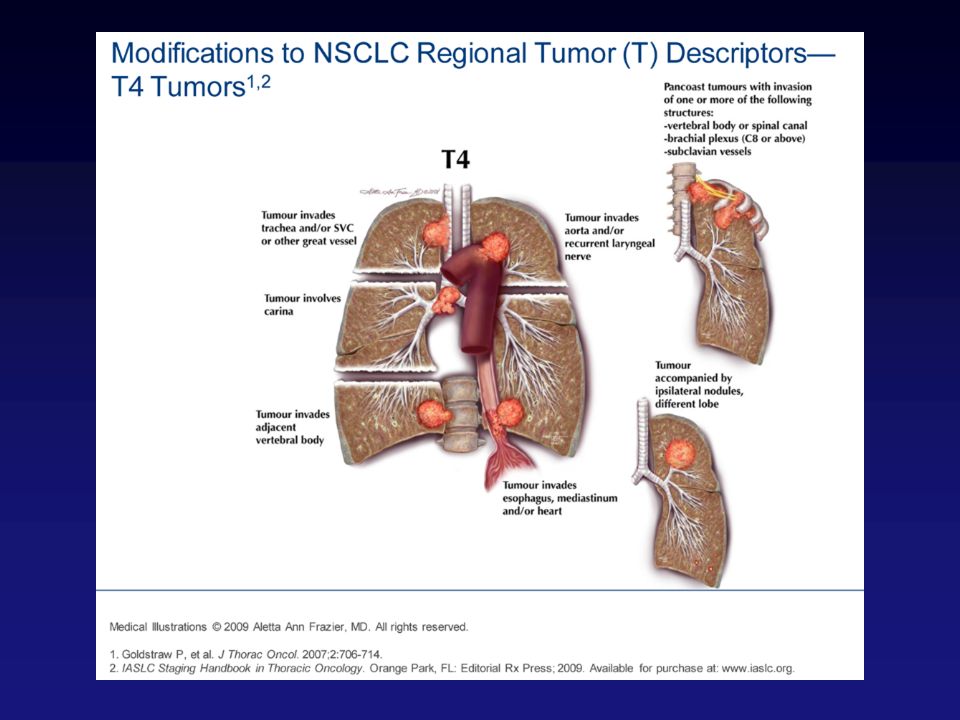
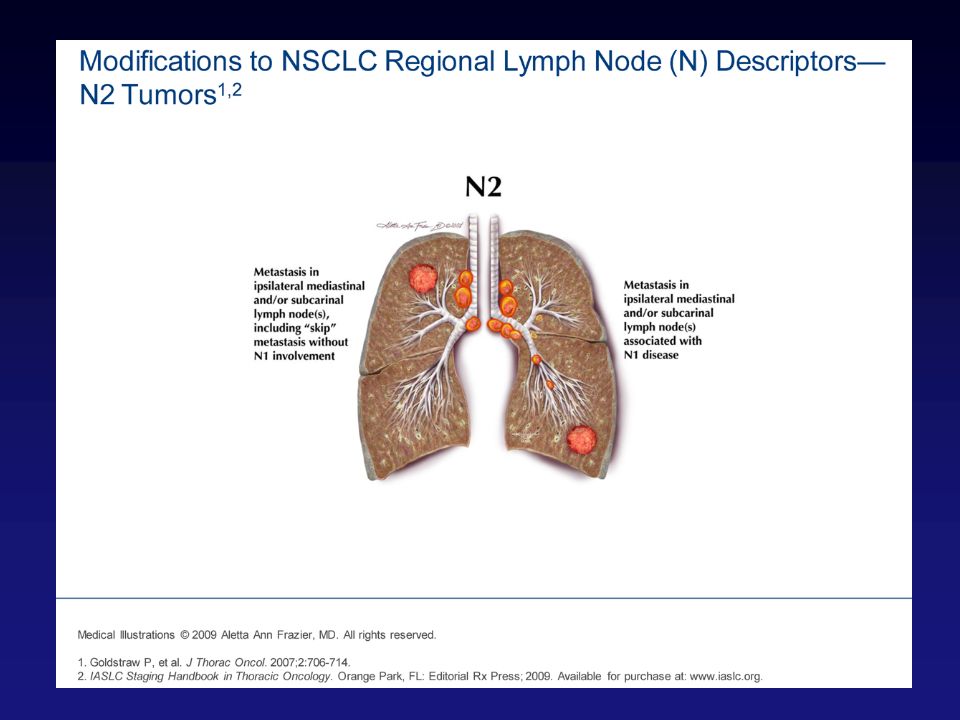
Revisions of the T Descriptor Satellite nodules in the same lobe moved to T3 (previously T4) Metastases in other ipsilateral lobes moved to T4 (previously M1) Pleural metastases (malignant pleural or pericardial effusions, pleural nodules) moved to M1a (previously T4) J Thorac Oncol 2007;2:593-602
 Metastases in other ipsilateral lobes moved to T4 (previously M1) Pleural metastases (malignant pleural or pericardial effusions, pleural nodules) moved to M1a (previously T4) J Thorac Oncol 2007;2:")
34
Japanese Nodal Definitions JTCVS 1978;76:832-39 Tsuguo Naruke, MD

35
Mountain Dresler Lymph Node Map Level 4R superior Level 4R inferior Level 12R Level 10R Level 11R Level 2RLevel 2L Level 4L Level 10L Level 8L Level 9L Chest 1997;111:17178-23

36
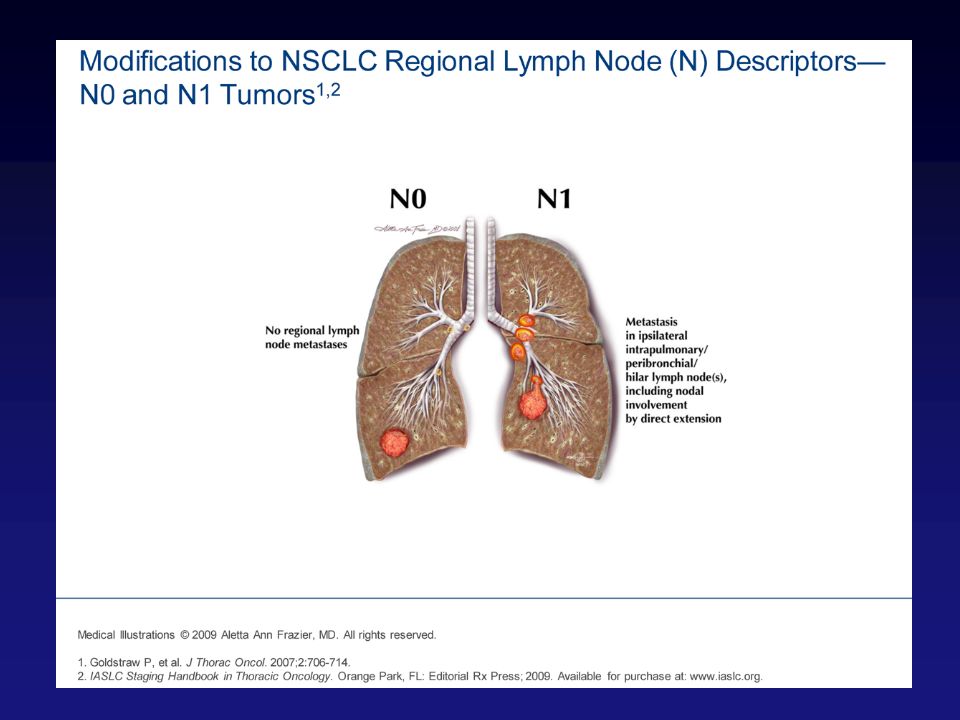
No change in descriptors Zones consisting of multiple levels correlate with survival ? Define N by zone or combination of zones J Thorac Oncol 2007;2:603-12 Revisions of the N Descriptor Hilar zone Lower zone Upper zone (R) AP Zone (L) Peripheral zone Subcarinal zone
 AP Zone (L) Peripheral zone Subcarinal zone.")
40
M1a –Pleural metastases (malignant pleural or pericardial effusions, pleural nodules) (previously T4) –Metastases in the contralateral lung M1b –Distant metastases (outside lung and pleura) J Thorac Oncol 2007;2:686-93 Revisions of the M Descriptor
 (previously T4) –Metastases in the contralateral lung M1b –Distant metastases (outside lung and pleura) J Thorac Oncol 2007;2: Revisions of the M Descriptor")
43
T2aN1 now IIA (changed from IIB) T2bN0 now stage IIA (changed from IB) T4N0 and T4N1 now IIIA (changed from IIIB) J Thorac Oncol 2007;2:706-14 Revisions of the Stage Groupings
 T2bN0 now stage IIA (changed from IB) T4N0 and T4N1 now IIIA (changed from IIIB) J Thorac Oncol 2007;2: Revisions of the Stage Groupings")
45
Staging - Special Circumstances Visceral pleural involvement – at least T2a Multiple synchronous tumors in single organ – stage most advanced and indicate multiple in parenthesis ex: T2a(2)N0 Multiple synchronous tumors in paired organ – stage and report independently
N0 Multiple synchronous tumors in paired organ – stage and report independently")
46
Staging - Special Circumstances Lymph node replacement – use best judgment Lymph node direct extension – stage as metastatic disease Lymph node disease < 2mm classify as pN0 Doubt – use lower stage Recurrent nerve injury – nodes (N2) vs primary (T4)
 vs primary (T4)")
47
Clinical Stage - Definition Information obtained prior to instituting therapy or within 4 months of diagnosis, whichever is shorter Includes: –Physical exam –Radiology –Laboratory –Biopsy: any type, any method

48
Clinical Staging - Definition Clinical T – includes any biopsy and even surgical exploration without resection, unless the biopsy proves the highest T category (T4) Clinical N - In the absence of pT, excision of single or sentinel node is cN Clinical Stage –Absence of pT and pN –Absence of pM1
 Clinical N - In the absence of pT, excision of single or sentinel node is cN Clinical Stage –Absence of pT and pN –Absence of pM1")
49
Pathologic Staging Information about extent of cancer obtained up through completion of definitive surgery therapy or within 4 months of diagnosis, whichever is longer

50
Pathologic Staging - Definition Pathologic T –Resection –Biopsy that proves highest T category (T4) Pathologic N –Any node if, pT present –Single node, if highest category (N3) –In the absence of pT, excision of single or sentinel node is cN Pathologic Stage If both pT and pN present, M1 may be cM1 or pM1 If pM1 present, T and N may be clinical or pathologic
 Pathologic N –Any node if, pT present –Single node, if highest category (N3) –In the absence of pT, excision of single or sentinel node is cN Pathologic Stage If both pT and pN present, M1 may be cM1 or pM1 If pM1 present, T and N may be clinical or pathologic")
51
Staging- Limitations TNM was originated by a surgeon (Denoix) based on the teachings of another surgeon (Halstead) No surprise that TNM is most applicable to patients whose primary and most effective treatment is surgery TNM is a temporal model that does not take into account other factors that predict response to treatment (surgery, chemotherapy, radiotherapy, other)
 based on the teachings of another surgeon (Halstead) No surprise that TNM is most applicable to patients whose primary and most effective treatment is surgery TNM is a temporal model that does not take into account other factors that predict response to treatment (surgery, chemotherapy, radiotherapy, other)")
52
Staging: What is Needed Staging system that incorporates new information that predicts survival – Genomics – Proteomics – Immunohistochemistry

Similar presentations












 tumor and whether.>")
 M0 - No metastases M1 - Metastases present.>")









