Download presentation
Presentation is loading. Please wait.

1
Crohn Disease (Regional Enteritis)
Sammy Termanini 1490

2
Overview Life long inflammatory bowel disease
Lumen becomes swollen and develops ulcers Idiopathic cause

3
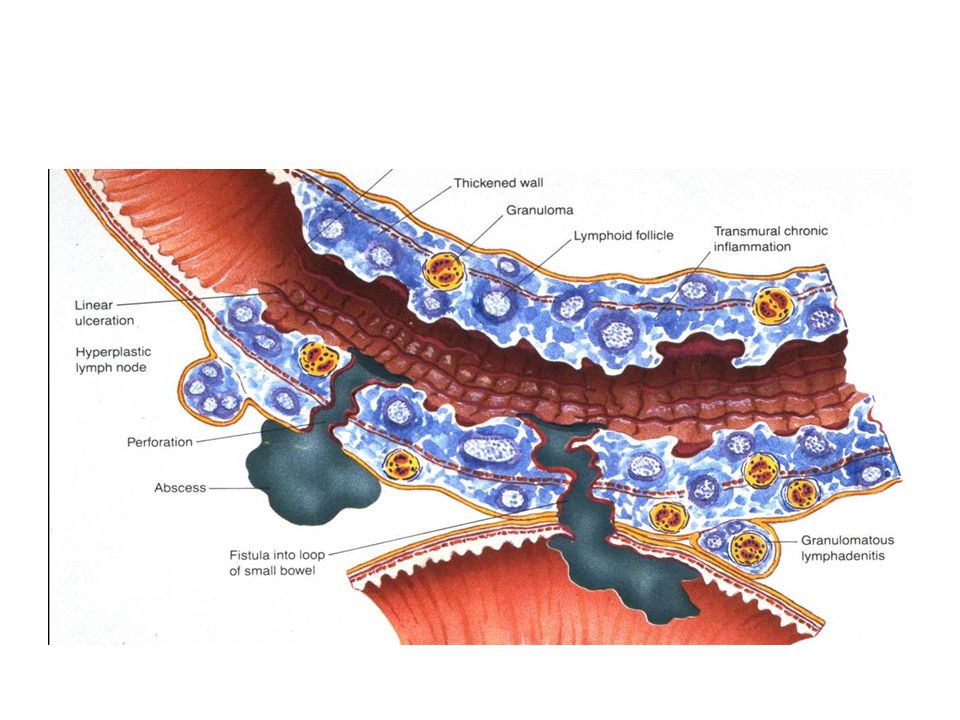
Morphology Most common sites of presentation, terminal ileum, ileocecal valve and cecum Skip lesions from apththous ulcers Cobblestone appearance from fissures between mucosal folds Intestinal wall is thickened Creeping fat

5
Microscopic Features Active infection
Abundant neutrophils that infiltrate and damage crypt epithelium or crypt abscess Distortion of of mucosal architecture Epithelial metaplasia consequence of chronic relapsing infection (pseudopyloric metaplasia) Paneth cell metaplasia in left colon, normally absent Non-caseating granulomas Absence of granulomas does not preclude diagnosis of Crohn’s Disease
 Paneth cell metaplasia in left colon, normally absent. Non-caseating granulomas. Absence of granulomas does not preclude diagnosis of Crohn’s Disease.")
6
Non-caseating Granuloma

7
Clinical Features Extremely variable
Usually begins with intermittent attacks of mild diarrhea, fever and abdominal pain 20% of cases present with right lower quadrant, fever and bloody diarrhea mimicking acute appendicitis or bowel perforation Periods of active disease interrupted by asymptomatic intervals Reactivated by physical or emotional stress, specific dietary items and cigarette smoking

8
Clinical Features Iron deficiency anemia may develop
Serum protein loss and hypoalbuminemia, generalized nutrient malabsorption, or malabsorption of vitamin B12 and bile salts. Fibrosing strictures of the terminal ileum, require surgical resection. Recurs at the site of anastomosis, and almost half require additional resections within 10 years. Fistulas develop between loops of bowel and may also involve the urinary bladder, vagina, and abdominal or perianal skin. Perforations and peritoneal abscesses are common.

9
Extraintestinal Manifestations
Uveitis, migratory polyarthritis, sacroiliitis, ankylosing spondylitis, erythema nodosum, and clubbing of the fingertips, Pericholangitis and primary sclerosing cholangitis also occur but are more common in ulcerative colitis. Risk of colonic adenocarcinoma increased in patients with long-standing Crohn disease

10
Diagnosis Medical history, physical examination, imaging tests to look at intestines and lab tests May go years without diagnosis Colonoscopy or flexible sigmoidoscopy Abdominal X-ray Upper gastrointestinal series or endoscopy CT scan MRI

11
Treatment Manage mild symptoms with antidiarrheal medicine (loperamide) Moderate symptoms use aminosalicylates ,antibiotics to control inflammation Severe symptoms treated with corticosteroids, immunomodulator medicines, or biologics. First step is to control the disease. When your symptoms are gone, your doctor will plan your treatment to keep you symptom-free (in remission). After symptoms are controlled, treatment focuses on medicine or a combination of medicines that keeps disease in remission Some severe cases of Crohn's disease need to be treated in the hospital.
. After symptoms are controlled, treatment focuses on medicine or a combination of medicines that keeps disease in remission. Some severe cases of Crohn s disease need to be treated in the hospital.")
12
References Kumar,Vinay; Abbas, Abul K.; Aster, Jon C.; Basic Pathology, Robbins; Philadelphia; Elservier Saunders;2013. Print.

Similar presentations










 Kristina Blaslov Mentor: A. Žmegač Horvat.>")






 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")

 it is a tube with muscle walls throughout its length. it is lined by an epithelium.>")