Download presentation
Presentation is loading. Please wait.

1
Benign Prostatic Hyperplasia
DR.Gehan Mohamed

2
Normal Prostate Anatomy
Prostate weights ~20g Measures ~3 by 4 by 2 cm Apex = inferior portion of prostate, continuous with striated sphincter. Base = superior portion and continuous with bladder neck.

3
PROSTATE histology Prostatic tissue is formed of two components :
fibromuscular tissue (30%) glandular epithelial cells (70%)
 glandular epithelial cells (70%)")
4
Normal histology of prostate: formed of glands and fibromuscular stroma

5
Normal histology of the prostate formed of glands and stroma glands: lined by two layers of cells which are inner cuboidal cells and outer basal cells stroma :fibro muscular stroma

6
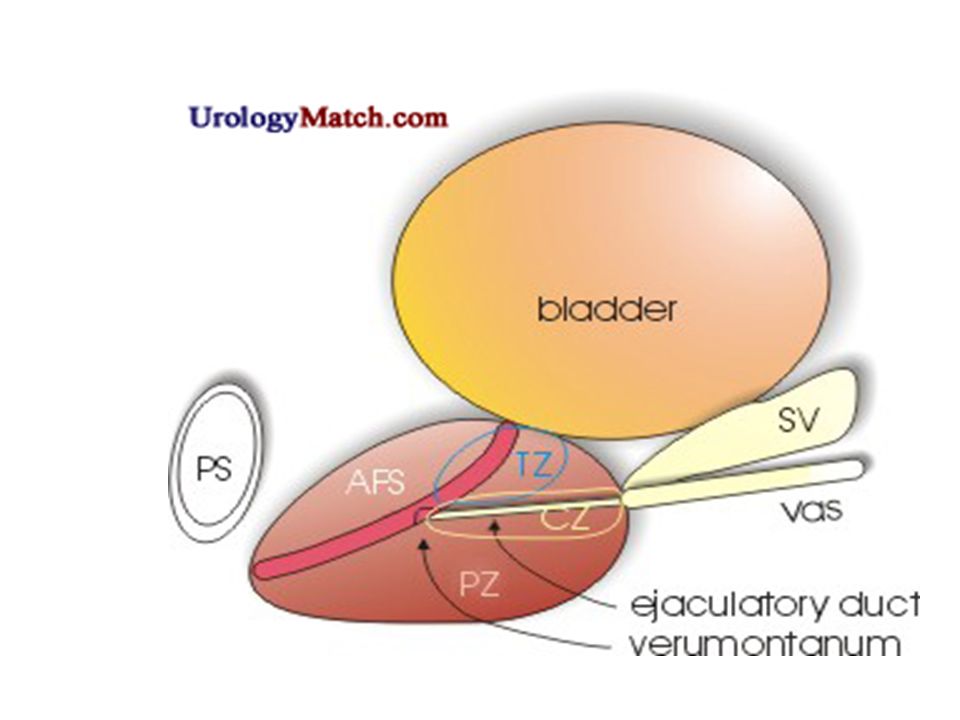
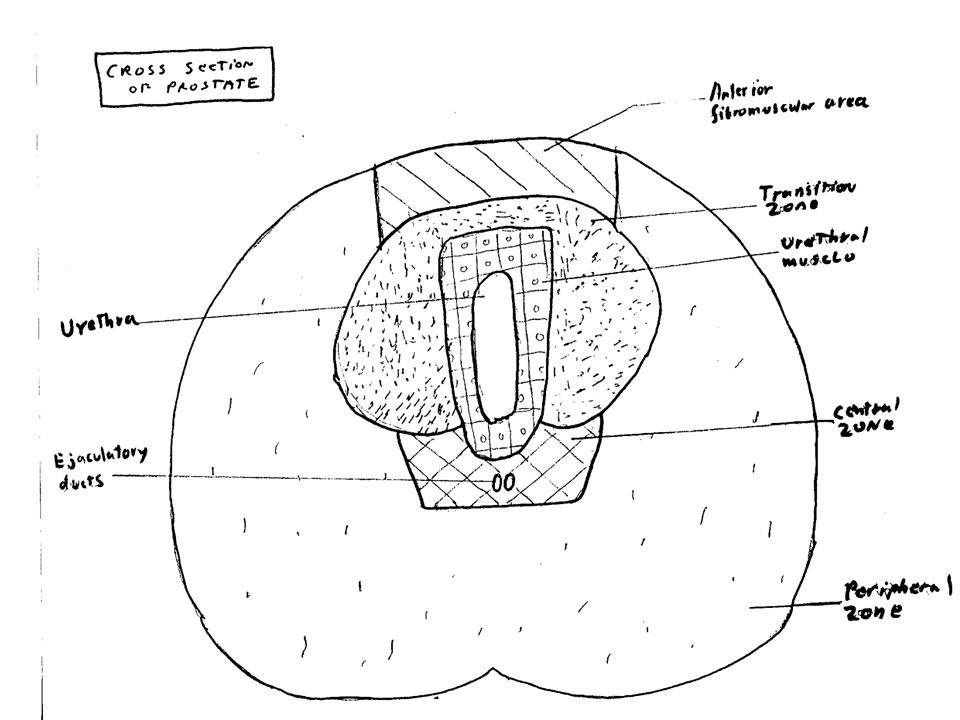
Prostate zones Central zone (CZ)
Cone shaped region that surround the ejaculatory ducts (extends from bladder base to the verumontanum) Only 1-5% of prostate cancer from this region . Peripheral zone (PZ) Posteriolateral prostate Majority of prostatic glandular tissue Origin of up to 70% of prostate adenocarcinoma Transitional zone (TZ) Surrounds the prostatic urethra Commonest site for benign prostatic hyperplasia.
 Only 1-5% of prostate cancer from this region . Peripheral zone (PZ) Posteriolateral prostate. Majority of prostatic glandular tissue. Origin of up to 70% of prostate adenocarcinoma. Transitional zone (TZ) Surrounds the prostatic urethra. Commonest site for benign prostatic hyperplasia.")
9
What causes BPH? BPH is part of the natural aging process, like getting gray hair or wearing glasses BPH cannot be prevented BPH can be treated n n n

10
Half of all men over the age of 60 will develop an enlarged prostate.
By the time men reach their 70’s and 80’s, 80% will experience urinary symptoms But only 25% of men aged 80 will be receiving BPH treatment

11
BPH Proposed Etiologies
1-alterations in the testosterone/estrogen balance:enlarged prostate may be caused by lower levels of testosterone (male hormone) production in middle to old age. As men age, the levels of testosterone in their blood decreases, leaving a higher proportion of estrogen (female hormone), so a higher amount of estrogen within the prostate gland can increase activity that promotes cell growth. 2-Induction of prostatic growth factors. 3- Increased stem cells/decreased stromal cell death
 production in middle to old age. As men age, the levels of testosterone in their blood decreases, leaving a higher proportion of estrogen (female hormone), so a higher amount of estrogen within the prostate gland can increase activity that promotes cell growth. 2-Induction of prostatic growth factors. 3- Increased stem cells/decreased stromal cell death.")
12
Benign Prostatic Hypertrophy (BPH)—Pathophysiology
Common in older men; varies from mild to severe Change is actually hyperplasia of prostate Nodules form around urethra Not change to cancer prostate. Rectal exams reveals enlarged gland Incomplete emptying of bladder leads to infections Continued obstruction leads to distended bladder, dilated ureters, renal damage If significant, surgery required

14
What’s Lower Urinary Tract Symptoms secondary to prostatic urethra obstruction?
Abnormal Voiding (obstructive) symptoms Hesitancy Weak stream Straining to pass urine Prolonged micturition Feeling of incomplete bladder emptying Urinary retention Storage (irritative or filling) symptoms Urgency:an increasingly strong desire to void) Frequency Nocturia Urge incontinence LUTS can arise from a variety of causes, for example as a consequence of prolonged urinary obstruction due to BPH. LUTS are categorised as being obstructive (voiding) or irritative (storage) symptoms. Obstructive symptoms include hesitancy, weak stream, straining to pass urine, prolonged micturition, feeling of incomplete bladder emptying, and urinary retention. Irritative symptoms include urgency, frequency, nocturia, and urge incontinence. LUTS may also be due to inflammatory or infectious processes. LUTS is not specific to BPH – not everyone with LUTS has BPH and not everyone with BPH has LUTS
 symptoms. Hesitancy. Weak stream. Straining to pass urine. Prolonged micturition. Feeling of incomplete bladder emptying. Urinary retention. Storage (irritative or. filling) symptoms. Urgency:an increasingly strong desire to void) Frequency. Nocturia. Urge incontinence. LUTS can arise from a variety of causes, for example as a consequence of prolonged urinary obstruction due to BPH. LUTS are categorised as being obstructive (voiding) or irritative (storage) symptoms. Obstructive symptoms include hesitancy, weak stream, straining to pass urine, prolonged micturition, feeling of incomplete bladder emptying, and urinary retention. Irritative symptoms include urgency, frequency, nocturia, and urge incontinence. LUTS may also be due to inflammatory or infectious processes. LUTS is not specific to BPH – not everyone with LUTS has BPH and not everyone with BPH has LUTS.")
15
BPH—Signs and Symptoms
Initial signs Obstruction of urine flow Hesitancy : delay between trying to urinate and the flow actually beginning. dribbling decreased force of urine stream Incomplete bladder emptying Frequency, nocturia : need to urinate at night recurrent Urinary Tract Infections

16
BPH complications hypertrophy of the prostatedetrussor muscle of the bladder undergo hypertrophy to overcome the obstruction in the prostatic urethra. Later on decompensation occur . Increase pressure inside bladderdiverticula formationincreasing urine retentionhydronephrosis renal failure.

17
Diverticula in bladder

19
Diagnosis of BPH Symptom assessment Digital rectal examination(DRE)
inaccurate for size but can detect shape and consistency Prostate Volume (PV) determination by ultrasonography Urodynamic analysis Measurement of prostate-specific antigen (PSA) high correlation between PSA and PV, men with larger prostates have higher PSA levels PSA is a predictor of disease progression and screening tool for Cancer Prostate. as PSA values tend to increase with increasing Prostatic Volume and increasing age, PSA may be used as a prognostic marker for BPH. The initial evaluation can be done either by a Primary Care Practitioner (PCP) or by a urologist. If the initial evaluation suggests a diagnosis of BPH, the physician can proceed to develop an appropriate treatment plan. The physical examination should include specific attention to the presence or absence of a distended bladder, urethral discharge, genital abnormalities, and neurologic abnormalities that can affect voiding. A digital rectal examination (DRE) is considered an important part of the physical examination of any patient complaining of symptoms of prostatism. This examination is conducted with a well-lubricated, gloved index finger, which is used to palpate the prostate gland and the surrounding tissues through the wall of the rectum. Because of the prevalence of prostatic disease in older men, many physicians conduct DREs as part of the routine annual physical examination of any man over the age of 50 years. The size, consistency, shape, and symmetry of the prostate gland can be felt through the rectal wall during a DRE. Several questionnaires are used to assess the severity of symptoms and their impact on a patient’s QoL. American Urology Association-Symptom Score (AUA-SI) or International Prostate Symptom Score (IPSS), QoL score and BPH-II. In men with symptoms of BPH, a urine sample should be examined for signs of a urinary tract infection or haematuria, both of which suggest a non-BPH cause for the LUTS. Both urinary tract infections and bladder cancer can produce symptoms similar to those produced by BPH.
 determination by ultrasonography. Urodynamic analysis. Measurement of prostate-specific antigen (PSA) high correlation between PSA and PV, men with larger prostates have higher PSA levels. PSA is a predictor of disease progression and screening tool for Cancer Prostate. as PSA values tend to increase with increasing Prostatic Volume and increasing age, PSA may be used as a prognostic marker for BPH. The initial evaluation can be done either by a Primary Care Practitioner (PCP) or by a urologist. If the initial evaluation suggests a diagnosis of BPH, the physician can proceed to develop an appropriate treatment plan. The physical examination should include specific attention to the presence or absence of a distended bladder, urethral discharge, genital abnormalities, and neurologic abnormalities that can affect voiding. A digital rectal examination (DRE) is considered an important part of the physical examination of any patient complaining of symptoms of prostatism. This examination is conducted with a well-lubricated, gloved index finger, which is used to palpate the prostate gland and the surrounding tissues through the wall of the rectum. Because of the prevalence of prostatic disease in older men, many physicians conduct DREs as part of the routine annual physical examination of any man over the age of 50 years. The size, consistency, shape, and symmetry of the prostate gland can be felt through the rectal wall during a DRE. Several questionnaires are used to assess the severity of symptoms and their impact on a patient’s QoL. American Urology Association-Symptom Score (AUA-SI) or International Prostate Symptom Score (IPSS), QoL score and BPH-II. In men with symptoms of BPH, a urine sample should be examined for signs of a urinary tract infection or haematuria, both of which suggest a non-BPH cause for the LUTS. Both urinary tract infections and bladder cancer can produce symptoms similar to those produced by BPH.")
20
BPH : show marked hyperplasia in the number of prostatic glands

21
When should BPH be treated?
BPH needs to be treated ONLy IF: Symptoms are severe enough to bother the patient and affect his quality of life Complications related to BPH n n

22
Treatment options 1- Transurethral resection of the prostate (TURP)
Medication :α blockers - relax the smooth muscle of prostate and provide a larger urethral opening Surgical approaches 1- Transurethral resection of the prostate (TURP) 2- Open simple prostatectomy n n n
 2- Open simple prostatectomy. n. n. n.")
23
Indication of surgical intervention
Acute urinary retention Gross hematuria Frequent urinary tract infection (UTI) Vesical stone BPH related hydronephrosis or renal function deterioration Obstruction
 Vesical stone. BPH related hydronephrosis or renal function deterioration. Obstruction.")
24
Differential Diagnosis of BPH(i
Differential Diagnosis of BPH(i.e from other causes of urinary obstruction) Urethral stricture Bladder neck contracture Carcinoma of the prostate Carcinoma of the bladder Bladder calculi Urinary tract infection and prostatitis Neurogenic bladder
 Urethral stricture. Bladder neck contracture. Carcinoma of the prostate. Carcinoma of the bladder. Bladder calculi. Urinary tract infection and prostatitis. Neurogenic bladder.")
25
Thanks for Your Attention!

Similar presentations



 Bob White, AIM-IRS ABMTS Milwaukee, WI.>")













 in men Kamal Patel GPST2.>")



