Download presentation
Presentation is loading. Please wait.

1
CURRENT ISSUES IN TB (& HIV) Marc Lipman 8 September 2011
 Marc Lipman 8 September 2011")
2
Headlines 9 million new cases of active TB each year 12% HIV co-infected –80% from sub-Saharan Africa or SE Asia TB rate increased 2-3x in high HIV sSA TB/HIV morbidity and economic cost huge but unknown TB responsible for 25% of all HIV-related deaths

3
HIV prevalence in new active TB cases, 2007 WHO, 2009

4
Areas we will cover Latency Screening Treatment of LTBI When to start ART IRIS

5
NATURAL HISTORY OF TB & WHY HIV IS SUCH A PROBLEM Exposure 70% no infection30% infection EarlyContainment progressors (60-95%) (1-2 years) LateNil HIV : 2-5%HIV : 40% progressors HIV : 5% lifetime riskHIV : 3-14%/year Glynn AIDS 2008;22:1859
 (1-2 years) LateNil HIV : 2-5%HIV : 40% progressors HIV : 5% lifetime riskHIV : 3-14%/year Glynn AIDS 2008;22:1859")
6
Risk factors for active TB/HIV Injecting drug users vs MSM Heterosexuals vs MSM From TB endemic country ? Reported previous TB Advanced clinical stage of disease Low blood CD4 count Not on ART Badri. Lancet 2002;359:2059 Girardi. CID 2005;41:1772 Seyler. AJCCRM 2005;172:123

7
What history tells us TB cannot be controlled if there is uncontrolled HIV infection ART is associated with ~60-90% in active TB Possible in active TB during initial 3 months of ART Developing world: 10,000 – 23,000/100,000 Developed world: 1300 - 1700 /100,000 Need to develop strategies to screen for TB pre ART

8
What is clinical latency?

9
The spectrum of tuberculosis Barry CE. Nat Rev Micro 2009;7:845

10
The spectrum of tuberculosis Barry CE. Nat Rev Micro 2009;7:845

11
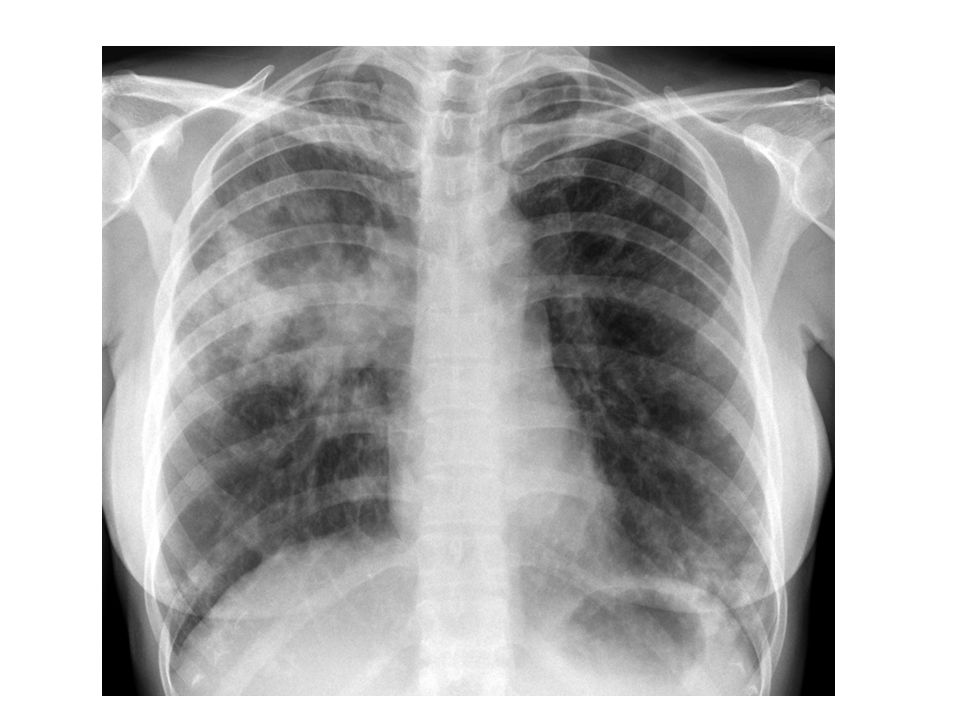
The typical, atypical CXR of TB/HIV

12
The spectrum of tuberculosis Barry CE. Nat Rev Micro 2009;7:845

13
Clinical states of TB to consider Active TB Sub-clinical TB Latent TB infection (BCG vaccinated) (Treated TB)
 (Treated TB)")
14
WHO three Is strategy Intensified case finding Infection control Isoniazid preventative therapy

15
What is the aim of screening? High TB burden countries Active TB disease Subclinical TB disease Latent TB infection Low TB burden countries Latent TB infection Active TB disease Subclinical TB disease

16
Clinical states of TB to consider Active TB Sub-clinical TB Latent TB infection (BCG vaccinated) (Treated TB)
 (Treated TB)")
17
Undiagnosed culture positive PTB in HIV infection Durban, South Africa ART roll-out programme, 825 adults (median blood CD4 100) Single sputum sample for MTB smear & culture 158 (19%) MTB culture+ (91% smear -) –48% no cough –22% no symptoms at all Bassett CID 2010;51:823
 Single sputum sample for MTB smear & culture 158 (19%) MTB culture+ (91% smear -) –48% no cough –22% no symptoms at all Bassett CID 2010;51:823")
18
Nucleic acid amplification in sub- clinical TB diagnosis South African, Adult ART roll out, CD4 171 2 sputums requested (468/515 at least 1) XpertTB MTB/RIF ( Boehme NEJM 2010 ) –Compare to culture & smear MTB cultured from 81/468 (17.3%) Xpert – sens 73%, spec 99% Smear – sens 28%, spec 100% Xpert achieved results using single sample & detected RIF resistance in 4 Lawn PLoS Med 2011;8:e1001067
 XpertTB MTB/RIF ( Boehme NEJM 2010 ) –Compare to culture & smear MTB cultured from 81/468 (17.3%) Xpert – sens 73%, spec 99% Smear – sens 28%, spec 100% Xpert achieved results using single sample & detected RIF resistance in 4 Lawn PLoS Med 2011;8:e")
19
Undiagnosed active TB in HIV How does this occur? –Reactivation? Rapid progression? New infection? Can symptom questionnaires pick out these subjects ie how many really have no symptoms? Are CXR/other tests helpful? What do we do once we have detected them? Can TB treatment duration be shortened in this population?

20
Clinical states of TB to consider Active TB Sub-clinical TB Latent TB infection (BCG vaccinated) (Treated TB)
 (Treated TB)")
21
Screening for active TB in TB endemic, high HIV areas Cambodia, Thailand, Vietnam Prospective screening questionnaire and sputum (3), stool, urine, blood +/- LN aspirate 267 (15%) of 1748 diagnosed with TB Cough (2 or 3 weeks in last 4): sens 22-33% Any cough + any fever or night sweats (3 weeks) in last 4 weeks: sens 93%, spec 36% –In such pts, 2 negative sputum smears, normal CXR, and CD4350 – ruled out active TB Cain NEJM 2010;362:707
, stool, urine, blood +/- LN aspirate 267 (15%) of 1748 diagnosed with TB Cough (2 or 3 weeks in last 4): sens 22-33% Any cough + any fever or night sweats (3 weeks) in last 4 weeks: sens 93%, spec 36% –In such pts, 2 negative sputum smears, normal CXR, and CD4350 – ruled out active TB Cain NEJM 2010;362:707")
22
Symptoms & CRP at diagnosis in active TB in the UK HIV+ (n=42)HIV- (n=101) No cough45%36% No fever17%46%* No sweats19%48%** No weight loss21%45%*** No fever, sweats & weight loss 7%33%**** Normal CRP7%18% No fever, sweats & weight loss plus normal CRP 2%13% * p=0.008; **p=0.001; ***p=0.02; ****p=0.003Breen. IJTLD 2008;12:44

23
Symptoms & CRP at diagnosis in active TB in the UK HIV+ (n=42)HIV- (n=101) No cough45%36% No fever17%46%* No sweats19%48%** No weight loss21%45%*** No fever, sweats & weight loss 7%33%**** Normal CRP7%18% No fever, sweats & weight loss plus normal CRP 2%13% * p=0.008; **p=0.001; ***p=0.02; ****p=0.003Breen. IJTLD 2008;12:44

25
Cavity Parenchymal band Tree in bud Nodules Bronchial thickening Consolidation Ground glass

26
Tree in bud

27
Clinical states of TB to consider Active TB Sub-clinical TB Latent TB infection (BCG vaccinated) (Treated TB)
 (Treated TB)")
28
Can we refine screening in low prevalence areas? USA & Canada study, NA-ACCORD –reporting not active screening 1995 – 2009; 41% previously on ARV Endpoint: TB diagnosed after starting ART Follow up median 4.7 years Increase in TB rates for at least 6 months of ART –at 3/12 = 215/100,000. Background rate = 5/100,000 Associated risk (ie who is best screened) –Blood CD4<200, high HIV load, non-Whites, history of IDU Sterling JID 2011;204;893
 –Blood CD4<200, high HIV load, non-Whites, history of IDU Sterling JID 2011;204;893.")
29
UK (BHIVA) approach to LTBI Balance risk of active TB developing vs Risk of drug induced hepatotoxicity* * Serious hepatotox estimated as 0.3%
 approach to LTBI Balance risk of active TB developing vs Risk of drug induced hepatotoxicity* * Serious hepatotox estimated as 0.3%")
30
UK (BHIVA) approach to LTBI Use data from available low incidence countries –UK CHIC* –Swiss HIV cohort study** Risk based on –Country of origin –Blood CD4 count –Use & duration of use of ART –Blood IGRA result *AIDS 2009;23:2507 **CID 2007;44:94
 approach to LTBI Use data from available low incidence countries –UK CHIC* –Swiss HIV cohort study** Risk based on –Country of origin –Blood CD4 count –Use & duration of use of ART –Blood IGRA result *AIDS 2009;23:2507 **CID 2007;44:94")
31
BHIVA recommendation: When to give LTBI treatment in UK HIV Sub- Saharan Africa Medium TB incidence country Low TB incidence country Blood IGRA +++ Blood CD4 count Any<500<350 Duration of ART use <24 months <6 months

32
TB assessment summary Clinical history (incl PMH) Examination CXR (TST/IGRA) Sputum (x1-3) –Smear & culture –Nucleic acid amplification
 Examination CXR (TST/IGRA) Sputum (x1-3) –Smear & culture –Nucleic acid amplification")
33
Isoniazid preventative therapy Botswana IPT 6/12 vs 36/12 (+/- ART) TB INH 6: 34/989 (3.4%) [1.26%/yr] TB INH 36: 20/1006 (2.0%) [0.72%/yr], p=0.047! Effect limited to TST+ subjects –?increased mortality in TST- on INH 36 Possible additional benefit of ART Samandari Lancet 2011;377:1588
![Isoniazid preventative therapy Botswana IPT 6/12 vs 36/12 (+/- ART) TB INH 6: 34/989 (3.4%) [1.26%/yr] TB INH 36: 20/1006 (2.0%) [0.72%/yr], p=0.047.](http://images.slideplayer.com/2/722572/slides/slide_33.jpg "Effect limited to TST+ subjects – increased mortality in TST- on INH 36 Possible additional benefit of ART Samandari Lancet 2011;377:1588.")
34
Other preventative therapies South Africa – HIV+ TST+ N= 1148, CD4 484 Randomised –INH 300mg 6/12 –INH 300mg continuous (up to 6 years) –Rifapentine 900mg + INH 900mg weekly 12/52 –Rifampin 600mg + INH 900mg twice weekly 12/52 TB incidence: 3.6% vs 2.7% vs 3.1 vs 2.9% No difference in survival Martinson NEJM 2011;365:11
 –Rifapentine 900mg + INH 900mg weekly 12/52 –Rifampin 600mg + INH 900mg twice weekly 12/52 TB incidence: 3.6% vs 2.7% vs 3.1 vs 2.9% No difference in survival Martinson NEJM 2011;365:11")
35
Summary HIV has altered our understanding of TB and human host interaction TB control = HIV control = TB control = …. Management strategies are location and person specific (implications for healthcare planning and resource use) There is a lot going on in TB/HIV!
 There is a lot going on in TB/HIV!.")
36
Problems with HAART + anti-TB Rx EARLY con-comitant use = drug-drug interactions additive adverse effects high pill burden reduced patient adherence immune reconstitution disease DELAY con-comitant use = high risk of major opportunistic infection & death Velasco JAIDS 2009;50:148. Westreich AIDS 2009; 23:707

37
Active TB: when to start HAART South African study Adults, Smear+ PTB, CD4<500 Integrated ( 4/52) n = 429 vs Sequential n = 213 TB & HAART Primary end point - death 56% in Int group IRIS - Int 12.4% vs Seq 3.8% (no deaths) Severe AE Int 30 vs Seq 32 per 100 py Abdool Karim. NEJM 2010;362:697-706

38
Timing of HAART 2 weeks vs 8-12 weeks will be answered by: SAPIT follow up; STRIDE; CAMELIA Karim S NEJM 2010

39
BHIVA recommendation: to start HAART Blood CD4 count (cells/μL) Recommendation <100As soon as practical 100-350 As soon as practical, but can wait till after 2 months TB treatment (if drug interactions, adherence or toxicity a problem) >350At physicians discretion BHIVA TB/HIV Guidelines 2010
 Recommendation <100As soon as practical As soon as practical, but can wait till after 2 months TB treatment (if drug interactions, adherence or toxicity a problem) >350At physicians discretion BHIVA TB/HIV Guidelines 2010")
40
TB/HIV treatment in UK practice Little difference in adverse events with different ARVS Good virological response with all ARVS No effect of TB on response to HAART No effect of HIV on TB outcome Breen JID 2006;193:1437

41
NICE HIV & TB CRG 2010 Blood CD4 <200 – TST & IGRA Either positive – ASSESS FOR ACTIVE TB & CONSIDER TREATMENT FOR LTBI Blood CD4 200-500 – IGRA OR TST/IGRA Either positive – ASSESS FOR ACTIVE TB & CONSIDER TREATMENT FOR LTBI Blood CD4 >500 – CONSIDER AS IMMUNCOMPETENT ADULT NO DISTINCTION BETWEEN IGRA TEST TYPES

Similar presentations