Download presentation
Presentation is loading. Please wait.

2
Primary glomerular diseases Talia Weinstein MD PhD Sourasky Medical Center

3
נ

28
FSGS FSGS has become the leading cause of primary nephrotic syndrome in adults The appearance of new forms of FSGS has led to the approach that FSGS is seen today as a clinico-pathologic syndrome, comprising diverse distinct diseases with different etiologies The approach to the diagnosis of FSGS is problematic because the morphologic features are non-specific and can occur in a variety of conditions or may be superimposed on other glomerular processes

29
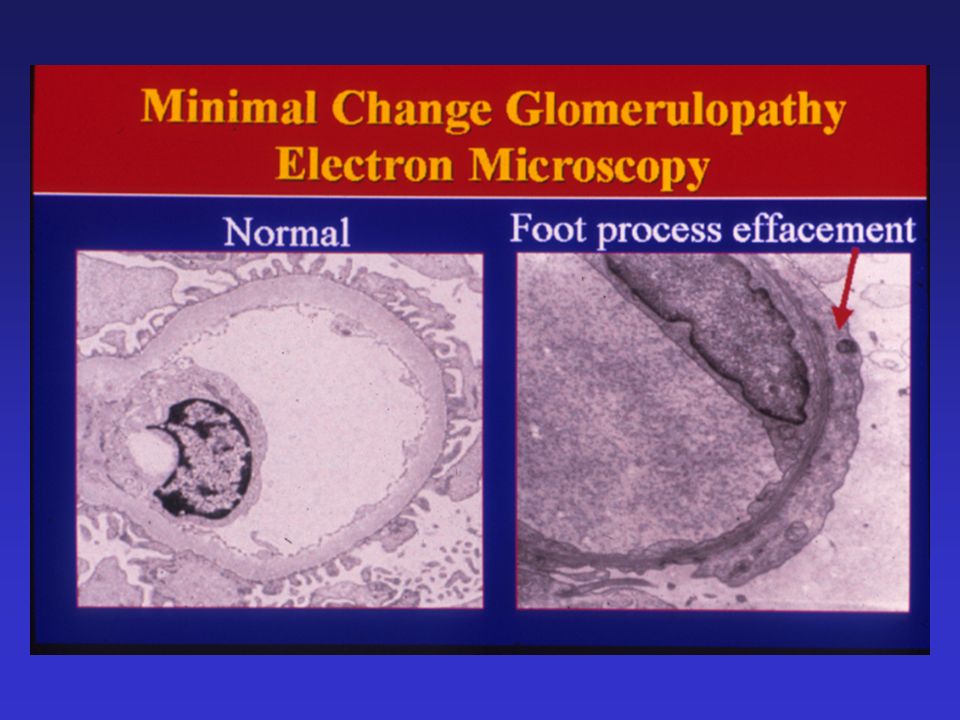
FSGS - Pathology The sine qua non of FSGS is the presence of increased amounts of extracellular matrix Typical pathologic features include segmental glomerular scars Immunofluorescence is negative or positive only for IgM and C3 A ominous sign is the presence of tubular atrophy or interstitial inflammatory cells

31
What is FSGS? Idiopathic FSGS is the primary manifestation of a specific renal disease FSGS is a defined lesion that occurs after stimulation by a variety of causes FSGS is a common final pathway of glomerular obliteration that occurs after myriad lesions of the kidney

32
The diagnosis of FSGS is further complicated by the existence of a primary (or idiopathic) form and many secondary forms Before a diagnosis of primary FSGS can be reached, secondary forms must be carefully excluded These include genetic mutations, viral infection, drug toxicity, as well as a large group of FSGS caused by intrarenal vasodilatation and increased glomerular capillary pressure secondary to reduced renal mass or hemodynamic stress
 form and many secondary forms Before a diagnosis of primary FSGS can be reached, secondary forms must be carefully excluded These include genetic mutations, viral infection, drug toxicity, as well as a large group of FSGS caused by intrarenal vasodilatation and increased glomerular capillary pressure secondary to reduced renal mass or hemodynamic stress")
34
Primary (idiopathic) FSGS HIV-associated nephropathy Heroin-associated nephropathy Familial FSGS: mutations in actinin, podocin, mitochondrial cytopathies Drug toxicity: pamidronate, interferon- lithium Secondary FSGS: a) due to reduced functional nephrons: unilateral agenesis, dysplasia, reflux nephropathy, sequela to cortical necrosis. b) due to hemodynamic stress: obesity, sickle cell anemia Diabetes mellitus, hypertension Nonspecific scarring: focal proliferative GN, hereditary nephritis, membranous nephropathy
 due to hemodynamic stress: obesity, sickle cell anemia Diabetes mellitus, hypertension Nonspecific scarring: focal proliferative GN, hereditary nephritis, membranous nephropathy.")
35
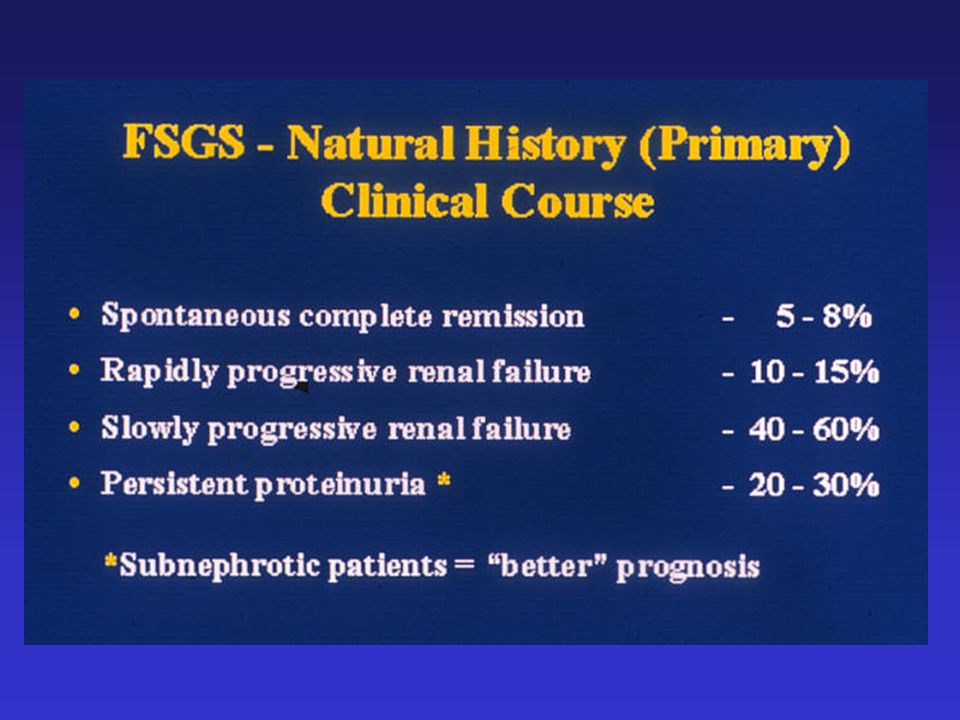
Clinical presentation Glomerular proteinuria is invariably present, but may be either nephrotic or sub- nephrotic Hypertension and hematuria may also be present Progression to to renal insufficiency and end-stage renal disease occurs; spontaneous remission occurs less commonly

37
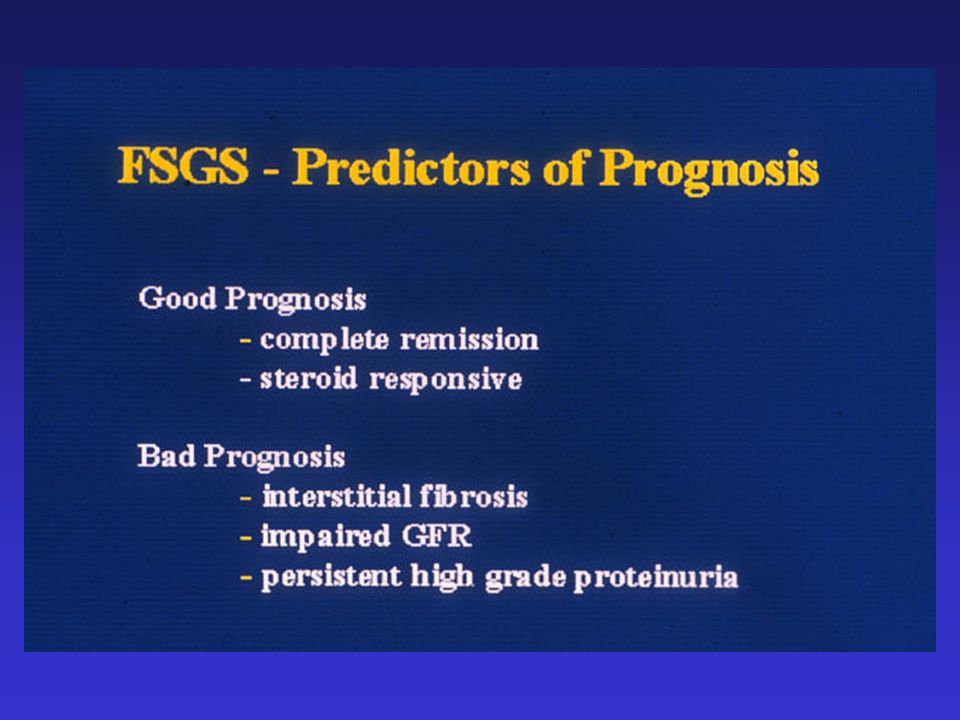
Accounts for 7% of glomerular lesions in children and up to 35% of lesions in adults presenting with the nephrotic syndrome The prevalence in blacks is 2 to 4 times that in whites Despite similar degrees of renal insufficiency at presentation, patients with secondary FSGS have a 5-year renal survival of 80% compared with 50% for patients with primary FSGS

40
The therapeutic approach to secondary FSGS depends upon the underlying condition Correction of the underlying process such as surgical repair of reflux, should be sought In patients with reduced renal mass (such as agenesis, hypertension), maneuvers to reduce glomerular capillary pressure (ACEI/ARB) are offered Steroids are uniformly ineffective in familial forms and secondary FSGS, and may even promote weight gain and sclerosis in patients with obesity and latent diabetes
, maneuvers to reduce glomerular capillary pressure (ACEI/ARB) are offered Steroids are uniformly ineffective in familial forms and secondary FSGS, and may even promote weight gain and sclerosis in patients with obesity and latent diabetes")
48
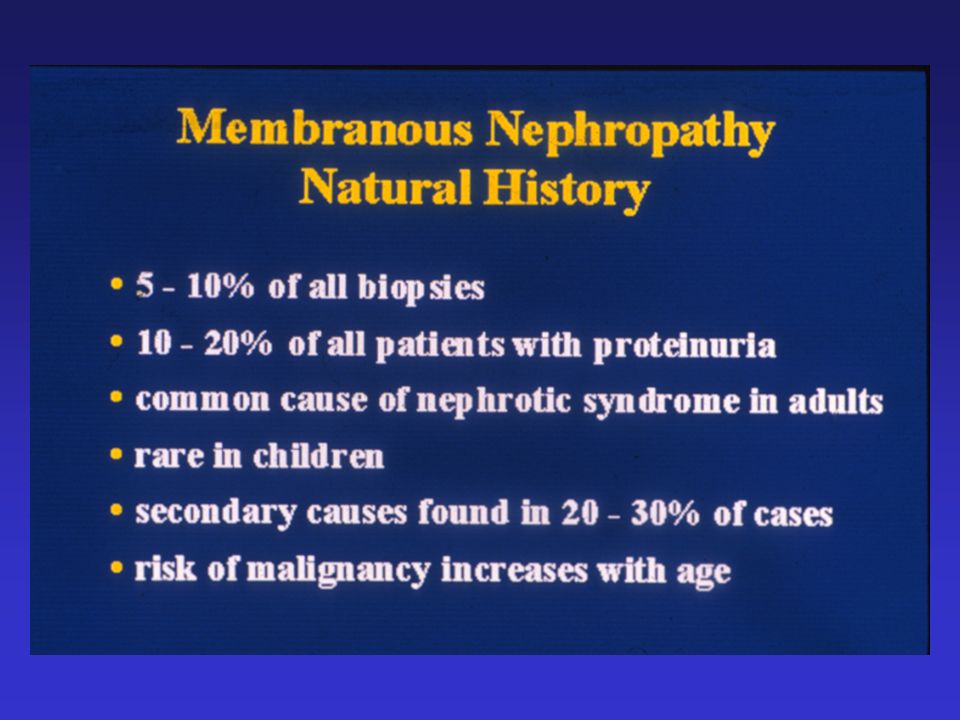
Therapy In view of the potential toxicity of the drugs used to treat idiopathic MN, the decision to initiate therapy is based in part on an understanding of the natural history of untreated patients with this disorder: - spontaneous remission of proteinuria occurs in 5- 10% - partial remission (< or = 2 gr/d) occurs in 25-40% - the incidence of end stage renal disease is about 14% at 5 years, 35% at 10 years, and 41% at 15 years
 occurs in 25-40% - the incidence of end stage renal disease is about 14% at 5 years, 35% at 10 years, and 41% at 15 years")
49
Risk factors for progressive disease: - men >50 years with the nephrotic syndrome - extensive duration of heavy proteinuria - patients with an elevated serum creatinine - on biopsy glomerular scarring and TI disease Therefore immunosuppressive agents should be considered only in those patients most at risk

50
Corticosteroids Cytotoxic agents cyclophosphamide chlorambucil Cyclosporine Mycofenolate Mofetil (MMF)
")
58
Nephritic syndrome Hematuria Red blood cell casts

61
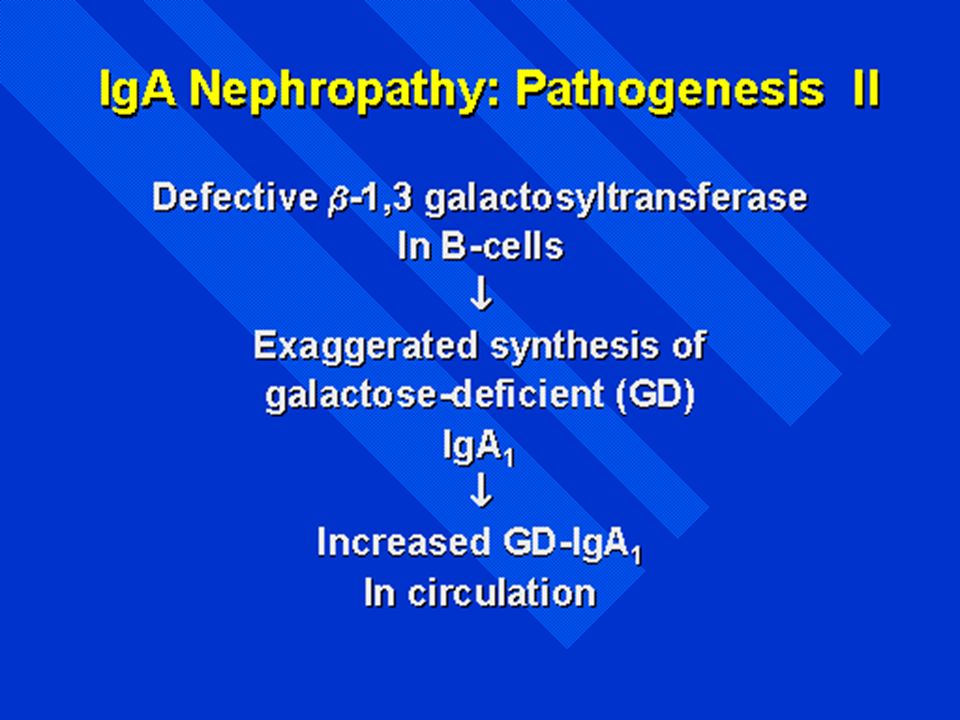
Micro/macrohematuria May follow URTI High IgA in serum IgA found in mesangium on IF

Similar presentations















































 FSGS Secondary FSGS 1. Familial/genetic.>")







 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")

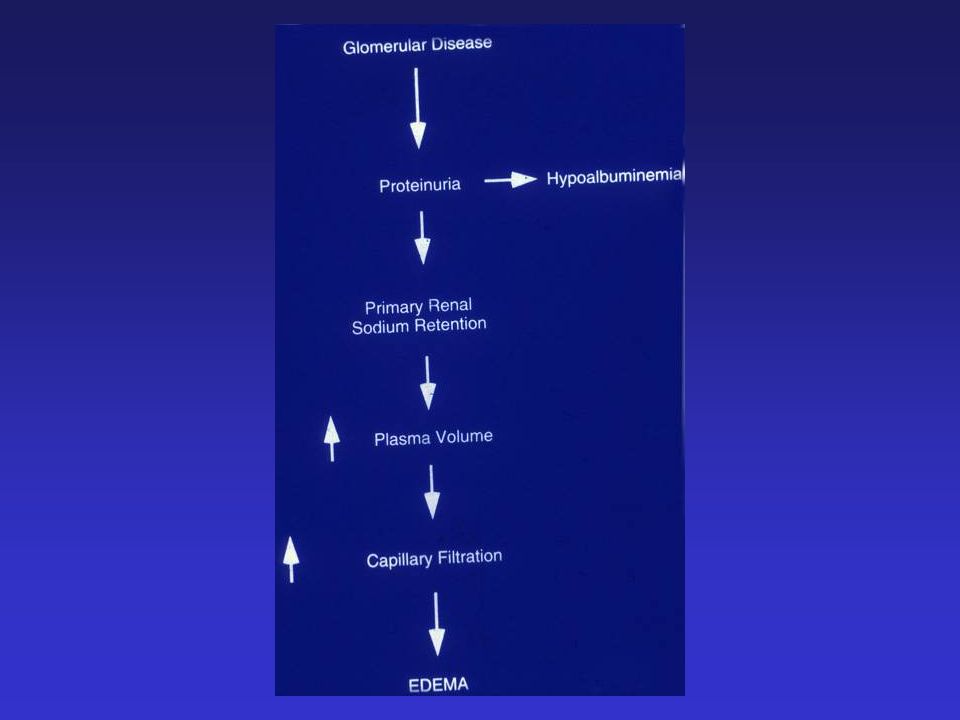
 Characteristics : Proteinuria ( urine protein loss > 2 gm/day ) Hypo-proteinemia ( serum albumin < 2.5 gm/dL ) Edema Hyperlipidemia.>")








