Download presentation
Presentation is loading. Please wait.

1
This lecture was conducted during the Nephrology Unit Grand Ground by a Sub-intern under Nephrology Division, Department of Medicine in King Saud University. Nephrology Division is NOT responsible for the content of the presentation for it is intended for learning and /or education purpose only.

2
Nephrotic syndrome Done by : Nora AlMahmoud

3
Objectives: 0 Definition 0 Pathophysiology 0 Causes 0 Clinical manifestations 0 Complication 0 Diagnosis 0 Treatment

4
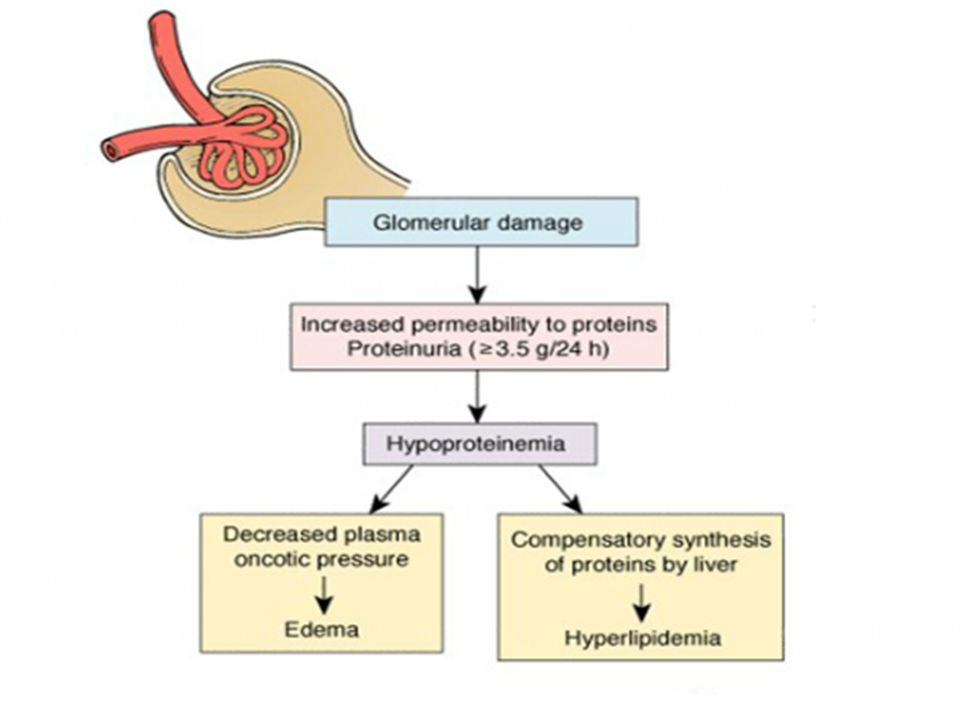
Definition Clinical complex that include the following : 1)Massive proteinuria (3.5g or more in adult). 2)Hypoalbuminemia (<3mg/dl) 3)Generalized edema 4)Hyperlipidemia and lipidurea
Hypoalbuminemia (<3mg/dl) 3)Generalized edema 4)Hyperlipidemia and lipidurea.")
5
0 Urinary loss of anticoagulants proteins, i.e.: protein C, protein S, and antithrombin Hypercoagulable state 0 Urinary loss of transport proteins Iron, Copper, and Zinc deficiency

6
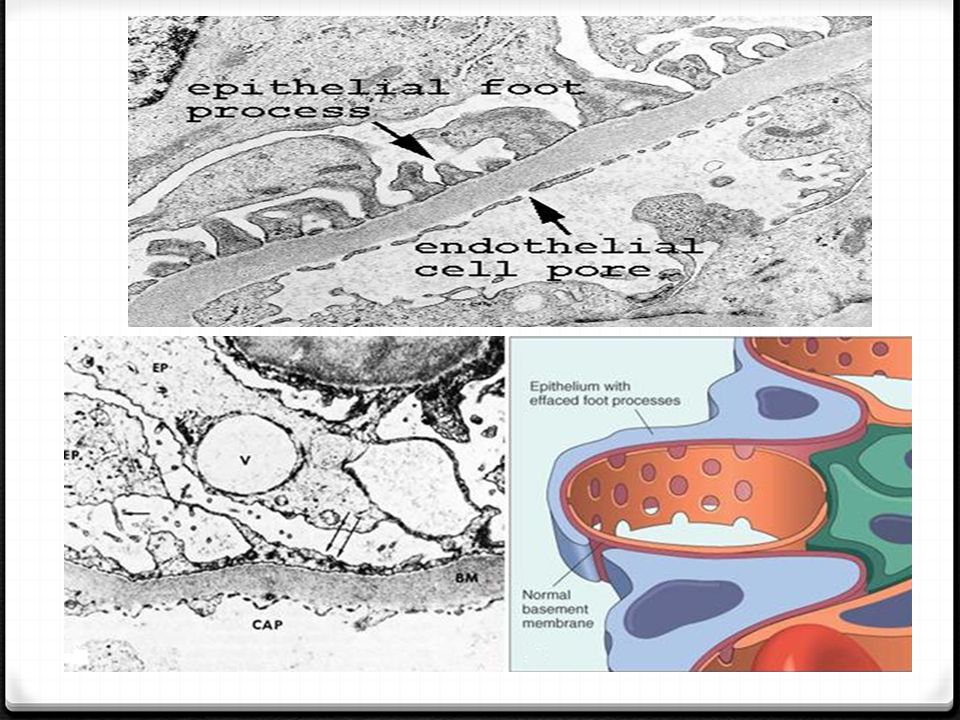
Pathophysiology Damage to Podocytes (glomerulus epithelial cells) allows proteins to pass through a 'leaky' glomerulus into the urine. Normally molecules of <20kDa will pass into the urine In Nephrotic syndrome molecules of >100kDa can pass into the urine

8
Causes 0 Causes of nephrotic syndrome vary according to age. 0 In children : always caused by lesion primary to the kidney. 0 In adult often due to renal manifestation of a systemic disease.

9
Primary causes 0 Membranous GN 0 Minimal change disease 0 Focal segmental glumerulosclerosis 0 Membranoproliferative GN

10
Membranous GN 0 Most common cause in Adult 0 The 1ry disease is idiopathic 0 The 2ry form is due to: -infection (Hepatitis C and B viruses, Malaria, syphilis ) - Drugs (gold, Captopril, penicillamine) - Neoplasm or Lupus 0 Deposition of Ag-Ab complexes
 - Drugs (gold, Captopril, penicillamine) - Neoplasm or Lupus 0 Deposition of Ag-Ab complexes")
12
Minimal change disease 0 Most common cause in Children 0 Associated with Hodgkin’s and non-Hodgkin’s lymphoma 0 No histological abnormality in light microscopy, Fusion of foot processes on Electron microscopy.

14
FSGN 0 Account for 25% of cases of nephrotic syndrome in adult 0 Associated with: HIV, Heroin, sickle cell and obesity. 0 It has fair to poor prognosis – resistant to steroid therapy – patient develop renal insufficiency within 5-10 years of diagnosis, the course is progressive.

15
Membranoproliferative GN 0 Can be idiopathic or 2ry to chronic immune disease (Hepatitis C, Alpha1 antitrypsin, HIV, Malignancy ) 0 GBM alteration, sub endothelial leukocytes infiltration, predominant masengial involvement.
 0 GBM alteration, sub endothelial leukocytes infiltration, predominant masengial involvement.")
16
Secondary causes 0 Systemic lupus erythematosus (SLE). 0 Amyloidosis. 0 Diabetes Mellitus. 0 Allergy. 0 Infections.(HBV, HCV, HIV, Malria, syphilis). 0 Drugs(Gold)
. 0 Drugs(Gold).")
17
Clinical Picture edema first presents periorbitally Ankle edema Severe proteinuria increase BP More severe features occur late or if untreated and may include pulmonary effusion, genital edema and anasarca (severe generalised edema).
.")
19
Complications 1. Venous thromboembolism 2. Extreme hypercholesterolaemia (>10mmol/L) 3. Infection 4. Renal Failure 5. Malnutrition

20
How to approach pt. with Neprotic syndrome? 0 Patient history - Identify medication or toxin exposure; risk factors for HIV or viral hepatitis; and symptoms suggesting other causes of edema Obtain history of diabetes, systemic lupus erythematosus, or other systemic illness 0 Urine dipstick : Confirm proteinuria 0 Random urine protein/creatinine ratio : Quantify degree of proteinuria (ratio greater than 3 to 3.5) 0 Serum creatinine : Rule out acute renal failure, assess glomerular filtration rate 0 Serum albumin : Assess degree of hypoalbuminemia 0 Lipid panel 0 Assess degree of hyperlipidemia
 0 Serum creatinine : Rule out acute renal failure, assess glomerular filtration rate 0 Serum albumin : Assess degree of hypoalbuminemia 0 Lipid panel 0 Assess degree of hyperlipidemia.")
21
0 Additional studies suggested by patient factors: -HIV screening test - Identify HIV -Hepatitis serology panel -Identify hepatitis B or C -Serum or urine protein electrophoresis -Suggests amyloidosis or multiple myeloma -Rapid plasma reagin -Identify syphilis - Antinuclear antibodies or complement (C3 and C4) level -Identify systemic lupus erythematosus; complement levels may also be reduced in membranoproliferative disease
 level -Identify systemic lupus erythematosus; complement levels may also be reduced in membranoproliferative disease")
22
Diagnosis 0 Urin analysis shows >3.5 g/24h : - Most often used: single spot urine for albumin and creatinine. 0 Most accurate test to determine etiology is : Renal Biopsy

23
Treatment 3 Aims: 1) Treat fluid retention : Restrict salt and water intake loop diuretic +/- thiazide diuretic ACE inhibitor +/- Angiotensin 2 receptor antagonist 2 ) Avoid complications: prophylactic heparin prompt treatment of infection treat hyperlipidaemia (statins) target BP 125/75
 Treat fluid retention : Restrict salt and water intake loop diuretic +/- thiazide diuretic ACE inhibitor +/- Angiotensin 2 receptor antagonist 2 ) Avoid complications: prophylactic heparin prompt treatment of infection treat hyperlipidaemia (statins) target BP 125/75")
24
3) Treat the underlying cause 0 steroids in all idiopathic 1ry renal disease 0 If steroids ineffective : -add Cyclophosphamide or Mycophenolate 0 ACE inhibitor used in all patients but does not reverse the disease
 Treat the underlying cause 0 steroids in all idiopathic 1ry renal disease 0 If steroids ineffective : -add Cyclophosphamide or Mycophenolate 0 ACE inhibitor used in all patients but does not reverse the disease")
25
Nephrotic Vs. Nephritic syndromes Nephrotic s.Nephritic s. PathogenesisAbnormal glomerular permeability due to number of conditions Inflammation of the Glomeruli due to any of the causes of Glumerulonephritis Causes1ry and 2ry causesPoststrept. Glomerulonephritis is the most common cause Lab findingProteinuria >3.5g/24h Hypoalbuminemia Hyperlipidemia, Fatty cast in the urine Hematuria ARF-Azotemia, Oliguria Proteinuria if present mild Clinical finding Generalized Edema Hypercoagulable state Increase risk of infection HTN Edema

Similar presentations




>")
 Definition NS is an accumulation of symptoms and signs and is characterized by proteinuria, hypoproteinemia, edema, and hyperlipidemia.>")
 saying that her legs have been swollen for a month. On examination you find that she has.>")








 Membranous glomerulonephritis Focal segmental glomerulosclerosis.>")

 RENAL DISEASE: OVERVIEW AND ACUTE RENAL FAILURE Pathophysiology of Disease: Chapter 16 (388-394) Jack.>")




