Download presentation
Presentation is loading. Please wait.

1
Should there be air there? Elizabeth M. Regan November 22, 2013 Dr. Cameron; Dr. P.Smith, Dr. Ebersole

2
CC: abdominal pain, N/V, T101.3 HPI: Patient is a 42 y/o female who originally presented to the ED on 10/26 with 1 month history of cough and markedly elevated WBC of 200. Patient was diagnosed with ALL and admitted for workup and initiation of chemotherapy. Her hospital stay became complicated by an UE DVT, large left- sided pleural effusion and retroperitoneal hematoma s/p BM biopsy. On 11/11 patient developed mid-epigastric abdominal pain, N/V and became febrile to 101.3 F. PMH: HTN, UE DVT, left-sided pleural effusion, hematoma PSH: nill Allergies: NKA Social: never smoker, denies alcohol and drug use CASE: OS (MR:6605248) 2
 2.")
3
Physical Exam: – Vitals: T99.3, BP 136/70, HR 112, RR 20, O2 97% – CONSTITUTIONAL: NAD – LUNGS: CTAB – CARDIOVASCULAR: NSR normal S1 and S2, no S3 or S4, no murmur – ABDOMEN: Normal bowel sounds, soft, mildly distended, TTP over epigastric and RUQ – EXTREMITIES: no LE edema, Left upper extremity - no longer edematous surrounding PICC, not TTP – NEURO: A&Ox3, CNII-XII grossly intact – SKIN: no rashes Labs: – Neutropenic – Normal lactate CASE

4
Acute Abdominal Pain, Fever – Ulcer – Pancreatitis – Infectious (Viral, Abscess) – Biliary Obstruction (cholecystitis, cholangitis, malignancy) – Tumor Lysis Imaging Modalities to consider – Ultrasound vs CT vs MRI? – Contrast? – Decision: CT abdomen and pelvis with IV contrast Working Clinical Diagnoses

5
Appropriateness Criteria

6
Normal CT Abdomen (Level of Stomach) Axial CT (with PO contrast)
 Axial CT (with PO contrast)")
7
OS CT Abdomen (Stomach)
")
8
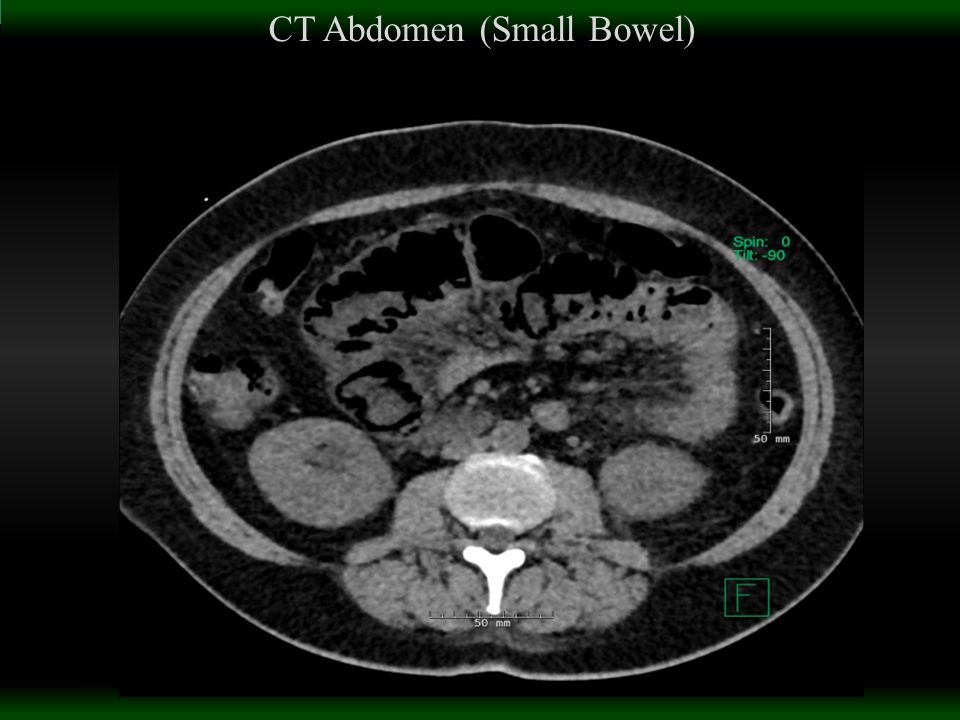
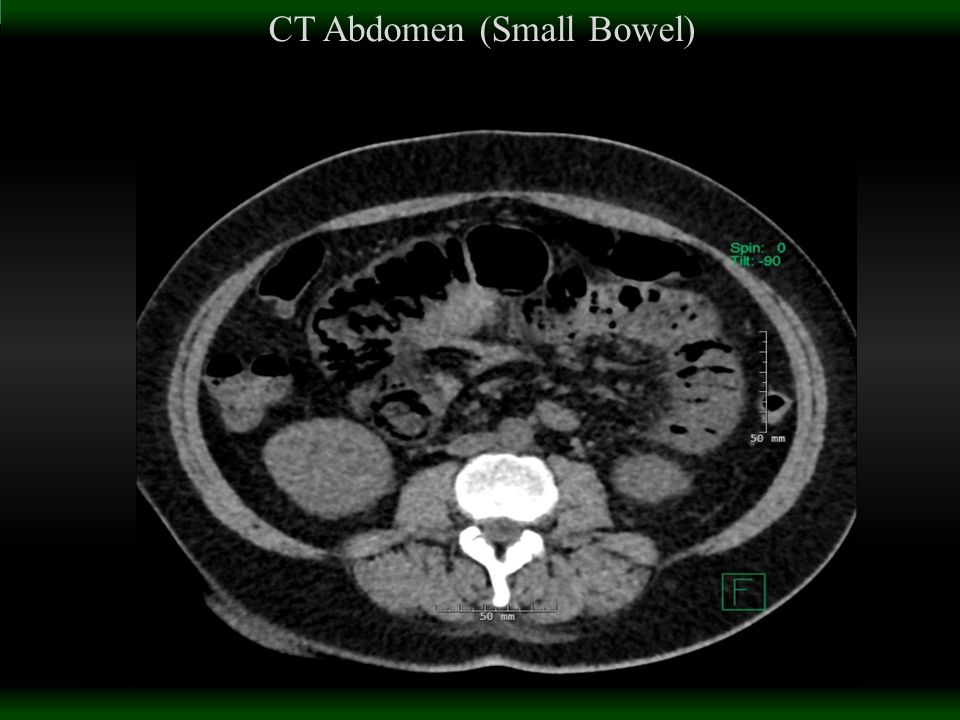
CT Abdomen (Small Bowel)
")
11
Pneumatosis intestinalis seen in posterior gastric wall, small bowel, as well as air within draining gastric vein What’s next? – Investigate for pneumoperitoneum

12
OS KUB- 1 view

13
OS CXR-No pneumoperitoneum

14
Abnormal CXR: Free Air under Diaphragm

15
Pneumatosis Intestinalis – Gas within the wall of the bowel; Can occur anywhere between esophagus and rectum – Symptom of multiple disease states, both GI and non-GI related – Can be benign or an emergency Emergencies include pneumoperitoneum, bowel ischemia/infarction Most presentations are benign; most patients are actually asymptomatic – Most Common in adults ages 40-70 as well as in the neonate population (associated with Necrotizing enterocolitis). Equal prevalence in males and females Working Diagnosis/ Pathology

16
– Most commonly associated disease states: COPD Immunocompromised states Inflammatory or infectious causes of GI tract Recent surgical or endoscopic procedures Diabetes Ischemia – Clinical Presentation usually includes: N/V, abdominal pain, mucus or blood in stools, weight loss

17
Plain Films: – Intramural gas can be linear, curvilinear, or circular in appearance – Linear pneumatosis tends to be more ominous, but can be benign – If pneumoperiotoneum is also present, look for: free air under the diaphragm, Rigler’s sign, falciform ligament sign CT: – More sensitive – Circumferential collections of air adjacent to lumen of bowel Characteristic Findings

18
Patient was non-peritonitic, complaining only of mild pain No pneumoperitoneum Surgery consulted, no evidence for bowel infarction/ischemia Serial abdominal exams, prontonix, and fluid resuscitation Patient improved within 36 hours. No surgical intervention needed. Outcome/Treatment

Similar presentations



 …the story of Mrs Harvey-Henry Dr Julian Dickmann General Surgery.>")















