Download presentation
Presentation is loading. Please wait.

1
肝癌年報

2
Hepatocellular Carcinoma: Overview
Burden of HCC Surveillance and diagnosis Staging and treatment algorithms Early HCC Intermediate HCC Advanced HCC A look to the future HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: This presentation will discuss the burden of hepatocellular carcinoma (HCC), methods of HCC surveillance and diagnosis, and staging and treatment algorithms pertaining to early HCC, intermediate HCC, and advanced HCC. Finally, we will look to the future of HCC management. 2
, methods of HCC surveillance and diagnosis, and staging and treatment algorithms pertaining to early HCC, intermediate HCC, and advanced HCC. Finally, we will look to the future of HCC management. 2.")
3
衛生署2008 & 2010死亡統計 惡性腫瘤自1982年起即高居台灣民眾死因首位,
2008年死亡人數首次破14萬人,標準化死亡率為每10萬人口484.3人 十大死因:惡性腫瘤為3萬8913人,佔所有死亡人數的27.3% 、標準化死亡率 為每10萬人口133.7人 2008年十大癌症順位分別是肺癌占20%、肝癌占19.7%、結腸直腸癌占11%、 女性乳癌占4%、胃癌占5.9% 衛生署資料顯示,2010年死亡人數占率依序為:惡性腫瘤占28.4%、心臟疾病 占10.8%、腦血管疾病占7.0%、

4
肝細胞癌 的發生率 在民國69年的統計中,男性與女性的每十萬人死亡率分別 是26.10 及8.14 肝細胞癌 的發生率男性是每十萬人有二十五人,在女性 是每十萬人有十人。 年發生率在慢性 B型肝炎的人是0.826 %,在大於35歲的 慢性 B型肝炎病人是2.77%,在肝硬化的人是5.6 %, 在B 型肝炎病毒表面抗原(HBsAg) 陰性的肝硬化病人是 %,在HBsAg 陽性的肝硬化病人是 %。 台灣的肝癌死亡率在東部山區有顯著的較高,而在西部山 區則較低。最高的死亡率見於澎湖群島
 陰性的肝硬化病人是 %,在HBsAg 陽性的肝硬化病人是 %。 台灣的肝癌死亡率在東部山區有顯著的較高,而在西部山 區則較低。最高的死亡率見於澎湖群島.")
5
肝癌最盛行的年齡 肝癌最盛行的年齡見於31至60歲之間,在民國50年代,最 高的發生率是在41 至50歲之間,但在爾後的研究則為50至 60歲。 肝硬化併發肝癌的平均年齡是56.7歲,在非肝硬化者則為 52歲。HBsAg 陽性的肝癌病人,其平均年齡是55歲,而在 HBsAg 陰性且C 型肝炎病毒抗體陽性的肝癌病人,其平均年 齡是65.7 歲。

6
Malignant Transformation Multistep
Normal liver Liver cirrhosis Hepatitis C Hepatitis B Ethanol NASH Epigenetic alterations Genetic alterations HCC[2] Dysplastic nodules[1] Potential Targets Oxidative stress and inflammation Viral oncogenes Carcinogens Growth factors Telomere shortening Cancer stem cells Loss of cell cycle checkpoints Antiapoptosis Angiogenesis HCC, hepatocellular carcinoma; NASH, nonalcoholic steatohepatitis. Jorge A. Marrero, MD, MS: This slide illustrates the multistep transformation that results in the development of HCC. The process starts with a normal liver that undergoes chronic liver injury, for example, infection with hepatitis C or hepatitis B, leading to fibrosis development and, eventually, cirrhosis. The next phase is dysplasia, which in turn evolves through genetic or epigenetic alterations into HCC. This sequence has been studied in detail and more is being discovered about the exact pathways that underlie malignant transformation as time goes by. 1. Tornillo L, et al. Lab Invest. 2002;82: Verslype C, et al. AASLD Abstract 24. 6 6

7
Surveillance for Hepatoma
Cost-effective The expected HCC > 1.5% /year in patients with hepatitis C and 0.2% / year in patients with hepatitis B

8
Patients for Whom HCC Surveillance Is Recommended
Asian males HBV carriers older than 40 yrs of age Asian female HBV carriers older than 50 yrs of age HBV carrier with HCC family history African/N American blacks with HBV Cirrhotic HBV carriers Hepatitis C with cirrhosis Stage 4 primary biliary cirrhosis Genetic hemochromatosis and cirrhosis Alpha-1 antitrypsin deficiency and cirrhosis Other cirrhosis 80% of patients with HCC have underlying cirrhosis HBV, hepatitis B virus; HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: This slide shows patients for whom HCC surveillance is recommended. According to guidelines from the American Association for the Study of Liver Disease (AASLD), surveillance is recommended in Asian males or females with hepatitis B who are older than 40 or 50 years of age, respectively; carriers of hepatitis B with a family history of HCC; Africans or North African black persons with hepatitis B; cirrhotic patients with hepatitis B; and patients with hepatitis C cirrhosis or cirrhosis from other causes. Josep M. Llovet, MD: The great majority (approximately 80%) of patients with HCC has underlying cirrhosis whereas only a small proportion of patients with noncirrhotic livers develop HCC. Mostly, these are patients with chronic hepatitis B, but most patients who should be included in surveillance programs are cirrhotic patients. Bruix J, et al. AASLD HCC guidelines. July 2010. Simonetti RS, et al. Dig Dis Sci. 1991;36:
, surveillance is recommended in Asian males or females with hepatitis B who are older than 40 or 50 years of age, respectively; carriers of hepatitis B with a family history of HCC; Africans or North African black persons with hepatitis B; cirrhotic patients with hepatitis B; and patients with hepatitis C cirrhosis or cirrhosis from other causes. Josep M. Llovet, MD: The great majority (approximately 80%) of patients with HCC has underlying cirrhosis whereas only a small proportion of patients with noncirrhotic livers develop HCC. Mostly, these are patients with chronic hepatitis B, but most patients who should be included in surveillance programs are cirrhotic patients. Bruix J, et al. AASLD HCC guidelines. July Simonetti RS, et al. Dig Dis Sci. 1991;36:")
9
AASLD Surveillance Guidelines
Surveillance recommended in at-risk groups Specific hepatitis B carriers Non–hepatitis B cirrhosis HCC surveillance should be performed with ultrasound Patients should be screened at 6-mo intervals Increased surveillance interval in patients at higher risk not needed AASLD, American Association for the Study of Liver Diseases; HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: The AASLD guidelines recommend that HCC surveillance be performed with ultrasound and that patients should be screened at 6-month intervals. Bruix J, et al. AASLD HCC guidelines. July 2010.

10
Diagnosis of HCC should be based on imaging techniques and/or biopsy

11
Diagnostic Algorithm for Suspected HCC

12
Diagnosis of Hepatocellular Carcinoma
The application of dynamic imaging criteria applied only to patients with cirrhosis of any etiology chronic hepatitis B who may not have fully developed cirrhosis or have regressed cirrhosis. High-grade dysplastic nodules or HCC ?? staining for 1.glypican 3 2.heat shock protein 70 3 glutamine synthetase Positivity for two of these three stains confirms HCC Bosetti C, Levi F, Boffetta P, Hepatology 2008;48:137–145.

13
Staging Systems and Treatment Strategies in HCC
Jorge A. Marrero, MD, MS: The next section of this presentation discusses staging systems and treatment strategy for HCC.

14
Variables used in staging
Tumor factors - Tumor size - Portal vein thrombosis - AFP Liver function - Child - Pugh criteria - MELD - score Over all heath of the patient Performance status Efficacy of treatment

15
Staging systems for Hepatoma
Clinical staging vs Pathological staging Outcome prediction - TNM - Okuda - CLIP (The Cancer of the Liver Italian Program) - JIS ( Japanese Integrated score ) Treatment option - BCLC ( Bacelona Clinic Liver Cancer)
 - JIS ( Japanese Integrated score ) Treatment option. - BCLC ( Bacelona Clinic Liver Cancer)")
16
AJCC staging system 2002

17
The prognostic value of the AJCC staging system (the 2002 edition)
Has been validated in liver transplantation The most accurate system to stratify post-transplantation outcomes The AJCC staging is the only one that is validated in patients treated with either hepatic resection or transplantation Vauthey JN, Ribero D, Abdalla EK, J Am Coll Surg. 2007;204(5):1016.
:1016.")
18
The prognostic value of the AJCC staging system (the 2002 edition)
Five-year survival rates, based upon the TNM staging system are as follows Stage I – 55 percent Stage II – 37 percent Stage III – 16 percent Vauthey JN, Lauwers GY, Esnaola NF, J Clin Oncol. 2002;20(6):1527.
:1527.")
19
Tumor, Node, Metastasis (TNM) staging
Staging of liver cancer includes only HCC; intrahepatic bile duct cancer is staged separately. The T3 category is split any of which are >5 cm (T3a; stage IIIA) versus tumors of any size that involve a major portal vein or hepatic vein (T3b, stage IIIB). stage IIIC disease. A T4 primary (direct invasion of an adjacent organ other than the gallbladder or with perforation of the visceral peritoneum) constitutes Inferior phrenic lymph nodes are no longer classified as a distant metastatic site (stage IVB) but as regional lymph node involvement (N+, stage IVA).
 versus tumors of any size that involve a major portal vein or hepatic vein (T3b, stage IIIB). stage IIIC disease. A T4 primary (direct invasion of an adjacent organ other than the gallbladder or with perforation of the visceral peritoneum) constitutes. Inferior phrenic lymph nodes are no longer classified as a distant metastatic site (stage IVB) but as regional lymph node involvement (N+, stage IVA).")
20
Tumor, Node, Metastasis (TNM) staging
Stage IV include all metastasis Stage IVa - includes node-positive disease (N1). Stage IVb- distant metastasis (M1).
. Stage IVb- distant metastasis (M1).")
21
TNM-7- 2010 Classification for Hepatocellular Carcinoma
Stage T1 Single, no vascular Invasion Stage T2 Single with vascular invasion, or Multiple tumors non> 5cm Stage T3a Multiple tumor with any > 5cm Stage T3b Any T with major portal vein or hepatic vein Stage T3c T4 adjacent organ, No GB ,No perforation of visceral peritoneum Stage IVa Any T N1 Stage IVb Any N 1

22
Okuda staging System

23
The Cancer of the Liver Italian Program score (CLIP)
")
24
CLIP in Clinical Practice
THE CANCER OF THE LIVER ITALIAN PROGRAM (CLIP) INVESTIGATORS HEPATOLOGY 1998; 28: HEPATOLOGY 2000;31:
 INVESTIGATORS HEPATOLOGY 1998; 28: HEPATOLOGY 2000;31:")
25
Five prognostic factors : Karnofsky performance status
The French Groupe d'Etude et de Traitement du Carcinome Hepatocellulaire (GETCH) Multivariate analysis of prognostic factors in 761 patients from 34 countries Five prognostic factors : Karnofsky performance status Serum bilirubin >50 micromol/L (>2.9 mg/dL) Serum alkaline phosphatase at least ≧ twice the upper limit of normal Serum alpha-fetoprotein >35 ng/mL Ultrasonographic portal obstruction
 Multivariate analysis of prognostic factors in 761 patients from 34 countries. Five prognostic factors : Karnofsky performance status. Serum bilirubin >50 micromol/L (>2.9 mg/dL) Serum alkaline phosphatase at least ≧ twice the upper limit of normal. Serum alpha-fetoprotein >35 ng/mL. Ultrasonographic portal obstruction.")
26
JIS (Japanese Integrated Score)
")
27
BCLC Staging System HCC Stage 0 Stage A-C Stage D PS 0, Child-Pugh A
Okuda 1-2, PS 0-2, Child-Pugh A-B Okuda 3, PS > 2, Child-Pugh C Very early stage (0) Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm Carcinoma in situ Single or 3 nodules Portal invasion, < 3 cm, PS 0 N1, M1, PS 1-2 Multinodular, PS 0 BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PST, performance status. Josep M. Llovet, MD: The Barcelona system differentiates 5 stages of HCC disease. Stage 0 cases are chronic patients with small lesions, < 2 cm in size, with single tumors, and no evidence of vascular invasion or extrahepatic spread. These should be asymptomatic, Child-Pugh A class patients. Early-stage patients have a single tumor or 3 nodules < 3 cm according to the Milan criteria, and an ECOG performance score of 0, whereas intermediate-, advanced-, and terminal-stage patients have multinodular or disseminated disease. Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 27
 Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm. Carcinoma in situ. Single or 3 nodules. Portal invasion, < 3 cm, PS 0. N1, M1, PS 1-2. Multinodular, PS 0. BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PST, performance status. Josep M. Llovet, MD: The Barcelona system differentiates 5 stages of HCC disease. Stage 0 cases are chronic patients with small lesions, < 2 cm in size, with single tumors, and no evidence of vascular invasion or extrahepatic spread. These should be asymptomatic, Child-Pugh A class patients. Early-stage patients have a single tumor or 3 nodules < 3 cm according to the Milan criteria, and an ECOG performance score of 0, whereas intermediate-, advanced-, and terminal-stage patients have multinodular or disseminated disease. Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 27.")
28
Variables Used in HCC Staging Systems
Tumor Staging Liver Function Health Status Europe-US GETCH/ French PVT; AFP < 35 or > 35 ug/L Bilirubin, alkaline phosphatase Karnofsky CLIP Number of nodules, tumor > or < 50% area of liver, and PVT; AFP< 400 or ≥ 400 ng/mL CTP No BCLC Tumor size, number of nodules, and PVT PST TNM Number of nodules, tumor size, presence of PVT, and presence of metastasis Asia JIS Okuda/ Tokyo Tumor > or < 50% of cross-sectional area of liver Ascites, albumin, and bilirubin CUPI TNM; AFP< 500 or ≥ 500 ng/mL Bilirubin, ascites, alkaline phosphatase Symptoms BCLC, Barcelona Clinic Liver Cancer; CLIP, Cancer of Liver Italian Program; CTP, Child-Turcotte-Pugh; CUPI, Chinese University Prognostic Index; GETCH, Groupe d'Etude de Traitement du Carcinome Hepatocellular; HCC, hepatocellular carcinoma; JIS, Japanese Integrated Staging System; TNM, tumor node metastasis. Josep M. Llovet, MD: Several staging systems have been proposed for HCC. All systems include an assessment of tumor stage and most also include liver function. An exception is the tumor necrosis metastasis (TNM) system, which measures fibrosis rather than liver function. Only a few staging systems capture variables related to health status such as Eastern Cooperative Oncology Group (ECOG) performance or Karnofsky score. In fact, only the Barcelona Clinic Liver Cancer (BCLC) system includes ECOG performance score; the French Groupe d'Etude de Traitement du Carcinome Hepatocellular system includes Karnofsky score, and the Chinese University Prognostic Index (CUPI) system includes the presence of symptoms. In the West, the staging systems that are most widely applied are the BCLC system and, less so, the TNM system. The Japanese Integrated Staging System score and the CUPI system are widely used in Asia. For more information, go online to: Marrero JA, et al. Hepatology. 2005;41: 28
 system, which measures fibrosis rather than liver function. Only a few staging systems capture variables related to health status such as Eastern Cooperative Oncology Group (ECOG) performance or Karnofsky score. In fact, only the Barcelona Clinic Liver Cancer (BCLC) system includes ECOG performance score; the French Groupe d Etude de Traitement du Carcinome Hepatocellular system includes Karnofsky score, and the Chinese University Prognostic Index (CUPI) system includes the presence of symptoms. In the West, the staging systems that are most widely applied are the BCLC system and, less so, the TNM system. The Japanese Integrated Staging System score and the CUPI system are widely used in Asia. For more information, go online to: Marrero JA, et al. Hepatology. 2005;41:")
29
Comparison of HCC Staging Systems
BCLC system uses key independent predictors of survival Performance score, portal vein thrombosis, tumor diameter Compared with other staging systems in cohort study BCLC had best stratification of survival across all stages BCLC was only system to have independent predictive value on survival BCLC is the only staging system that stratifies patients into treatment groups BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma. Josep M. Llovet, MD: Dr. Marrero led a comparative study of HCC staging systems in a cohort of American patients that identified the BCLC system as the best predictor of survival. In addition, the BCLC system is the only system that stratifies patients into treatment groups as well as provides prognostic stratification. For more information, go online to: Marrero JA, et al. Hepatology. 2005;41:

30
BCLC Staging and Treatment Strategy
HCC PS 0, Child-Pugh A Okuda 1-2, PS 0-2, Child-Pugh A-B Okuda 3, PS > 2, Child-Pugh C Very early stage (0) Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm Carcinoma in situ Single or 3 nodules Portal invasion, < 3 cm, PS 0 N1, M1, PS 1-2 Multinodular, PS 0 Single 3 nodules ≤ 3 cm Portal pressure/bilirubin Increased Associated diseases BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PEI, percutaneous ethanol injection; PS, performance score; RCT, randomized controlled trial; RFA, radiofrequency ablation; TACE, transarterial chemoembolization. Josep M. Llovet, MD: With appropriate use of resection, transplantation, and local ablation, 5-year survival rates > 50% can be expected, rising to 70% with resection and liver transplantation. However, these treatments are currently considered in approximately 30% of patients in the West and even fewer patients worldwide. For example, in Asia, only 5% to 10% of patients receive potentially curative therapies. Jorge A. Marrero, MD, MS: How does one choose between radiofrequency ablation and resection, given that there are data from a randomized trial showing no difference in overall survival between the 2 strategies? If the tumor is < 2 cm in diameter, radiofrequency ablation can achieve a complete response rate of up to 98%, which is comparable with resection. In tumors of this size, the decision of whether to apply radiofrequency ablation rather than resection may depend on local availability of a hepatobiliary team with experience in resecting tumors or, conversely, access to an interventional radiologist able to perform local ablation with high accuracy. For tumors > 2 cm in diameter, in my experience, local ablation does not achieve a complete response rate of 100%, and as the tumor size increases, the response rate decreases, such that for a tumor of 4-5 cm in diameter, radiofrequency ablation achieves complete response in approximately 50% to 60% of cases. This does not compete well with resection. Therefore, resection remains a first-line treatment option for tumors > 2 cm in diameter. For very small tumors of < 2 cm, there is a question about which approach is optimal, and local expertise should factor in the decision. Normal No Yes Resection Liver transplantation RFA/PEI TACE Sorafenib Symptomatic (20%); survival < 3 mos Curative treatments (30%); 5-yr survival: 40%-70% RCTs (50%); 3-yr survival: 10%-40% Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 30
 Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm. Carcinoma in situ. Single or 3 nodules. Portal invasion, < 3 cm, PS 0. N1, M1, PS 1-2. Multinodular, PS 0. Single. 3 nodules ≤ 3 cm. Portal pressure/bilirubin. Increased. Associated. diseases. BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PEI, percutaneous ethanol injection; PS, performance score; RCT, randomized controlled trial; RFA, radiofrequency ablation; TACE, transarterial chemoembolization. Josep M. Llovet, MD: With appropriate use of resection, transplantation, and local ablation, 5-year survival rates > 50% can be expected, rising to 70% with resection and liver transplantation. However, these treatments are currently considered in approximately 30% of patients in the West and even fewer patients worldwide. For example, in Asia, only 5% to 10% of patients receive potentially curative therapies. Jorge A. Marrero, MD, MS: How does one choose between radiofrequency ablation and resection, given that there are data from a randomized trial showing no difference in overall survival between the 2 strategies If the tumor is < 2 cm in diameter, radiofrequency ablation can achieve a complete response rate of up to 98%, which is comparable with resection. In tumors of this size, the decision of whether to apply radiofrequency ablation rather than resection may depend on local availability of a hepatobiliary team with experience in resecting tumors or, conversely, access to an interventional radiologist able to perform local ablation with high accuracy. For tumors > 2 cm in diameter, in my experience, local ablation does not achieve a complete response rate of 100%, and as the tumor size increases, the response rate decreases, such that for a tumor of 4-5 cm in diameter, radiofrequency ablation achieves complete response in approximately 50% to 60% of cases. This does not compete well with resection. Therefore, resection remains a first-line treatment option for tumors > 2 cm in diameter. For very small tumors of < 2 cm, there is a question about which approach is optimal, and local expertise should factor in the decision. Normal. No. Yes. Resection. Liver transplantation. RFA/PEI. TACE. Sorafenib. Symptomatic (20%); survival < 3 mos. Curative treatments (30%); 5-yr survival: 40%-70% RCTs (50%); 3-yr survival: 10%-40% Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 30.")
31
Treatment for Very Early Stage Hepatoma

32
Treatment for Very Early Stage Hepatoma
Hepatic resection or ablation of HCC lesion < 2cm have the same 5- year survival rates Decision based on tumor location, hepatic function, functional status, other co-morbidities, local practice Resection limited to patients with compensated cirrhosis - bilirubiin < 2mg/dl, No portal hypertension, platelet >105 In studies of Child A resection for tumor <2 cm - The 5 year survival rates 49-93%, 5 year recurrence 80% 1. Takayama T, Hepatology 1998;28:1241– Ikai I Cancer 2004;101:796– Zhou XD Cancer 2001;91:1479– Nathan H Ann Surg 2009; 249:799–805.

33
Ablation as the first line approach for very early HCC
A cohort study of radiofrequency ablation of 218 patients Complete ablation of lesions < 2 cm - 97% in 31 ms, with a local recurrence rate of less than 1%. 5 year recurrence rate 80% NO RCT to compare surgery or RFA Markov Model simulating 10,000 patients -overall survival was nearly identical in RFA and HR Livraghi T, Meloni F, Di Stasi M, et al. HEPATOLOGY 2008;47:82-89. Cho YK, Kim JK, Kim WT, et al. Hepatology 2010;51:1284–1290.

34
Treatment for Early Stage Hepatomas

35
Resection Option Portal pressure measurement to predict the outcome has been validated in Japan. First option for patients who have the optimal profile, as defined by the BCLC staging system. Advanced liver disease, the mortality is higher – liver transplantation or ablation.

36
Resection versus Ablation
A RCT comparing Child-Pugh class A cirrhosis who have single HCCs 5 cm or less in diameter - No statistically significant differences Nonrandomized investigations – RFA can achieve similar survival rates as surgical resection in small, solitary tumors at the very early stage of the BCLC classification The response rates to RFA 70-95% in tumor < 3cm, In tumors ≧ 3 cm response rates 50-70% in > 3 cm. overall 5 year survival %

37
Candidates for RFA/PEI
Includes individuals who are not candidates for surgery Radiofrequency ablation generally preferred over percutaneous ethanol injection Necrotic effect more predictable across tumor sizes Meta-analyses suggest survival benefit with radiofrequency ablation vs percutaneous ethanol injection PEI, percutaneous ethanol injection; RFA, radiofrequency ablation. Josep M. Llovet, MD: A third option is percutaneous local ablation. This procedure is suitable for patients who are not candidates for surgery or liver transplantation. Radiofrequency ablation is considered the first-line treatment option for these patients based on data from 4 randomized, controlled trials that found this approach to be significantly more effective than percutaneous ethanol injection regarding local control of disease. In addition, meta-analyses suggest there may be an overall survival benefit in favor of radiofrequency ablation. Bruix J, et al. AASLD HCC guidelines. July 2010. 37

38
Combining RF ablation with TACE for (3.1–5.0 cm) HCCs
An RCT - evaluating the therapeutic efficacy of Combining RF ablation with TACE Local tumor progression rate were significantly lower in the TACE and RF ablation–treated group than in the RF ablation–only group (6% vs 39%, P =0.012) A phase III randomized double-blinded placebo controlled study with thermally sensitive liposomal doxorubicin in combination with RF ablation HCC is ongoing. Morimoto M , Numata K , Kondou M Cancer 2010 ; 116 ( 23 ): 5452 –
 A phase III randomized double-blinded placebo controlled study with thermally sensitive liposomal doxorubicin in combination with RF ablation HCC is ongoing. Morimoto M , Numata K , Kondou M Cancer 2010 ; 116 ( 23 ): 5452 –")
39
Adjuvant Therapy in the Resection Setting
Recurrence following resection (in one year –metastasis , late recurrence -De no Vo carcinogenesis) Approximately 50% at 3 yrs Approximately 70% at 5 yrs Positive results for several types of adjuvant therapy in this setting However, no standard-of-care adjuvant therapy for HCC patients undergoing resection RCT using Vit K2 , 548 patients- not effective Sorafenib after resection or ablation - ongoing Large, randomized, controlled trials of adjuvant therapy following resection HCC, hepatocellular carcinoma. Josep M. Llovet, MD: Recurrence is common following resection, occurring in approximately 50% of patients at 3 years, and 70% at 5 years. There is no recommendation at present regarding optimal adjuvant therapy, but numerous large, randomized, controlled trials are ongoing. Llovet JM, et al. Hepatology. 1999;30: Llovet JM, et al. J Natl Cancer Inst. 2008;100: 39
 Approximately 50% at 3 yrs. Approximately 70% at 5 yrs. Positive results for several types of adjuvant therapy in this setting. However, no standard-of-care adjuvant therapy for HCC patients undergoing resection. RCT using Vit K2 , 548 patients- not effective. Sorafenib after resection or ablation - ongoing. Large, randomized, controlled trials of adjuvant therapy following resection. HCC, hepatocellular carcinoma. Josep M. Llovet, MD: Recurrence is common following resection, occurring in approximately 50% of patients at 3 years, and 70% at 5 years. There is no recommendation at present regarding optimal adjuvant therapy, but numerous large, randomized, controlled trials are ongoing. Llovet JM, et al. Hepatology. 1999;30: Llovet JM, et al. J Natl Cancer Inst. 2008;100:")
40
Liver Transplantation for HCC: Milan Criteria (Stage 1 and 2)
Single tumor, not > 5 cm Up to 3 tumors, none > 3 cm + Absence of macroscopic vascular invasion, absence of extrahepatic spread HCC, hepatocellular carcinoma. Josep M. Llovet, MD: For patients with liver dysfunction, such as portal hypertension or abnormal bilirubin or those with Child-Pugh class B disease, the first-line treatment option is liver transplantation. When used appropriately, transplantation has been associated with 5-year survival rates of 70% and a 5-year recurrence rates of < 15%. However, there is a shortage of donors in almost every country worldwide. Were this not the case, liver transplantation could be considered in patients with single tumors not > 5 cm or with up to 3 tumors < 3 cm that are not resectable. 5-yr survival with transplantation: ~ 70% 5-yr recurrent rates: < 15% Mazzaferro V, et al. N Engl J Med. 1996;334: Llovet JM. J Gastroenterol Hepatol. 2002;17(suppl 3):S428-S433.
:S428-S433.")
41
UCSF (University of California, San Francisco criteria)
Solitary tumor < or = 6.5 cm, Three or fewer nodules with the largest lesion < or = cm Total tumor diameter < or = 8 cm, without gross vascular invasion

42
Solitary large ( > 5-cm) tumor
Not early-stage disease because they do not qualify for transplantation No upper limit of size for surgical resection appears in the BCLC flowchart These patients should not be excluded from surgical referral because their tumors are too large The results of transarterial therapies as standalone treatments are highly variable Down staging? Majno PE , Mentha G , Mazzaferro V ..Hepatology 2010 ; 51 ( 4 ): 1116 –
: 1116 –")
43
Treatment of Intermediate HCC
HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: The next section will focus on intermediate-stage HCC.

44
BCLC Staging and Treatment Strategy
HCC PS 0, Child-Pugh A Okuda 1-2, PS 0-2, Child-Pugh A-B Okuda 3, PS > 2, Child-Pugh C Very early stage (0) Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm Carcinoma in situ Single or 3 nodules Portal invasion, < 3 cm, PS 0 N1, M1, PS 1-2 Multinodular, PS 0 Single 3 nodules ≤ 3 cm Unresectable HCC Portal pressure/bilirubin Increased Associated diseases BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PEI, percutaneous ethanol injection; PS, performance score; RCT, randomized controlled trial; RFA, radiofrequency ablation; TACE, transarterial chemoembolization. Josep M. Llovet, MD: For patients with intermediate-stage B disease who have multinodular tumors without symptoms, no portal invasion, extrahepatic spread, or lymph node involvement, the recommended treatment is transarterial chemoembolization. Surgery is not indicated in patients who have satellite lesions or portal hypertension. Other treatment options include internal radiation with yttrium 90, which is currently in phase III study. Early data are encouraging, but there is insufficient evidence on which to base a recommendation at this point. Normal No Yes Resection Liver transplantation RFA/PEI TACE Sorafenib Symptomatic (20%); survival < 3 mos Curative treatments (30%); 5-yr survival: 40%-70% RCTs (50%); 3-yr survival: 10%-40% Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 44
 Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D) Single < 2 cm. Carcinoma in situ. Single or 3 nodules. Portal invasion, < 3 cm, PS 0. N1, M1, PS 1-2. Multinodular, PS 0. Single. 3 nodules ≤ 3 cm. Unresectable HCC. Portal pressure/bilirubin. Increased. Associated. diseases. BCLC, Barcelona Clinic Liver Cancer; HCC, hepatocellular carcinoma; PEI, percutaneous ethanol injection; PS, performance score; RCT, randomized controlled trial; RFA, radiofrequency ablation; TACE, transarterial chemoembolization. Josep M. Llovet, MD: For patients with intermediate-stage B disease who have multinodular tumors without symptoms, no portal invasion, extrahepatic spread, or lymph node involvement, the recommended treatment is transarterial chemoembolization. Surgery is not indicated in patients who have satellite lesions or portal hypertension. Other treatment options include internal radiation with yttrium 90, which is currently in phase III study. Early data are encouraging, but there is insufficient evidence on which to base a recommendation at this point. Normal. No. Yes. Resection. Liver transplantation. RFA/PEI. TACE. Sorafenib. Symptomatic (20%); survival < 3 mos. Curative treatments (30%); 5-yr survival: 40%-70% RCTs (50%); 3-yr survival: 10%-40% Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10): , by permission of Oxford University Press. 44.")
45
Natural History of Nonsurgical HCC Study Design: Control Arm of 2 RCTs
102 untreated cirrhotic patients with unresectable HCC Managed with symptomatic treatment Median survival of 17 months (range: 1-60 months) 1-yr survival was 54% 2-yr survival was 40% 3-yr survival was 28% BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; PS, performance score; RCT, randomized controlled trial. Josep M. Llovet, MD: Median survival in patients with intermediate-stage disease is approximately 17 months if left untreated but may be extended with chemoembolization. Llovet JM, et al. Hepatology. 1999;29:62-67.
 1-yr survival was 54% 2-yr survival was 40% 3-yr survival was 28% BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; PS, performance score; RCT, randomized controlled trial. Josep M. Llovet, MD: Median survival in patients with intermediate-stage disease is approximately 17 months if left untreated but may be extended with chemoembolization. Llovet JM, et al. Hepatology. 1999;29:")
47
Arterial Embolization for HCC Meta-analysis of 6 RCTs (2-Yr Survival)
Random Effects Model, OR (95% CI) Author, Journal Yr Patients, n Lin, Gastroenterology GETCH, NEJM Bruix, Hepatology Pelletier, J Hepatol Lo, Hepatology Llovet, Lancet Overall 503 0.01 0.1 0.5 1 2 10 100 GETCH, Groupe d'Etude de Traitement du Carcinome Hepatocellular; HCC, hepatocellular carcinoma; OR, odds ratio; RCT, randomized controlled trial. Josep M. Llovet, MD: Several randomized, controlled trials have been conducted in this patient population. The results of a meta-analysis published in 2003 found that chemoembolization was significantly more effective than best supportive care or suboptimal therapies, with a median survival of 20 months. Based on these data, both the European Association for the Study of the Liver and AASLD guidelines recommend chemoembolization as the first-line treatment option for this patient group. Z = -2.3 P = .017 Median survival: ~ 20 mos Favors Treatment Favors Control Llovet JM, et al. Hepatology. 2003;37:
 Author, Journal Yr Patients, n. Lin, Gastroenterology GETCH, NEJM Bruix, Hepatology Pelletier, J Hepatol Lo, Hepatology Llovet, Lancet Overall GETCH, Groupe d Etude de Traitement du Carcinome Hepatocellular; HCC, hepatocellular carcinoma; OR, odds ratio; RCT, randomized controlled trial. Josep M. Llovet, MD: Several randomized, controlled trials have been conducted in this patient population. The results of a meta-analysis published in 2003 found that chemoembolization was significantly more effective than best supportive care or suboptimal therapies, with a median survival of 20 months. Based on these data, both the European Association for the Study of the Liver and AASLD guidelines recommend chemoembolization as the first-line treatment option for this patient group. Z = P = Median survival: ~ 20 mos. Favors Treatment. Favors Control. Llovet JM, et al. Hepatology. 2003;37:")
48
Contraindications to TACE
Extrahepatic tumor spread Lack of portal blood flow Portal vein thrombosis, portosystemic anastomoses or hepatofugal flow Advanced liver disease (Child-Pugh Class B or C) Clinical symptoms of end-stage cancer TACE, transarterial chemoembolization. Josep M. Llovet, MD: Chemoembolization is not appropriate for all patients with intermediate-stage disease. For instance, extrahepatic spread, lack of portal blood flow, advanced disease, or clinical symptoms of end-stage cancer are contraindications for chemoembolization. Bruix J, et al. AASLD HCC guidelines. July 2010.
 Clinical symptoms of end-stage cancer. TACE, transarterial chemoembolization. Josep M. Llovet, MD: Chemoembolization is not appropriate for all patients with intermediate-stage disease. For instance, extrahepatic spread, lack of portal blood flow, advanced disease, or clinical symptoms of end-stage cancer are contraindications for chemoembolization. Bruix J, et al. AASLD HCC guidelines. July")
49
Survival After Yttrium-90 Resin Microsphere Radioembolization of HCC
325 patients September 2003 and December 2009 Child-Pugh class A (82.5%), underlying cirrhosis (78.5%) Common adverse events were: fatigue, nausea/vomiting, and abdominal pain. Grade 3 or higher increases in bilirubin were reported in 5.8% of patients. All-cause mortality was 0.6% and 6.8% at 30 and 90 days Bruno Sangro, Livio Carpanese, Roberto CianniHEPATOLOGY 2011;54: )
, underlying cirrhosis (78.5%) Common adverse events were: fatigue, nausea/vomiting, and abdominal pain. Grade 3 or higher increases in bilirubin were reported in 5.8% of patients. All-cause mortality was 0.6% and 6.8% at 30 and 90 days. Bruno Sangro, Livio Carpanese, Roberto CianniHEPATOLOGY 2011;54: )")
50
Survival After Yttrium-90 Resin Microsphere Radioembolization of HCC
The median overall survival was 12.8 months ( months) BCLC A, 24.4 months [ months] BCLC B, 16.9 months [ months] BCLC C, 10.0 months [ months Bruno Sangro, Livio Carpanese, Roberto Cianni HEPATOLOGY 2011;54: Overall median survival was 7.3 months in patients with BCLC class C without extrahepatic metastases and 10.4 months (95% CI: 7.2, 16.6) in those with Child-Pugh A with portal vein thrombosis Salem R , Lewandowski RJ , Mulcahy MF , et al . Gastroenterology 2010 ; 138 ( 1 ): 52 –
 BCLC A, 24.4 months [ months] BCLC B, 16.9 months [ months] BCLC C, 10.0 months [ months. Bruno Sangro, Livio Carpanese, Roberto Cianni HEPATOLOGY 2011;54: Overall median survival was 7.3 months in patients with BCLC class C without extrahepatic metastases and months (95% CI: 7.2, 16.6) in those with Child-Pugh A with portal vein thrombosis. Salem R , Lewandowski RJ , Mulcahy MF , et al . Gastroenterology 2010 ; 138 ( 1 ): 52 – 64 .")
51
Treatment of Advanced HCC
HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: We will now move on to discussion of treatment for advanced HCC.

52
Understanding Survival Outcomes in HCC Patients
Stage 0 PS 0, Child-Pugh A Stage A-C Okuda 1-2, PS 0-2, Child-Pugh A-B Stage D Okuda 3, PS > 2, Child-Pugh C Very early stage (0) Single < 2 cm Carcinoma in situ Early stage (A) Single or 3 nodules < 3 cm, PS 0 Intermediate stage (B) Multinodular, PS 0 Advanced stage (C) Portal invasion, N1, M1, PS 1-2 Terminal stage (D) 2010 Natural History Median OS > 36 mos Median OS 16 mos Median OS 6 mos (4-8 mos) HCC, hepatocellular carcinoma; OS, overall survival; PS, performance score; TACE, transarterial chemoembolization. Jorge A. Marrero, MD, MS: The current paradigm in HCC is that approximately 30% to 40% of patients are either stage 0 or A, whereas the majority has more advanced disease. If we do a good job of identifying patients at risk by promoting appropriate surveillance, then perhaps this paradigm will change in the future so that most patients will present with early-stage disease, perhaps leading to better outcomes. Josep M. Llovet, MD: I agree. This is what is happening now in Japan, where surveillance programs target the at-risk population effectively. Now, some 60% of Japanese patients are diagnosed at early stages of disease and 30% at a very early stage. Wider implementation of surveillance programs in the West could also achieve this goal. With Therapy Curative therapies OS > 60 mos TACE: OS 20 mos Sorafenib: 10.7 mos 2011 40% 20% 40% Stage at Diagnosis 2012 60% 20% 20% Courtesy of Josep M. Llovet, MD. 52
 Single < 2 cm. Carcinoma in situ. Early stage (A) Single or 3 nodules < 3 cm, PS 0. Intermediate stage (B) Multinodular, PS 0. Advanced stage (C) Portal invasion, N1, M1, PS 1-2. Terminal stage (D) Natural History. Median OS > 36 mos. Median OS. 16 mos. Median OS. 6 mos (4-8 mos) HCC, hepatocellular carcinoma; OS, overall survival; PS, performance score; TACE, transarterial chemoembolization. Jorge A. Marrero, MD, MS: The current paradigm in HCC is that approximately 30% to 40% of patients are either stage 0 or A, whereas the majority has more advanced disease. If we do a good job of identifying patients at risk by promoting appropriate surveillance, then perhaps this paradigm will change in the future so that most patients will present with early-stage disease, perhaps leading to better outcomes. Josep M. Llovet, MD: I agree. This is what is happening now in Japan, where surveillance programs target the at-risk population effectively. Now, some 60% of Japanese patients are diagnosed at early stages of disease and 30% at a very early stage. Wider implementation of surveillance programs in the West could also achieve this goal. With Therapy. Curative therapies OS > 60 mos. TACE: OS 20 mos. Sorafenib: 10.7 mos % 20% 40% Stage at Diagnosis % 20% 20% Courtesy of Josep M. Llovet, MD. 52.")
53
Phase III SHARP Trial: Sorafenib vs Placebo in Advanced HCC
Stratification by macroscopic vascular invasion and/or extrahepatic spread, ECOG PS, geographical region Sorafenib 400 mg BID PO (n = 299) Patients with advanced, measurable HCC, ECOG PS 0-2 (N = 602) Placebo (n = 303) ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; PS performance score; OS, overall survival. Josep M. Llovet, MD: The recommendation of sorafenib as the first-line treatment option for patients with advanced HCC is based on the results of SHARP, a large, double-blind, placebo-controlled trial comparing sorafenib vs placebo. The study was completed and published in 2008. For more information, go online to: Primary endpoints: OS, time to symptomatic progression Secondary endpoints: progression (radiologic, clinical), adverse events Llovet JM, et al. N Engl J Med. 2008;359:
 Patients with advanced, measurable HCC, ECOG PS 0-2. (N = 602) Placebo. (n = 303) ECOG, Eastern Cooperative Oncology Group; HCC, hepatocellular carcinoma; PS performance score; OS, overall survival. Josep M. Llovet, MD: The recommendation of sorafenib as the first-line treatment option for patients with advanced HCC is based on the results of SHARP, a large, double-blind, placebo-controlled trial comparing sorafenib vs placebo. The study was completed and published in For more information, go online to: Primary endpoints: OS, time to symptomatic progression. Secondary endpoints: progression (radiologic, clinical), adverse events. Llovet JM, et al. N Engl J Med. 2008;359:")
54
Phase III SHARP Trial: OS (ITT)
1.00 Sorafenib (n = 299) Median: 10.7 mos (95% CI: ) 0.75 Placebo (n = 303) Median: 7.9 mos (95% CI: ) Survival Probability 0.50 0.25 HR (S/P): 0.69 (95% CI: ; P = ) CI, confidence interval. Josep M. Llovet, MD: In the SHARP study, sorafenib significantly improved survival vs placebo, from a median of 7.9 months to 10.7 months in the sorafenib-treated group. For more information, go online to: 8 16 24 32 40 48 56 64 72 80 Wks Pts at Risk, n Sorafenib Placebo 299 303 274 276 241 224 205 179 161 126 108 78 67 47 38 25 12 7 2 Llovet JM, et al. N Engl J Med. 2008;359: Copyright © 2008 Massachusetts Medical Society. All rights reserved.
 Median: 10.7 mos (95% CI: ) Placebo (n = 303) Median: 7.9 mos (95% CI: ) Survival Probability HR (S/P): 0.69 (95% CI: ; P = ) CI, confidence interval. Josep M. Llovet, MD: In the SHARP study, sorafenib significantly improved survival vs placebo, from a median of 7.9 months to 10.7 months in the sorafenib-treated group. For more information, go online to: Wks. Pts at Risk, n. Sorafenib. Placebo Llovet JM, et al. N Engl J Med. 2008;359: Copyright © 2008 Massachusetts Medical Society. All rights reserved.")
55
Conclusions From Phase III SHARP Trial
Sorafenib is first systemic therapy to prolong survival in HCC patients Survival: HR: 0.69; 31% decrease in risk of death Time to radiologic progression: 5.5 mos with sorafenib vs mos with placebo (P < .001) In Asian patients , an identical RCT shows a median survival time of 4.2 months ( placeb) vs 6.5 months Sorafenib is the new reference standard for systemic therapy of HCC patients HCC, hepatocellular carcinoma; HR, hazard ratio. Josep M. Llovet, MD: The findings of the SHARP trial represent a breakthrough in the management of HCC. Sorafenib is the first systemic therapy that has been shown to prolong survival in patients with HCC and has been adopted by the AASLD and the European Association for the Study of the Liver guidelines as the new reference standard for systemic treatment of HCC. For more information, go online to: Llovet JM, et al. N Engl J Med. 2008;359: Cheng AL Lancet Oncology 2009; 10: 25-34
 In Asian patients , an identical RCT shows a median survival time of 4.2 months ( placeb) vs 6.5 months. Sorafenib is the new reference standard for systemic therapy of HCC patients. HCC, hepatocellular carcinoma; HR, hazard ratio. Josep M. Llovet, MD: The findings of the SHARP trial represent a breakthrough in the management of HCC. Sorafenib is the first systemic therapy that has been shown to prolong survival in patients with HCC and has been adopted by the AASLD and the European Association for the Study of the Liver guidelines as the new reference standard for systemic treatment of HCC. For more information, go online to: Llovet JM, et al. N Engl J Med. 2008;359: Cheng AL Lancet Oncology 2009; 10:")
57
HCC Management Liver disease and cancer
HCC is the intersection of 2 diseases Liver disease and cancer Skilled pathologists needed for diagnosis Specialists required to deliver treatment options Surgeons for resection or transplantation Radiologists ( Hepatologist )for ablation and chemoembolization Hepatologists and oncologists follow treatment strategy and labs Midlevel providers bring support, particularly for oral therapy HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: Management of HCC requires a multidisciplinary approach. Treatment options involve surgery, medical oncology, diagnostic and interventional radiology, as well as hepatology. Josep M. Llovet, MD: Hepatocellular carcinoma is a complex and unique disease, involving cirrhosis and liver disease as well as cancer. Hepatic resection and liver transplantation requires specialist surgeons, and skilled pathologists are needed to confirm diagnosis. Use of local ablation therapies and chemoembolization depends on access to interventional radiologists, and finally, hepatologists and oncologists must be well versed in treatment strategy. The multidisciplinary team is central to the management of this disease.
for ablation and chemoembolization. Hepatologists and oncologists follow treatment strategy and labs. Midlevel providers bring support, particularly for oral therapy. HCC, hepatocellular carcinoma. Jorge A. Marrero, MD, MS: Management of HCC requires a multidisciplinary approach. Treatment options involve surgery, medical oncology, diagnostic and interventional radiology, as well as hepatology. Josep M. Llovet, MD: Hepatocellular carcinoma is a complex and unique disease, involving cirrhosis and liver disease as well as cancer. Hepatic resection and liver transplantation requires specialist surgeons, and skilled pathologists are needed to confirm diagnosis. Use of local ablation therapies and chemoembolization depends on access to interventional radiologists, and finally, hepatologists and oncologists must be well versed in treatment strategy. The multidisciplinary team is central to the management of this disease.")
58
性別分佈 M: F = 2 : 1

59
年齡分佈

60
臨床期別分佈- stage I,II, III 增加

61
首次治療方式分佈 ─臨床期別Ⅰ期- 開刀與局部治療增加
首次治療方式分佈 ─臨床期別Ⅰ期- 開刀與局部治療增加

62
AJCC臨床期別

63
期別相關分佈 2008 107 10 9.35 2009 144 2010 177 AJCC臨床及病理期別為不詳比例 年份 申報數 %
2010 177
64
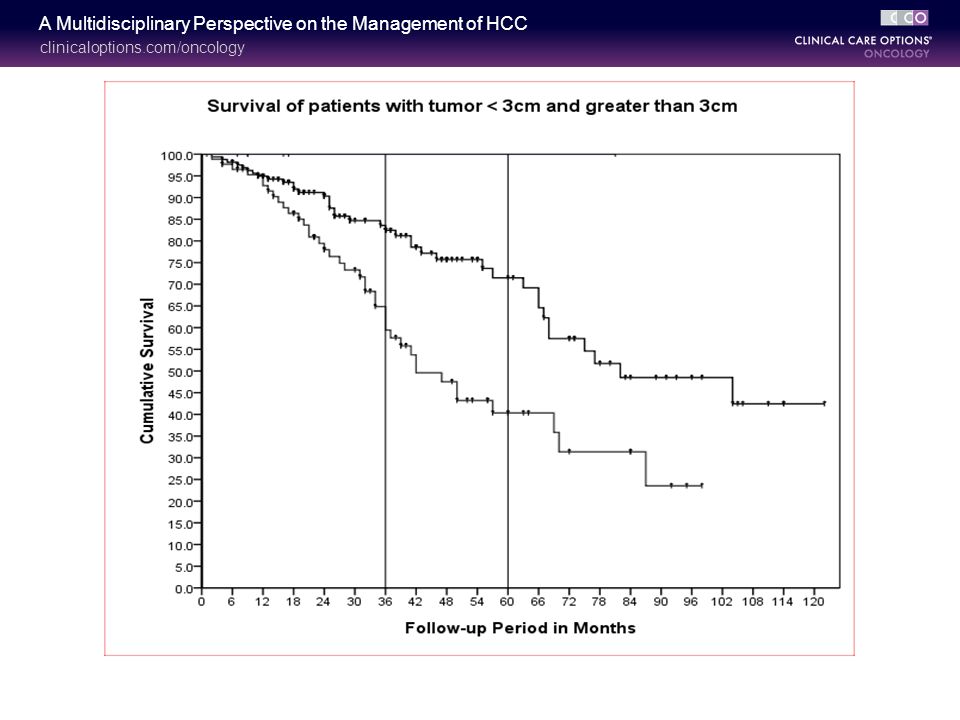
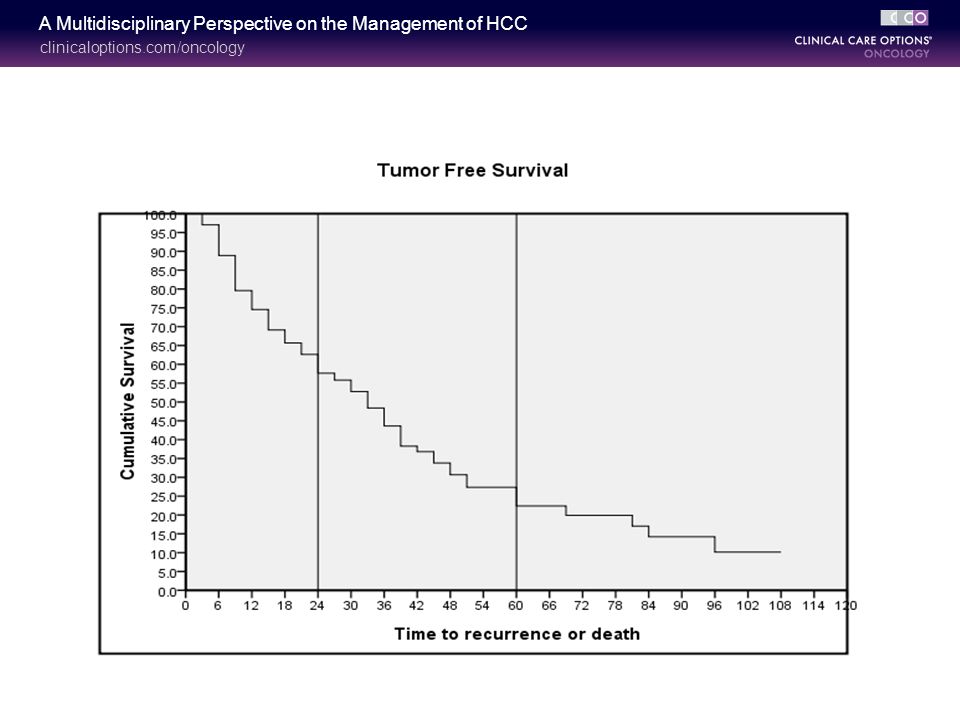
本院肝癌病患存活率分析結果 ─治療方式OP與RFA
●利用生命表法來繪製OP與RFA療法之存活曲線 (N =120) 註1:以 生命表法分析。
 註1:以 生命表法分析。")
Similar presentations





 for Liver Tumour Dr Dai Wing Chiu Queen Mary Hospital.>")











 New mass/nodule NoYes Alternative imaging technique Atypical featureTypical.>")

