Download presentation
Presentation is loading. Please wait.

1
Advances in Nuclear Medicine and its Impact on Diagnosis and Management of GI Cancers Medhat Osman, MD PhD Philip Alderson, MD

2
2007 Estimated US Cancer Cases * *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2007. Men 766,860 Women 678,060 26%Breast 15%Lung & bronchus 11%Colon & rectum 6%Uterine corpus 4%Non-Hodgkin 4%Non-Hodgkin lymphoma lymphoma 4%Melanoma of skin 4% Thyroid 4% Thyroid 3%Ovary 3%Ovary 3%Kidney 3%Kidney 3%Leukemia 21%All Other Sites Prostate29% Lung & bronchus15% Colon & rectum10% Urinary bladder7% Non-Hodgkin 4% lymphoma lymphoma Melanoma of skin4% Kidney4% Leukemia 3% Oral cavity3% Pancreas2% All Other Sites19%

3
2007 Estimated US Cancer Deaths * ONS=Other nervous system. Source: American Cancer Society, 2007. Men 289,550 Women 270,100 26%Lung & bronchus 15%Breast 10%Colon & rectum 6%Pancreas 6%Pancreas 6%Ovary 6%Ovary 4%Leukemia 4%Leukemia 3%Non-Hodgkin lymphoma 3%Non-Hodgkin lymphoma 3%Uterine corpus 3%Uterine corpus 2%Brain/ONS 2%Brain/ONS 2% Liver & intrahepatic bile duct 2% Liver & intrahepatic bile duct 23% All other sites Lung & bronchus31% Prostate9% Colon & rectum 9% Pancreas6% Leukemia4% Liver & intrahepatic4% bile duct Esophagus4% Urinary bladder3% Non-Hodgkin 3% lymphoma Kidney3% All other sites 24%

4
Lifetime Probability of Developing Cancer, by Site, Women, 2001-2003 * SiteRisk All sites † 1 in 3 Breast 1 in 8 Lung & bronchus 1 in 16 Colon & rectum 1 in 19 Uterine corpus 1 in 40 Non-Hodgkin lymphoma 1 in 55 Ovary 1 in 69 Melanoma 1 in 73 Pancreas 1 in 79 Urinary bladder ‡ 1 in 87 Uterine cervix 1 in 138 Source: DevCan: Probability of Developing or Dying of Cancer Software, Version 6.1.1 Statistical Research and Applications Branch, NCI, 2006. http://srab.cancer.gov/devcan * For those free of cancer at beginning of age interval. Based on cancer cases diagnosed during 2001 to 2003.

5
Source: DevCan: Probability of Developing or Dying of Cancer Software, Version 6.1.1 Statistical Research and Applications Branch, NCI, 2006. http://srab.cancer.gov/devcan Lifetime Probability of Developing Cancer, by Site, Men, 2001-2003 * Site Risk All sites † 1 in 2 Prostate 1 in 6 Lung and bronchus1 in 12 Colon and rectum1 in 17 Urinary bladder ‡ 1 in 28 Non-Hodgkin lymphoma1 in 47 Melanoma1 in 49 Kidney1 in 61 Leukemia1 in 67 Oral Cavity1 in 72 Stomach1 in 89

6
Basic Questions Is it cancer? Is it cancer? Is it localized ? Is it localized ? How to treat? How to treat? Is treatment working? Is treatment working? Is more treatment needed? Is more treatment needed?

7
Limitations of Anatomic Imaging Tumor diagnosis Tumor diagnosis Disease staging Disease staging Therapeutic response & disease recurrence Therapeutic response & disease recurrence Radiation exposure Radiation exposure –Annual background: 3 mSv –Chest PA : 0.02 mSv –Screeing Mammogram: 0.4 mSv –CT »Chest: 8-18 mSv »Abdomen: 3.5- 25 mSv »Pelvis: 3.3-10 mSv Mettler FA, et al. Radiology 2008:248 (1):254-263
:")
8
Benefits of PET Imaging Improved diagnostic specificity Improved diagnostic specificity Improved tumor staging Improved tumor staging Improved monitoring of response to therapy Improved monitoring of response to therapy Improved monitoring of disease recurrence Improved monitoring of disease recurrence

9
Limitations of PET Imaging False-positive False-positive False-negative False-negative Limited spatial resolution Limited spatial resolution Inability to pinpoint tumor location Inability to pinpoint tumor location Two hours per study! Two hours per study!

10
Positron Emission Tomography

11
Advantages of PET-CT Scanner Advantages of PET-CT Scanner Whole-body staging in one exam Whole-body staging in one exam Nearly simultaneous acquisition of PET and CT images Nearly simultaneous acquisition of PET and CT images Improved anatomic lesion localization Improved anatomic lesion localization Shorter PET image acquisition Shorter PET image acquisition Lower radiation exposure Lower radiation exposure –Whole body PET/CT at SLU: < 20 mSv –Chest, abdomen and pelvic CT: 14.8-53 mSv

12
COLORECTAL CARCINOMA Initial Diagnosis Sensitivity: 85% Sensitivity: 85% Specificity: 67% Specificity: 67% Facey K, et al. NHS. R&D Programme: July 2004

13
Colorectal Liver Metastases Colorectal Liver Metastases Wiering B, et al. Cancer 2005:104:2658-2670 SensitivitySpecificity PET88%96% ceCT83%84%

14
Colorectal Liver Metastases; on a per-lesion basis Bipat S, et al. Radiology. 2005:273:123-131 Sensitivity PET76% ceCT64% MRI (1.5-T) 64%
 64%.")
15
Extrahepatic Lesions Extrahepatic Lesions Wiering B, et al. Cancer. 2005:104:2658-2670 SensitivitySpecificity PET92%95% ceCT61%91%

16
PET Changes Management and Improves Prognostic Stratification in Patients with Recurrent Colorectal Cancer: Results of a Multicenter Prospective Study PET Changes Management and Improves Prognostic Stratification in Patients with Recurrent Colorectal Cancer: Results of a Multicenter Prospective Study 65.6% of patients with residual structural lesion suggestive of recurrence 65.6% of patients with residual structural lesion suggestive of recurrence 49% of patients with potentially resectable pulmonary or hepatic metastases 49% of patients with potentially resectable pulmonary or hepatic metastases Scott AM, et al. J Nuc Med. 2008;49:1451-1457

17
63-yo with prostate ca, s/p prostatectomy Pre XRT colonoscopy revealed rectal mass Biopsy: rectal cancer Abd ceCT: no mets PET/CT for staging

23
ESOPHAGEAL CANCER Initial Diagnosis PET is more accurate than conventional imaging modalities PET is more accurate than conventional imaging modalities The overall incremental value of PET compared to CT with regard to staging accuracy was 14% The overall incremental value of PET compared to CT with regard to staging accuracy was 14% Kato H, et al. Cancer. 2005:103:148-156

24
Detection of Metastases: Detection of Metastases: Local Local –Sensitivity: 52% –Specificity: 84% Distant Distant –Sensitivity: 67% –Specificity: 97% Facey K, et al. NHS. R&D Programme: July 2004 Von Westreenen NH, et al. J Clin Oncol. 2004;22:3850-3812

25
65-yo M with history of laryngeal ca, s/p XRT Recent dx of esophageal ca ceCT: no mets PET/CT for staging

27
PANCREATIC CANCER; Differentiating Benign From Malignant Lesions PANCREATIC CANCER; Differentiating Benign From Malignant Lesions Orlando LA, et al. Aliment Pharmacol Ther. 2004;20:1063-1070 SensitivitySpecificity PET/CT 71% - 100% 53% - 100% ceCT 0% - 100%

28
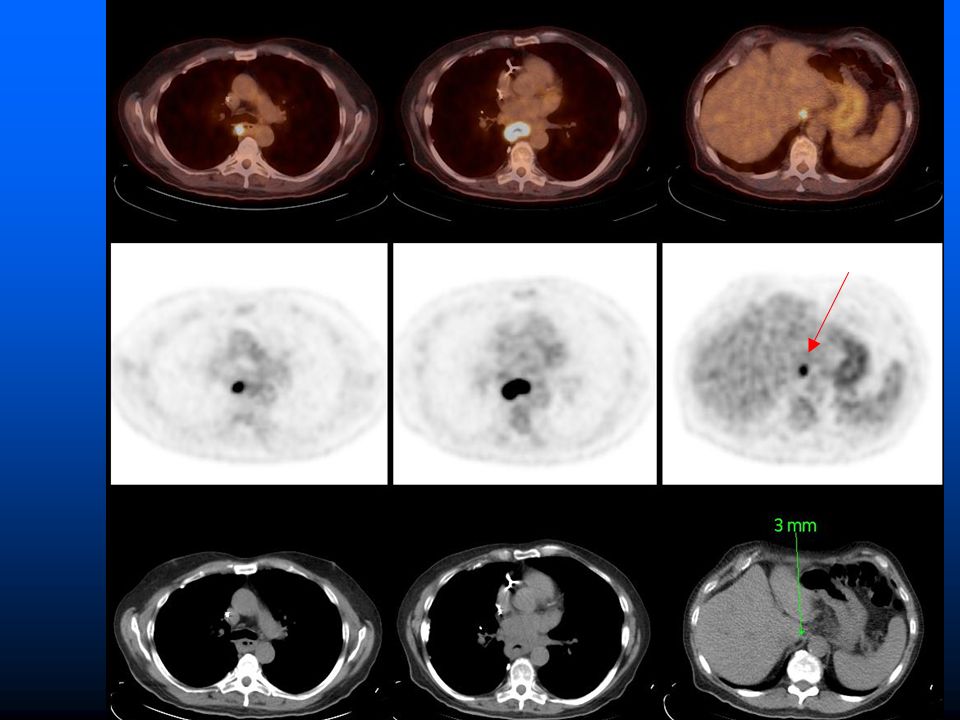
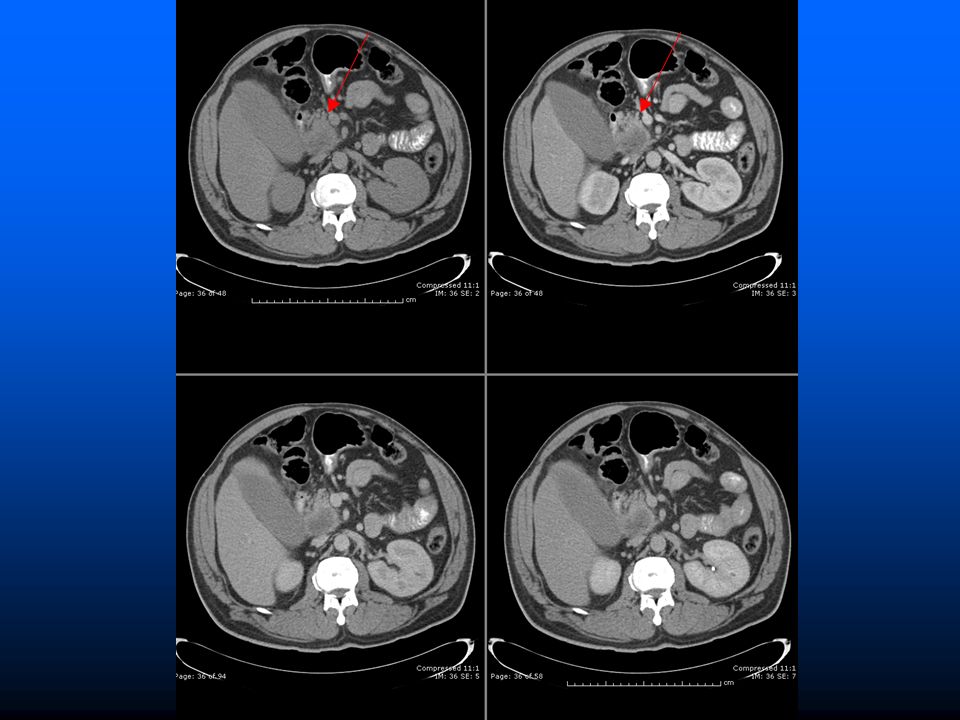
54-yo M with jaundice ceCT: pancreatic mass with no metastases Biopsy: pancreatic Ca PET/CT for staging

32
Male, age 66 Male, age 66 Former smoker Former smoker New LUL mass New LUL mass PET/CT for diagnosis and staging PET/CT for diagnosis and staging

41
ADVANCES New scanners New scanners New tracers New tracers Open coverage Open coverage

42
GEMINI TF PET/CT scanner with TruFlight technology

44
A B C D E “WHOLE-BODY” FOV VARIATIONS S Huston, M M Osman, SNM05

45
Added Value of True Whole-Body Over Limited Whole-Body FDG PET/CT in Cancer Patients

47
Results 20/ 500 (4%) of patients had new, previously unidentified cancerous lesions outside LWB FOV 20/ 500 (4%) of patients had new, previously unidentified cancerous lesions outside LWB FOV Detection of malignancy outside LWB resulted in changed in management in 13 (65%) and staging in 11 (55%) of those 20 patients Detection of malignancy outside LWB resulted in changed in management in 13 (65%) and staging in 11 (55%) of those 20 patients Of those 20, 5/500 (1%) patients had their only malignant lesion outside the LWB FOV Of those 20, 5/500 (1%) patients had their only malignant lesion outside the LWB FOV Osman MM, et al. SNM. 2006

48
PET/CT PET/MR

49
F-18 FLT PET

50
Imaging Gastric Cancer with PET and the Radiotracers 18 F-FLT and 18 F-FDG: A Comparative Analysis Hermann, et al. J Nuc Med. 2007;48:1945-1950

51
Sensitivity and Uptake of 18 F-FLT & 18 F-FDG in Gastric Cancer Imaging gastric cancer with proliferation marker 18 F-FLT is feasible 18 F-FLT was more sensitive than 18 F-FDG, especially in tumors presenting with no/low 18 F-FDG uptake

52
Detection of HCC Using 11 C-Choline: Comparison with 18 F-FDG ceCT 11 C-Choline 18 F-FDG

53
Detection of HCC: 18 C-Choline vs 18 F-FDG 11 C-Choline had a better detection rate compared to 18 F-FDG for a moderately differentiated HCC lesions but not for poorly differentiated lesions 18 F-FDG produce the opposite results 11 C-Choline is a potential tracer to complement 18 F- FDG in the detection of HCC lesions Yamamoto Y, et al. J Nuc Med. 2008;49:1245-1248

54
PET/CT: THE MOST IMPORTNAT CANCER IMAGING MODALITY NOPR 08 UPDATE >1500 facilities contributed data from >23,000 patients >1500 facilities contributed data from >23,000 patients FDG-PET changed treatment in 36.5% FDG-PET changed treatment in 36.5% JCO, published online March 24, 2008

Similar presentations





























 is well established Tomoharu T. et.>")

 in Colorectal Cancer Dr Chan Wai Keung Department of Surgery Ruttonjee and Tang Shiu Kin Hospitals.>")
 and Norma J. Nowak PhD (Cancer.>")

 Connects the body.>")

